Article Text

Abstract
Objectives: To evaluate the impact the National Service Framework (NSF) for coronary heart disease has had on emergency treatment and outcomes in patients presenting with acute coronary syndromes.
Design: Retrospective cohort study.
Setting: Coronary care units of two district general hospitals.
Results: Data from 3371 patients were recorded, 1993 patients in the 27 months before the introduction of the NSF and 1378 patients in the 24 months afterwards. After the introduction of the NSF in-hospital mortality was significantly reduced (95 patients (4.8%) v 43 (3.2%), p = 0.02). This was associated with a reduction in the development of Q wave myocardial infarction (40.6% v 33.3%, p < 0.0001) and in the incidence of left ventricular failure (15.9% v 12.3%, p = 0.003). The proportion of patients receiving thrombolysis increased (69.4% v 84.7%, p < 0.0001) with a decrease in the time taken to receive it (proportion thrombolysed within 20 minutes 12.1% v 26.6%, p < 0.0001). The prescription of β blockers (51.9% v 65.8%, p < 0.0001), angiotensin converting enzyme inhibitors (37% v 66.4%, p < 0.0001), and statins (55.2% v 72.7%, p < 0.0001) improved and the proportion of patients referred for invasive investigation increased (18.3% v 27.0%, p < 0.0001). Trend analysis showed that improvements in mortality and thrombolysis were directly associated with publication of the NSF, whereas the improvements seen in prescription of β blockers and statins were the continuation of pre-existing trends.
Conclusions: In the two years that followed publication of the NSF the initial treatment and outcome of patients presenting with acute coronary syndromes improved. Some of the improvements can be attributed to the NSF but others are continuations of pre-existing trends.
- ACE, angiotensin converting enzyme
- ACS, acute coronary syndromes
- CHD, coronary heart disease
- CI, confidence interval
- FRISC-II, Fragmin and fast revascularisation during instability in coronary artery disease
- HOPE, heart outcomes prevention evaluation
- LVF, left ventricular failure
- NSF, National Service Framework
- National Service Framework
- coronary heart disease
- acute coronary syndromes
- treatment
- outcomes
Statistics from Altmetric.com
- ACE, angiotensin converting enzyme
- ACS, acute coronary syndromes
- CHD, coronary heart disease
- CI, confidence interval
- FRISC-II, Fragmin and fast revascularisation during instability in coronary artery disease
- HOPE, heart outcomes prevention evaluation
- LVF, left ventricular failure
- NSF, National Service Framework
In March 2000 the introduction of the National Service Framework (NSF) for coronary heart disease (CHD) in the UK signalled that CHD was being made a government priority and indicated a goal to reduce death from CHD and related illnesses by 40% by the year 2010.1 Another goal was to standardise treatment regimens throughout the country to end geographical variations (or “postcode prescribing”) previously seen. The NSF has 12 standards addressing various aspects of CHD2 (see appendix available on the Heart website—www.heartjnl.com/supplemental).
One chapter of the NSF is dedicated to myocardial infarction and acute coronary syndromes (ACS). The broad aims are improving access to immediate paramedic care, speeding up administration of thrombolysis, increasing referral rates for invasive investigation, and improving prescribing rates of secondary prevention medications. The NSF has an associated timetable for achieving these aims and individual organisations are now being assessed and compared against standards. Although the standards put forward in the myocardial infarction and ACS chapter have an evidence based background, the effect of the publication of the NSF in implementing change is unknown. Recent evidence suggests that few hospitals have implemented standards that satisfy the requirements of the NSF.3
Since 1988 a dedicated computerised database has been used to record all admissions for ACS to two hospitals in the east end of London, serving a population of 700 000. Uniquely, this data collection was in place and in use before the publication of the NSF, allowing before versus after comparisons of treatment and outcomes. Data have been analysed to determine whether changes in treatment were the result of gradual pre-existing trends or whether there was a stepwise change attributable to the NSF.
METHODS
The study was based on patients with ACS or myocardial infarction admitted to the coronary care units of the Royal London and Newham General hospitals. The NSF came into operation on 1 April 2000. We compared data for patients admitted in the 27 months before the NSF implementation with data for patients admitted in the 21 months afterwards. Baseline clinical data were collected prospectively and stored electronically as previously described.4 Information recorded included patient demographic data, cardiac history, risk factors for CHD, ECG features (initial and subsequent), emergency treatment, complications, and further investigations arranged. Secondary prevention measures, discharge medications, and follow up arrangements were also documented. A diagnosis of diabetes was recorded if the patient required insulin, oral hypoglycaemic agents, or dietary sugar restriction. The diagnosis of left ventricular failure (LVF) was recorded for patients treated with diuretics with radiological evidence of interstitial or alveolar pulmonary oedema or symptoms of dyspnoea associated with basal inspiratory crepitations or a third heart sound.
Statistical methods
Patient characteristics and clinical outcomes before and after introduction of the NSF were compared by t tests or Mann-Whitney U tests for continuous variables and by χ2 or Fisher’s exact test for categorical variables. Logistic regression models were used to analyse trends in treatment over time. Patients were grouped into nine categories of three month according to their time of admission. This variable was fitted as a linear constant to determine overall trend and trends before and after the introduction of the NSF. An interaction term was fitted to assess any differences in trend before and after introduction of the NSF. Where no trend was observed before introduction of the NSF, rates before and after were directly compared. Where trends were observed, rates after the NSF was introduced were compared with those expected if the pre-NSF trend had continued.
RESULTS
Patient demographics
Table 1 lists patient characteristics. There was a small but significant increase in the number of patients of Asian ethnic origin after introduction of the NSF and in patients with a previous episode of ACS. Fewer patients after introduction of the NSF had a family history of ischaemic heart disease. Otherwise, differences in patient demographics, the treatment they were receiving, or the presenting ECG did not differ significantly.
Patient characteristics before and after the introduction of the National Service Framework (NSF) for coronary heart disease
Outcomes
In-hospital mortality fell after the introduction of the NSF (95 patients (4.8%) v 43 patients (3.2%), p = 0.02) (table 2). Similarly, the proportion of patients who subsequently developed Q waves on their ECG fell (790 patients (40.6%) v 430 patients (33.3%), p < 0.0001). The incidence of LVF fell in the cohort of patients admitted after introduction of the NSF (313 patients (15.9%) v 167 patients (12.3%), p = 0.003). The underlying mortality trend had been increasing before the NSF. The odds ratio (OR) for the six months before the NSF introduction was 1.22 (95% confidence interval (CI) 1.02 to 1.46). Adjusting for this trend, ethnicity, history of ACS, and family history of ischaemic heart disease gives an adjusted OR for mortality of 0.39 (95% CI 0.2 to 0.77, p = 0.007) and for ventricular fibrillation of 1.48 (95% CI 0.58 to 3.78, p = 0.42) (table 2). There was no underlying chronological trend in Q wave development or LVF. The adjusted ORs for these variables (adjusted for ethnicity, history of ACS, and family history of ischaemic heart disease) are 0.72 (95% CI 0.62 to 0.83, p < 0.0001) and 0.74 (95% CI 0.60 to 0.91, p = 0.004), respectively.
Clinical outcomes
Thrombolysis
Rates of treatment
Among patients eligible for thrombolysis, the proportion who received it increased (506 patients (69.4%) v 359 patients (84.7%), p < 0.0001). This difference remained significant after adjustment for ethnic group, previous ACS, family history of CHD, Q waves on the ECG, and presence of LVF (p < 0.0001). The number of patients who received thrombolysis increased progressively throughout the observational periods (fig 1). After introduction of the NSF, the rate of increase of patients receiving thrombolysis accelerated significantly when compared with the pre-NSF data (fig 1A, p = 0.03), indicating that this was not the continuation of a pre-existing trend.

Thrombolytic treatment before and after introduction of the National Service Framework (NSF) for coronary heart disease. (A) The trend with time for rate of treatment is not significant in the five groups before introduction of the NSF (p = 0.08) but afterwards the slope increases significantly (p = 0.03) and observed rates of treatment at every time point are significantly higher than predicted (p = 0.007), providing evidence that use of thrombolytic treatment increased after introduction of the NSF. (B) There is no evidence of any trend over time for rate of treatment within 20 minutes in the five groups before introduction of the NSF (p = 0.94). There is strong evidence that the percentage treated within 20 minutes has increased since 31 March 2000 (p < 0.0001).
Time to treatment
The proportion of patients who were thrombolysed within 20 minutes of arriving at hospital (the NSF target for door to needle time) increased from 55 patients (12.1%) to 91 patients (26.6%), p < 0.0001). After introduction of the NSF there was a significant stepwise increase in the proportion of patients being thrombolysed within 20 minutes (fig 1B, p < 0.0001).
Aspirin
Although the majority of patients were discharged receiving aspirin, there was a small but significant decrease in the proportion of these patients after introduction of the NSF (1787 patients (94.8%) v 1204 patients (90.9%), p < 0.0001).
β Blockers
Prescription of β blockers increased significantly after the NSF from 968 patients (51.9%) to 870 patients (65.8%) (p < 0.0001). The use of β blockers had been increasing progressively before introduction of the NSF and this trend continued after NSF (fig 2A), without a variation in rate.
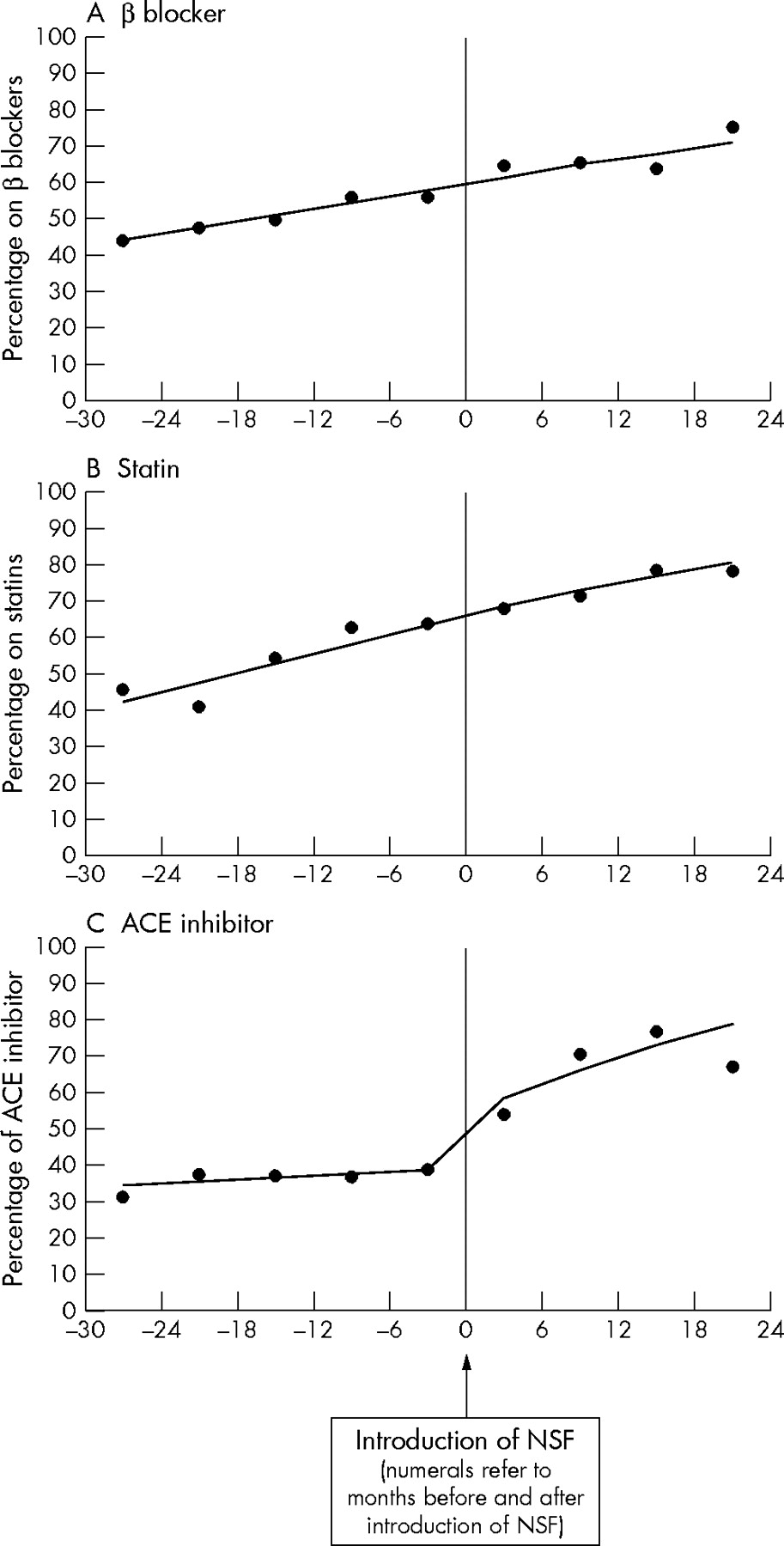
Rates of secondary prevention before and after introduction of the NSF. (A) Prescription of β lockers increased over time in the five groups before introduction of the NSF (p < 0.0001) but the rate of change did not increase thereafter. (B) Statin prescription increased over time in the five groups before introduction of the NSF (p < 0.0001) but the rate of change did not increase thereafter. (C) There is no evidence of a trend in prescription of angiotensin converting enzyme (ACE) inhibitors over time in the five groups before introduction of the NSF (p = 0.25) but a stepwise increase was recorded at the time the NSF was introduced (p = 0.003) and thereafter rate of prescription with time increased significantly (p < 0.0001).
Hydroxymethyl glutaryl coenzyme A reductase inhibitors (statins)
The proportion of patients being prescribed statins increased significantly after introduction of the NSF from 1024 patients (55.2%) to 956 patients (72.7%) (p < 0.0001) (table 3). The use of statins had been increasing steadily before the NSF was introduced and this continued in the post-NSF period with no significant difference in the rate of increase (fig 2B).
Comparison of treatment before versus after the introduction of NSF for coronary heart disease
Angiotensin converting enzyme inhibitors
The use of angiotensin converting enzyme (ACE) inhibitors significantly increased after introduction of the NSF from 690 patients (37%) to 879 patients (66.4%) (p < 0.0001). After introduction of the NSF the proportion of patients receiving ACE inhibitors increased stepwise (fig 2C).
Referral for urgent cardiac catheterisation
The number of patients who were transferred between hospitals for cardiac catheterisation before discharge increased after introduction of the NSF from 357 patients (18.3%) to 366 patients (27.0%) (p < 0.0001). After introduction of the NSF the proportion of patients undergoing cardiac catheterisation increased stepwise and has been increasing steadily since then (fig 3).

{kind=link}
{kind=link}
{kind=link}
Referral for in-hospital coronary angiography. There is no evidence of a trend over time in the five groups before introduction of the NSF (p = 0.19) but thereafter the rate of referral for cardiac catheterisation increased significantly with time (p < 0.0001).
DISCUSSION
This study shows an improvement in the outcome of patients with ACS admitted to the coronary care units of two east London hospitals between 1998 and 2002. In-hospital mortality was significantly reduced by one third from 4.8% to 3.2% (p = 0.02) and fewer patients developed Q wave infarction (40.6% to 33.3%, p < 0.0001). These improvements in outcome coincided with objective evidence of improvements in care as shown by an increase in thrombolysis rates among eligible patients, decreased time to thrombolysis, and increased prescribing of β blockers, ACE inhibitors, and statins. Referral for angiography and early revascularisation also increased.
Treatments and outcomes changed throughout health care systems due to several possible causes. Alterations in patient selection, resources, and staff can affect both treatment and prognosis of patients. Changes in the evidence base as a result of the publication of new studies may also have an impact on patient care. The implementation of guidelines is another potential source of change in practice and the NSF for CHD was introduced midway within our study period. To what extent was the NSF responsible for the improvements in patient care and outcome?
Selection criteria for admission of patients to the two coronary care units were not changed during the study period with the exception of the introduction of troponin assays, which were introduced gradually towards the end of the study period. Although there were minor changes in patient demographics, particularly an increase in the proportion of Asian patients, these changes would tend to make outcomes worse rather than better.5 Adjustment for these and the underlying mortality trend before the introduction of the NSF confirms the mortality benefit after the NSF was introduced (OR 0.39, 95% CI 0.20 to 0.77, p = 0.007). Funding, bed numbers, or numbers or grades of medical staff did not change significantly. The numbers of cardiac rehabilitation nurses increased slightly (one extra nurse at each hospital).
Our statistical analysis shows that improvements in care over the study period fell into two patterns. Some parameters changed gradually, with no evidence of a change around the NSF date (for example, β blocker and statin use), whereas others were changed stepwise, coinciding with the publication of the NSF (for example, mortality, rates of thrombolysis among those eligible, time to thrombolysis, ACE inhibitor use, and referral for early revascularisation). It therefore seems likely that improvements in the prescription of β blockers and statins were not directly influenced by the NSF guidelines and are the continuation of a pre-existing trend towards increased use of these drugs among patients with ACS.
Trend analysis shows that mortality was rising before the NSF was introduced (OR for the six months before NSF 1.22, 95% CI 1.02 to 1.46). Therefore, the stepwise improvement in mortality seen around the time of the NSF is likely attributable to the publication of the NSF. The NSF advises that the need for ACE inhibitors be reviewed after 4–6 weeks and that their use be limited to certain patients with symptomatic or objective left ventricular dysfunction. Therefore, publication of the HOPE (heart outcomes prevention evaluation)6 trial (published soon after the introduction of the NSF) may have been the driving force for the stepwise increase in use of ACE inhibitors, rather than the implementation of the NSF guidelines. Similarly, the beneficial effects of early revascularisation were reported by the FRISC-II (Fragmin and fast revascularisation during instability in coronary artery disease)7 study at around the same time. However, evidence for the use of thrombolysis as soon as possible after the onset of ST elevation myocardial infarction has been established for many years8 and this evidence base has not changed recently. It seems clear, therefore, that the improvements in rates and timing of thrombolysis were a result of the publication of the NSF. The ability of a hospital to organise effective rapid administration of thrombolytics is primarily the result of good organisation, and guidelines may be expected to have a particularly strong impact on organisational issues in patient care (see box).
Strategies to achieve measured improvements
-
General: setting up of multidisciplinary NSF committee who met regularly—These meetings were advertised in the form of emails, posters, etc. This raised awareness of the NSF among staff caring for patients with acute coronary syndromes (ACS).
-
Education—The NSF team organised teaching sessions for all new accident and emergency medical staff to recognise symptoms, signs, and ECG changes of patients presenting with ACS and to highlight the importance of prompt treatment of these patients. The role of health care assistants in accident and emergency was also expanded by training them to competently record ECGs.
-
Introduction of integrated care pathways (ICP) for patients presenting with chest pain—These ICPs outlined step by step the progress patients should have made and desired drug treatment with specific explanations required for any deviations from this.
-
Increased numbers and expanded role of cardiac rehabilitation nurses—Before the NSF was introduced, one hospital (RLH) had only one cardiac rehabilitation nurse who was there on rotation only. The grade varied from E to H. The other hospital (NGH) had two rehabilitation nurses, a team leader (grade I), and a G grade nurse. After introduction of the NSF, the RLH provided a dedicated cardiac rehabilitation sister (G grade) and another F grade nurse. A further F grade nurse was appointed at NGH.
-
Audit—The database in use in the coronary care units provided an instrument for audit. Door to needle times were audited regularly (three monthly) to assess compliance with the NSF. Practice was changed, as necessary, to improve care.
Study limitations
This was a retrospective registry analysis. In addition, the data are non-randomised because the NSF was universally applied in England and Wales and there was therefore no opportunity to compare centres with and without implementation of the standards. The non-randomised nature therefore raises the possibility that the changes observed were caused by unmeasured factors, since there was no control cohort.
Conclusions
The use of guidelines in cardiology remains controversial9 but there is evidence, particularly from the USA, that the implementation of audited guidelines has a positive impact on patient outcome.10,11 Although the improvements in care that we have shown still fall short of NSF targets, it is reassuring that these have still coincided with a decrease in mortality and morbidity. This suggests that the setting of clear, unambiguous targets contained within regularly audited guidelines is an effective means of effecting changes in health care. This may not be true of less clearly defined initiatives for altering practice such as clinical governance.12 We have observed improvements in patient care in the absence of any significant change in resources. It is possible to speculate that the combination of NSF guidelines with appropriate levels of funding might have had more profound effects on patient outcomes than those observed in this study.
Supplementary materials
Files in this Data Supplement:
- [view PDF] - Twelve Standards of NSF.
Footnotes
-
↵* Also the Department of Cardiology, Newham General Hospital
-
Published Online First 20 May 2005
-
Competing interests: There is no conflict of interests.