Article Text

Abstract
Objectives To define the epidemiology of adverse cardiovascular events among women with congenital heart disease (CHD) hospitalised for childbirth in the USA.
Design and setting The 1998–2007 Nationwide Inpatient Sample, an administrative dataset representative of overall US hospital admissions, was used to identify hospitalisations for delivery.
Main outcome measures Logistic regression was used to estimate ORs for cardiovascular outcomes (arrhythmia, heart failure, cerebrovascular accident, embolism, death or a combined outcome) for women with and without CHD. Covariates included age, number of medical comorbidites, pulmonary hypertension, hospital teaching status, insurance status and method of delivery.
Results Annual deliveries for women with CHD increased 34.9% from 1998 to 2007 compared with an increase of 21.3% in the general population. Women with CHD were more likely to sustain a cardiovascular event (4042/100 000 vs 278/100 000 deliveries, univariate OR 15.1, 95% CI 13.1 to 17.4, multivariable OR 8.4, 95% CI 7.0 to 10.0). Arrhythmia, the most common cardiovascular event, was more frequent among women with CHD (2637/100 000 vs 210/100 000, univariate OR 12.9, 95% CI 10.9 to 15.3, multivariable OR 8.3, 95% CI 6.7 to 10.1). Death occurred in 150/100 000 patients with CHD compared with 8.2/100 000 patients without CHD (multivariable OR 6.7, 95% CI 2.9 to 15.4). Complex CHD was associated with greater odds of having an adverse cardiovascular event than simple CHD (8158/100 000 vs 3166/100 000, multivariable OR 2.0, 95% CI 1.4 to 3.0).
Conclusions Maternal CHD is associated with a markedly increased risk of adverse cardiovascular events and death during admission for delivery.
- Congenital heart disease
- adults
- epidemiology
- pregnancy
- cesarean section
Statistics from Altmetric.com
Introduction
Advances in the care of congenital heart disease (CHD) have led to a growing population of adults living with the condition.1–3 As more people with CHD survive into their childbearing years, the challenges posed by pregnancy in women with CHD will be increasingly relevant.4–6
Although maternal death is uncommon, women with CHD have a significant risk of cardiovascular complications during pregnancy and childbirth.7–11 Pregnancy is associated with marked physiological changes including increased blood volume, heart rate and stroke volume, as well as decreased systemic vascular resistance. These physiological alterations are accompanied by structural modifications including increased ventricular diastolic dimensions, myocardial thickness and valvular cross-sectional area.12 13 While these changes are usually well tolerated, women with heart disease may be unable to compensate. Several risk factors for cardiovascular complications have been described including pulmonary arterial hypertension, left ventricular dysfunction, severe left-sided obstruction, mechanical valve replacement, cyanosis, prior arrhythmia or other cardiac events.14–19
Previous studies of the cardiovascular risk of pregnancy in CHD have focused on tertiary care populations and, with a rare exception,19 have been limited to a small number of specialised centres. Few studies have compared outcomes to a normal ‘control’ group.11 The frequency and characteristics of peripartum cardiovascular complications in women with CHD cared for outside major centres is therefore not well understood and little is known about the epidemiology of pregnancy and delivery among women with CHD at the population level. In this study we compared the occurrence of maternal cardiovascular events during childbirth among women with CHD and those without CHD using a nationally representative hospital discharge database.
Methods
We used the 1998–2007 Nationwide Inpatient Sample, the largest all-payer nationally representative hospital discharge database in the USA, to investigate the epidemiology of adverse cardiovascular outcomes during hospitalisation for childbirth among women with CHD compared with women without CHD. This database has been used to study other aspects of hospitalisations for CHD as well as pregnancy outcomes in other populations.3 20–22 Because this study used publicly available anonymous data, the Institutional Review Board of the Hospital of University of Pennsylvania granted an exemption. We identified women hospitalised with an International Classification of Diseases 9th Revision (ICD-9) code indicating vaginal delivery or caesarean section, as described previously.22 CHD was identified by ICD-9 code and divided into simple, unclassified and complex categories. To the extent possible with the available data, we defined simple diagnoses to correspond to those classified as simple CHD, while complex diagnoses correspond to those classified as moderate severity or great complexity in a previously described framework.2 Unclassified lesions included unspecified defect of septal closure (ICD-9 745.9), unspecified congenital cardiac anomaly (ICD-9 746.9), cardiac malposition (ICD-9 746.87) or unspecified congenital cardiovascular disease complicating pregnancy (ICD-9 648.5). Women with simple or unclassified lesions and concomitant complex lesions or pulmonary hypertension were categorised as complex in analyses unless specified.
The primary outcome was a combined outcome consisting of death, heart failure (ICD-9 428), arrhythmia (ICD-9 427), cerebrovascular accident including transient ischaemic attack (ICD-9 431, 433, 434, 435, 436), embolic events (ICD-9 415.1, 444, 445, 673) and unspecified cardiovascular complications of pregnancy (ICD-9 668.1). We also analysed the occurrence of each specific outcome and subcategories of arrhythmia. Rates are presented as number of events per 100 000 deliveries (n/100 000) or percentage of deliveries (n/100). Covariates included age in years, number of comorbidities,23 year, hospital teaching status, delivery method (caesarean or vaginal delivery), primary insurance and pulmonary hypertension (ICD-9 416).
Univariate and multivariable logistic regression, adjusting for the covariates above, were used to determine predictors of cardiovascular events. In addition, we performed univariate and multivariable linear regression to define predictors of length of stay (LOS) and total hospital charges. Logistic regression was performed to identify predictors of LOS >3 days and total hospital charges >$15 000, approximating the upper decile for these variables. Statistical analyses were performed using SAS for Windows Version 9.2. All analyses used provided sample weights and accounted for complex sample design and clustering by hospital.
Results
Demographic and clinical characteristics
There were approximately 42 602 106 deliveries in the USA between 1998 and 2007, and 71.6/100 000 (n=30 500) women admitted for delivery had CHD. The number of deliveries among women with CHD increased 34.9% over the study period compared with 21.3% in the general population. Patients with CHD were more likely to have at least one medical comorbidity (20.4% vs 12.0%, p<0.0001) and to deliver by caesarean section (32.2% vs 26.5%, p<0.0001; table 1).
Demographic and clinical variables for women with and without congenital heart disease admitted to a US hospital for delivery, 1998–2007
Simple CHD without coexisting pulmonary hypertension or complex CHD was present in 50.9% (n=15 539) of women with CHD while unclassified defects were present in 36.3% (n=11 068). An additional 2.5% (n=747) had a simple or unclassified diagnosis with concomitant pulmonary hypertension and were classified as complex CHD. A complex defect was present in 10.3% (n=3146) of women with CHD.
Maternal outcomes and CHD
The combined cardiovascular outcome occurred in 4042/100 000 deliveries in women with CHD and 278/100 000 deliveries in women without CHD, a difference which remained significant after adjusting for multiple covariates (OR 8.4, 95% CI 7.0 to 10.2; table 2 and figure 1).
Incidence of adverse maternal cardiovascular events for women with and without congenital heart disease*
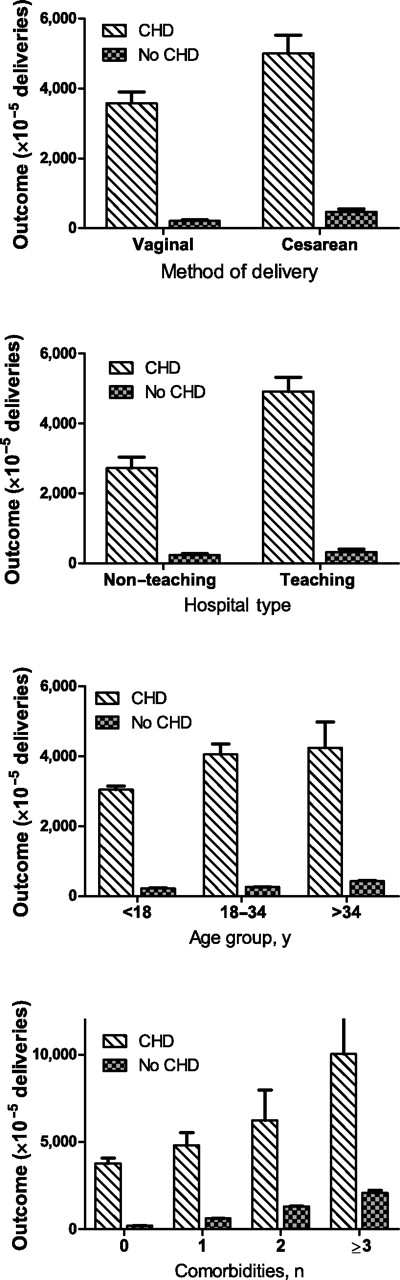
Incidence of adverse cardiovascular (CV) events for women with and without congenital heart disease (CHD) stratified by method of delivery, hospital type, age group and number of medical comorbidities. Data are for women having childbirth during hospitalisation. The analysis used sampling weights and accounted for the complex survey design. Error bars represent SE.
Women with CHD were more likely to die during admission for delivery (150/100 000 vs 8.4/100 000 deliveries, multivariable OR 6.7, 95% CI 2.9 to 15.4). Arrhythmia was the most common adverse cardiovascular event in both women with CHD and those without CHD (2637/100 000 vs 210/100 000 deliveries, multivariable OR 8.3, 95% CI 6.7 to 10.1). The incidence of heart failure was also higher among women with CHD (965/100 000 vs 34.5/100 000 deliveries), although this was in large part accounted for by the higher prevalence of pulmonary hypertension in this group (see below; multivariable OR 7.0, 95% CI 4.6 to 10.7; table 2). The odds of cerebrovascular accident were markedly increased in women with CHD (318/100 000 vs 5.4/100 000 deliveries, multivariable OR 41.6, 95% CI 25.8 to 67.1; table 2).
Adjusting for pulmonary hypertension in addition to the other covariates had a notable impact on the relationship of maternal CHD and the combined outcome (multivariable OR before and after adjusting for pulmonary hypertension 12.5→8.4, table 2). Pulmonary hypertension affected the relationship between CHD and heart failure (multivariable OR 20.4→7.0), death (multivariable OR 12.1→6.7) and embolism (multivariable OR 6.0→2.9) but had little appreciable effect on arrhythmia or cerebrovascular accident (table 2).
Women with CHD had longer average LOS (3.5 vs 2.6 days, univariate and multivariable p<0.0001) and higher hospital charges ($11 515 vs $8006, univariate and multivariable p<0.0001). LOS and total charges were greater among women with CHD after adjusting for confounders, as shown in figure 2 stratified by delivery method, hospital teaching status, age group and number of comorbidities.

(A) Mean length of stay (LOS) and (B) mean total hospital charges by presence or absence of congenital heart disease (CHD) stratified by method of delivery, hospital type, age group and number of medical comorbidities. Data are for women having childbirth during hospitalisation. The analysis used sampling weights and accounted for the complex survey design. Error bars represent SE.
Predictors of adverse outcome among women with CHD
Among women with CHD, independent predictors of the combined adverse cardiovascular outcome included pulmonary hypertension (multivariable OR 3.9, 95% CI 2.4 to 6.6), delivery at a teaching hospital (multivariable OR 1.8, 95% CI 1.3 to 2.3) and caesarean section (multivariable OR 1.3, 95% CI 1.0 to 1.7).
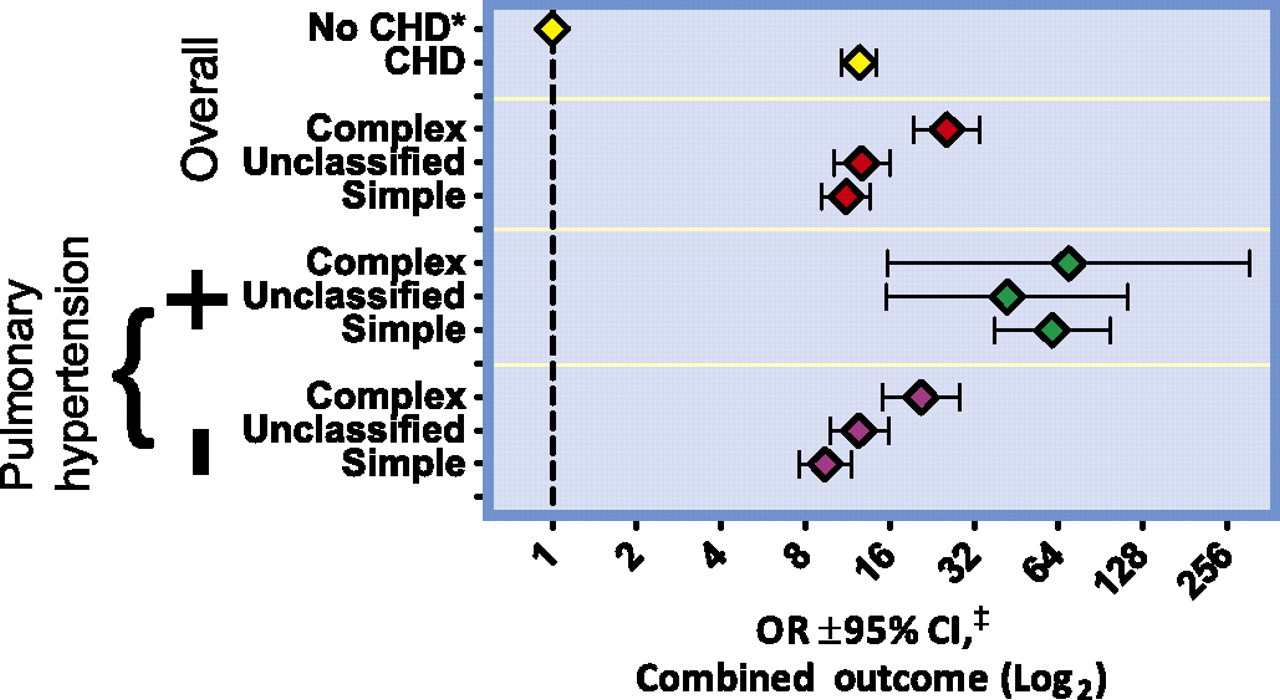
Women with simple, unclassified or complex CHD were more likely to sustain the combined cardiovascular outcome than those without CHD (figure 3). Pulmonary hypertension was associated with increased odds for an adverse cardiovascular event for CHD diagnoses of any complexity. The odds of sustaining the combined event were equivalent for women with pulmonary hypertension independent of CHD complexity (figure 3). Women with complex CHD had a higher frequency of cardiovascular complications than those with simple CHD (8158/100 000 vs 3166/100 000, univariate OR 2.7, 95% CI 2.0 to 3.6, multivariable OR 2.0, 95% CI 1.4 to 3.0). Excluding patients with pulmonary hypertension, adverse cardiovascular events occurred in 6439/100 000 women with complex CHD. The incidence of the combined cardiovascular outcome for patients with unclassified CHD was similar to simple CHD (3824/100 000 vs 3166/100 000, univariate OR 1.2, 95% CI 0.9 to 1.6, multivariable OR 1.4, 95% CI 0.99 to 1.9). Among women with concomitant pulmonary hypertension, those with only simple CHD sustained the combined outcome in 14 492/100 000 deliveries. The findings were similar for unclassified diagnoses (10 477/100 000) and complex diagnoses (16 130/100 000).

{kind=link}
{kind=link}
{kind=link}
Odds for adverse cardiovascular outcome by congenital heart disease (CHD) complexity and pulmonary hypertension status. ORs ±95% CIs of sustaining a maternal adverse cardiovascular outcome. The top half of the graph depicts the OR for women with CHD overall and for women with complex, unclassified and simple CHD. The bottom half of the figure shows results for each subcategory of CHD stratified by the presence and absence of pulmonary hypertension. Women without CHD (no CHD, shown in the first row) serve as the reference. ‡Multivariable model included age in years, number of Elixhauser comorbidities, year of hospitalisation, hospital teaching status, type of insurance and method of delivery (caesarean section or vaginal delivery). Multivariable results are presented for all groups except the subsets with pulmonary hypertension. Because of the smaller sample size, only univariate analysis could be performed for these subsets.
Women with complex CHD were more likely to have heart failure (3281/100 000 vs 559/100 000, univariate OR 6.0, 95% CI 3.3 to 11.1, multivariable OR 3.9, 95% CI 1.9 to 8.3) and arrhythmia (4194/100 000 vs 2077/100 000, univariate OR 2.1, 95% CI 1.3 to 3.2, multivariable OR 1.9, 95% CI 1.1 to 3.2) compared with those with simple CHD. Individual analyses for death, stroke and embolism are not reported, given the small absolute number of these events for CHD subgroups. Complex CHD was associated with greater odds of LOS >3 days(34.9±1.9% vs 22.2±0.8%, univariate OR 1.9, 95% CI 1.5 to 2.2, multivariable OR 1.4, 95% CI 1.1 to 1.8) and hospital charges >$15 000 (26.3±1.9% vs 14.9±0.9%, univariate OR 2.0, 95% CI 1.7 to 2.5, multivariable OR 1.5, 95% CI 1.2 to 2.0) than simple CHD.
Types of arrhythmia during hospitalisation for delivery
Supraventricular arrhythmias were the most common type of arrhythmia. Among the subset of women who sustained an arrhythmia during delivery, a supraventricular arrhythmia occurred in 75.0±3.5% and 78.4±0.4% of women with and without CHD, respectively, while a ventricular arrhythmia occurred in 13.8±2.8% and 6.0±0.2% of women with and without CHD, respectively. Premature beats without other supraventricular or ventricular arrhythmia were present in 8.2±2.2% and 10.9±0.3% of women with and without CHD, respectively. Unspecified arrhythmias occurred in 3.0±1.4% of women with CHD and 4.7±0.2% of women without CHD.
All types of arrhythmia were associated with longer LOS and higher changes (all univariate and multivariable p<0.0001). Adjusting for covariates, compared with women who did not have an arrhythmia, LOS was on average 3.4±0.4 days longer and total charges $34 102±2528 higher for those with ventricular arrhythmia, and LOS was on average 1.1±0.1 days longer and total charges $4515±248 higher for those with supraventricular arrhythmia. LOS was prolonged by only 0.7±0.1 days and total charges increased by $2875±348 for women with premature beats, and women with unspecified arrhythmia had LOS and total charges similar to the general population (↑0.3±0.1 days, p=0.03 and ↑$1438±815, p=0.08).
The absolute frequency of each type of arrhythmia per 100 000 deliveries is shown in table 3, along with univariate and multivariable OR stratified by the presence of CHD. Women with CHD had relatively higher ORs than women without CHD for more clinically important arrhythmias (supraventricular and ventricular arrhythmias) compared with premature beats and unspecified arrhythmias. Atrial flutter was rare in women without CHD (1.9/100 000 deliveries), while its incidence was markedly increased among women with CHD (198.8/100 000 deliveries). Sinus node dysfunction was also strikingly more common among women with CHD.
Incidence of arrhythmia by type for women with and without congenital heart disease*
Implications of adverse maternal cardiovascular outcomes
The combined outcome was associated with a higher rate of caesarean section (45.3% vs 26.3%, univariate OR 2.3, 95% CI 2.2 to 2.4, multivariable OR 2.0, 95% CI 1.9 to 2.0), increased LOS (5.0 vs 2.6 days, univariate and multivariable p<0.0001) and total charges ($20 850 vs $7960, univariate and multivariable p<0.0001). This was true for women without CHD (LOS 4.9 vs 2.6 days, p<0.0001; total charges $20 808 vs $7960, p<0.0001) and those with CHD (LOS 5.9 vs 3.4 days, p<0.0001; total charges $24 888 vs $10 935, p<0.0001). The combined outcome was associated with caesarean section among those with CHD (39.7% vs 31.7%, univariate OR 1.4, 95% CI 1.1 to 1.8, multivariable OR 1.3, 95% CI 1.0 to 1.7) and those without CHD (45.4% vs 26.3%, univariate OR 2.3, 95% CI 2.2 to 2.4, multivariable OR 2.0, 95% CI 1.9 to 2.0).
Discussion
Women with CHD are at increased risk of arrhythmia, heart failure, cerebrovascular events, other embolic events and death at the time of delivery.
We found that women with CHD are at markedly higher risk of death during childbirth, but deaths are still rare in this population, occurring in only 0.15%. It is unsurprising that contemporary studies of pregnancy in women with CHD, including at most several hundred pregnancies, have reported few maternal deaths.15 16 The largest meta-analysis to date of 2491 pregnancies did not report mortality data, noting that accurate estimates of such rare events require larger samples with less propensity to survivor bias.24 This highlights an advantage of large administrative databases. While uncommon, maternal mortality is the ‘ultimate’ adverse event and an accurate estimate of the risk of maternal mortality is crucial for pre-pregnancy counselling.
The most common adverse cardiovascular event among women with and without CHD is arrhythmia. Palpitations and premature beats, generally considered benign phenomena, are common among healthy pregnant women without structural heart disease.25 26 For this reason, we investigated the frequency of subtypes of arrhythmia. Women with CHD have increased odds for all types of arrhythmias. The difference is greater, however, among clinically important arrhythmias such as atrial fibrillation/flutter and ventricular tachycardia. The most marked increases in incidence for women with CHD are seen for atrial flutter and sinus node dysfunction, both rare in pregnant women without structural heart disease. A specific diagnosis was not available for a subset of arrhythmias. The modest associated increase in LOS and charges suggest that, for the most part, they are less clinically significant than specified supraventricular and ventricular arrhythmias. Data on the incidence of arrhythmias in women without CHD are in general agreement with rates of arrhythmia hospitalisation during pregnancy described from a single large centre (any arrhythmia 205/100 000 vs 166/100 000; paroxysmal supraventricular tachycardia 16.4/100 000 vs 24/100 000; ventricular tachycardia/fibrillation/arrest 12.6/100 000 vs 8/100 000; premature beats 26.2/100 000 vs 33/100 000), although we report a higher incidence of atrial fibrillation/flutter (∼16/100 000 vs 2/100 000).27
Our findings are consistent with previous research and provide further insights into the population risk for adverse maternal cardiovascular events at the time of delivery. Contemporary studies have estimated a maternal cardiovascular event rate of 11–25% during pregnancy and in the early postpartum period among women with heart disease.11 15 16 24 The timing of cardiac events during pregnancy among women with CHD is variable; one study reported that just over half of such events occurred before hospital admission for delivery and 3–4% of women sustained cardiac events between the onset of labour and hospital discharge.15 This is similar to our finding that approximately 4% of women with CHD have a cardiovascular event during admission for delivery. Our results are also in agreement with previous research describing arrhythmia and heart failure as the most common cardiac events during pregnancy among women with CHD.24 The reported absolute risk of these and other cardiovascular events, however, varies widely between studies. This is probably due to low sample sizes as well as heterogeneous referral populations and differing definitions.24 The importance of a cardiovascular event during pregnancy is not limited to the immediate outcome of that event, as highlighted by a recent report that women who sustain such an event during pregnancy are more than twice as likely to sustain a late cardiovascular event at 5 years of follow-up after pregnancy.28
We report a 34.9% increase in the number of women with CHD admitted for delivery between 1998 and 2007 compared with a 21.3% increase among the general population. As the number of women with CHD surviving to adolescence and adulthood increases, comprehensive care including appropriate congenital heart care assists these women in remaining healthy enough to consider childbearing.29 Pregnancy in women with CHD will therefore be an increasingly important clinical issue. A better understanding of obstetric and anaesthetic risk factors and complications will help guide the peripartum management of this population.
The classification of CHD into simple and complex categories has been described previously and is designed to identify patients who should be cared for by CHD specialists.2 3 This categorisation is not primarily based on the risk of adverse outcomes during pregnancy. The use of administrative data limits our ability to confidently categorise the severity of CHD. Appreciating this methodological limitation, we found women with complex CHD have an increased risk for adverse cardiovascular events, whether or not they had pulmonary hypertension.
This study highlights the risk posed by pulmonary hypertension in pregnancy. For example, we report that, among women with a diagnosis of simple CHD, 3.2% who do not have pulmonary hypertension have an adverse cardiovascular event compared with 14.4% of those with a simple lesion and pulmonary hypertension. Our data are consistent with the previously reported finding that pulmonary hypertension is associated with an especially high risk of adverse events during pregnancy. The maternal mortality for women with pulmonary arterial hypertension (a subset with elevated pulmonary vascular resistance and not equivalent to the broader diagnosis of pulmonary hypertension) related to pregnancy is estimated to be between 30% and 50%.14 30 As a result of this prohibitive risk, women with pulmonary arterial hypertension are generally counselled to avoid pregnancy and the number of such pregnancies is correspondingly low.11 15 16 About half of the women in our population had simple congenital lesions, while simple CHD with concomitant pulmonary hypertension accounted for only 2.5% of CHD pregnancies. In contrast, simple lesions without pulmonary hypertension were present in a large number of pregnancies. Our data generally support previous reports that women with simple defects usually tolerate pregnancy without complications. Nevertheless, we found that even women with simple lesions in the absence of pulmonary hypertension have an increased likelihood of sustaining an adverse cardiovascular event compared with the general population.
We also found that women with CHD are more likely to undergo delivery by caesarean section. The data available preclude an assessment of the indications or appropriateness of the finding, but this raises concern that the perceived cardiac complexity of these patients predisposes to caesarean delivery in the absence of another clinical indication. Independent of the increased rate of caesarean delivery, women with CHD had a longer average hospital stay and higher hospital charges. This increased resource utilisation has public policy and economic implications.
Limitations of the study
Our findings must be interpreted in light of methodological constraints. Large administrative databases have advantages as outlined above, but also pose limitations on the analysis. ICD-9 codes provide limited clinical detail and are of unknown validity for most diagnoses studied. The Nationwide Inpatient Sample does not provide clinical data beyond these codes, so we could not assess markers of disease severity such as functional status. There is no mechanism linking multiple admissions for a patient. To avoid overestimating incidence due to multiple admissions for the same category of cardiovascular event during a pregnancy, we limited our analysis to delivery. Since only a subset of cardiovascular events occurs at the time of delivery, our report probably underestimates the burden of adverse cardiovascular events. While general trends and correlates of adverse outcomes can be analysed, it is unclear if these represent true causal risk factors for given cardiovascular events.
Conclusion
Women with CHD are at increased risk for adverse cardiovascular outcomes and death. This risk is heightened in women with complex lesions and those with pulmonary hypertension. Women with CHD hospitalised for childbirth are more likely to undergo caesarean section. They also have longer hospital stays and incur higher hospital charges.
Acknowledgments
We are grateful to Fernando Baraona, Nancy Barker, Michelle Z Gurvitz, Eric V Krieger and Lilamarie Moko for insightful review of this manuscript.
References
Footnotes
Preliminary data were presented in abstract form at the American Heart Association Scientific Sessions, 2009.
Competing interests None.
Ethics approval The Institutional Review Board of the Hospital of University of Pennsylvania granted an exemption
Provenance and peer review Not commissioned; externally peer reviewed.