Article Text

Abstract
Objective To perform a patient-pooled analysis of a routine invasive versus a selective invasive strategy in elderly patients with non-ST segment elevation acute coronary syndrome.
Methods A meta-analysis was performed of patient-pooled data from the FRISC II–ICTUS–RITA-3 (FIR) studies. (Un)adjusted HRs were calculated by Cox regression, with adjustments for variables associated with age and outcomes. The main outcome was 5-year cardiovascular death or myocardial infarction (MI) following routine invasive versus selective invasive management.
Results Regarding the 5-year composite of cardiovascular death or MI, the routine invasive strategy was associated with a lower hazard in patients aged 65–74 years (HR 0.72, 95% CI 0.58 to 0.90) and those aged ≥75 years (HR 0.71, 95% CI 0.55 to 0.91), but not in those aged <65 years (HR 1.11, 95% CI 0.90 to 1.38), p=0.001 for interaction between treatment strategy and age. The interaction was driven by an excess of early MIs in patients <65 years of age; there was no heterogeneity between age groups concerning cardiovascular death. The benefits were smaller for women than for men (p=0.009 for interaction). After adjustment for other clinical risk factors the HRs remained similar.
Conclusion The current analysis of the FIR dataset shows that the long-term benefit of the routine invasive strategy over the selective invasive strategy is attenuated in younger patients aged <65 years and in women by the increased risk of early events which seem to have no consequences for long-term cardiovascular mortality. No other clinical risk factors were able to identify patients with differential responses to a routine invasive strategy.
Trial registration http://www.controlled-trials.com/ISRCTN82153174 (ICTUS), http://www.controlled-trials.com/ISRCTN07752711 (RITA-3).
- Non-ST-elevation acute coronary syndrome
- treatment strategy
- elderly
- gender
- stemi
- risk factors
- acute coronary syndrome
- reperfusion
- nstemi
- angina
- unstable
- cardiac remodelling
- risk stratification
- MRI
- acute ischaemic syndromes
Statistics from Altmetric.com
- Non-ST-elevation acute coronary syndrome
- treatment strategy
- elderly
- gender
- stemi
- risk factors
- acute coronary syndrome
- reperfusion
- nstemi
- angina
- unstable
- cardiac remodelling
- risk stratification
- MRI
- acute ischaemic syndromes
Introduction
The most recent guidelines for myocardial revascularisation recommend a routine invasive over a selective invasive approach in patients with non-ST segment elevation acute coronary syndrome (NSTE-ACS) at high risk for recurrent events.1 Although higher age has been identified as a non-modifiable risk factor in the most recent strategy trials,2–4 recommendations regarding treatment strategies are generally hampered by lower patient numbers with increasing age. This is especially true in patients aged ≥75 years,5 an underexposed subgroup that is often excluded from major trials. Limited randomised data are available, and previous studies comparing these strategies in elderly patients were performed before the availability of stents and glycoprotein IIb/IIIa inhibitors,6 7 so few data are available regarding more contemporary practice. In addition to the under-representation in clinical trials, registry data show that elderly patients with NSTE-ACS are less likely to undergo cardiac catheterisation and revascularisation, partly explained by an underestimation of risk by the physician.8
Besides the higher risk for recurrent events with older age, elderly patients are an important subgroup because of the heterogeneity in cognitive and physical functioning and more comorbidities which may alter the course after ACS.9 Moreover, elderly patients will constitute an important subgroup of patients, bearing in mind the gradually increasing age in the Western world.
In the current analysis of the FRISC II–ICTUS–RITA-3 (FIR) patient-pooled dataset, we evaluated long-term outcomes in a subgroup of elderly patients randomised to a routine invasive versus a selective invasive strategy. Moreover, we were able to compare these outcomes across other clinical categories of baseline risk.
Methods
Setting and data collection
The principal investigators (LW, RJdW, KAF) initiated the FIR collaborative analysis and a protocol was written which included the main prespecified analyses and a core set of variables. Investigators from the three trials provided individual patient data to form the FIR patient-pooled database, including variables on demographics, clinical history, risk factors for coronary artery disease, baseline ECG characteristics, laboratory results and 5-year clinical outcomes. Datasets from each trial were sent for merging to the coordinating Academic Medical Center in Amsterdam, The Netherlands. The merged database was checked for completeness and consistency by all three participating sites.
Study population and procedures
The details of the design of the FRISC II, ICTUS and RITA-3 trials have been described previously.2–4 The three trials compared a routine invasive strategy with a selective invasive strategy in patients with NSTE-ACS. Patients in the routine invasive group were scheduled to undergo early coronary angiography (within 24–48 h in the ICTUS trial, within 72 h in the RITA-3 trial), with subsequent revascularisation when appropriate. In the FRISC II trial the aim was to perform angiography and revascularisation, if appropriate, within 7 days. Coronary artery bypass grafting (CABG) was recommended in patients with severe left main stem or three-vessel disease. The selective invasive strategy consisted of initial medical treatment with coronary angiography and revascularisation only in the case of refractory angina despite optimal medical treatment (or in the case of haemodynamic or rhythmic instability in the ICTUS trial). In the FRISC II and ICTUS trials a predischarge ischaemia detection test was performed.
Age
Based on recommendations of the American Heart Association on Clinical Cardiology and the Society of Geriatric Cardiology, we formed the following three age study groups for our analysis: patients aged <65 years, patients aged 65–74 years and patients aged ≥75 years.9 Regarding the original trials, patients were eligible for the FRISC II trial if they were aged ≤75 years (or older unless revascularisation was deemed inappropriate) and for the ICTUS trial if they were aged between 18 and 80 years. No age-related exclusion criteria were defined in the RITA-3 trial.
Outcomes
The main outcomes for the current analysis were the 5-year composite outcome cardiovascular (CV) death or myocardial infarction (MI) and the individual components CV death and MI. CV death was defined as death from any cause unless an unequivocal non-cardiovascular cause could be established. The original definition of MI per trial was used because it was not possible to readjudicate individual events to accommodate a common definition. In the FRISC II trial, MI was defined by the occurrence of two of the following conventional criteria: typical chest pain, diagnostic ECG recording (new Q waves) and elevation of one cardiac biomarker above the upper limit of normal (ULN) with spontaneous MIs or elevation of one cardiac biomarker up to 1.5 the ULN with procedure-related MIs. In the RITA-3 trial, MI was defined as diagnostic ECG recording (new Q waves) or by the combination of a typical clinical event, ECG evidence of acute infarction and an elevation of one cardiac biomarker up to twice the ULN. In the ICTUS trial, MI was defined as myocardial necrosis in the setting of myocardial ischaemia. Myocardial necrosis was defined as an elevation of one cardiac biomarker above the ULN with spontaneous MIs, or three times the ULN in case of a procedure-related MI.10 We used both spontaneous and procedure-related MIs from all three studies in our current analysis.
Data concerning in-hospital major bleeding was available from the ICTUS and RITA-3 trials. Major bleeding was defined in the ICTUS trial as fatal bleeding, intracranial bleeding, a need for blood transfusion, a decrease of ≥3 mmol/l in haemoglobin levels and bleeding resulting in haemodynamic compromise. Major bleeding in the RITA-3 trial was defined as bleeding requiring surgical intervention or transfusion.
Statistical analysis
Cumulative event rates for unadjusted analyses were estimated by the Kaplan–Meier method and compared with the log-rank test. Follow-up for the composite outcome was censored at the actual date of last contact or at 5 years, whichever came first. The relation between treatment strategy and outcomes in the three age study groups were investigated in three sets of Cox proportional hazards models: (1) unadjusted models; (2) multivariable models with adjustment for the FIR risk score and study; and (3) multivariable models with adjustment for variables significantly related to age and outcomes. The FIR risk score indicates the 5-year risk for cardiovascular death or MI and is based on the following variables: age, BMI, diabetes, hypertension, previous MI and the presence of ST depression ≥0.1 mV.11 Interaction between age as a continuous variable and treatment strategy was assessed by including an interaction term in the Cox proportional hazards models. In prespecified analyses we analysed the relation between treatment strategy and outcomes in the three age study groups according to gender or baseline risk as indicated by the FIR risk score.11 Because we specifically wanted to examine the impact of age, the most important contributor to the FIR score, age was excluded from the risk score model and we redefined the low-risk, intermediate-risk and high-risk category cut-offs in patients assuming they received the selective invasive strategy that resulted in roughly one-third of outcomes per group. The proportional hazards assumption for all analyses was verified graphically; no relevant violations were observed.
Results
A total of 5467 patients with NSTE-ACS were included in the FIR dataset, of whom 2807 (51.3%) were aged <65 years, 1821 (33.3%) were aged 65–74 years and 839 (15.3%) were aged ≥75 years. The baseline characteristics are presented in table 1.
Baseline characteristics according to age study groups
Generally, with increasing age there were fewer men, an increased history of MI or revascularisation and a higher baseline risk profile as indicated by the FIR risk score (even after excluding age as one of the risk score components). Regarding risk factors for coronary artery disease, the older patients were less often smokers and had less hypercholesterolaemia, while diabetes mellitus and hypertension were more common.
Revascularisation over time
At 5-year follow-up, 74.1% of all patients underwent revascularisation by percutaneous coronary intervention or CABG in the routine invasive strategy group while 49.6% underwent revascularisation in the selective invasive strategy group. These revascularisation rates were, respectively, 80% and 53% in the FRISC II trial, 81% and 60% in the ICTUS trial and 62% and 39% in the RITA-3 trial. Figure 1 shows the cumulative revascularisation over time according to treatment strategy and age study group. No difference in revascularisation was observed between the three age groups in the routine invasive (p=0.33) or the selective invasive strategy groups (p=0.13). No heterogeneity was observed across studies. With increasing age, revascularisation was more often performed with CABG (30.5% in patients aged <65 years, 46.6% in those aged 65–74 years and 53.5% in those aged ≥75 years (p value for trend <0.001). Regarding PCI or both procedures on the same day, these percentages were 68.9%, 52.8%, 46.5% and 0.5%, 0.6% and 0.0%, respectively.

Timing of first coronary revascularisation according to age categories (p value by log-rank test).
Five-year outcomes
In the total population the cumulative event rates for the composite outcome CV death or MI and its individual components were 17.1% (907/5467), 7.4% (399/5467) and 12.3% (644/5467), respectively. For each of these outcomes, increasing 5-year event rates were observed across the <65 years, 65–74 years and ≥75 years age categories (overall log-rank p<0.001 for all outcomes). The cumulative event rates are shown in table 2.
Cumulative event rates for composite and individual outcomes of death or myocardial infarction at 5-year follow-up
Regarding treatment strategies, 15.9% of patients randomised to the routine invasive strategy experienced the composite outcome compared with 18.3% in the selective invasive strategy (HR 0.86, 95% CI 0.76 to 0.98, p=0.03). The HRs for the individual outcomes MI and cardiovascular mortality were 0.83 (95% CI 0.71 to 0.97, p=0.03) and 0.83 (95% CI 0.68 to 1.01, p=0.07), respectively.
Age
When comparing a routine invasive strategy with a selective invasive strategy with regard to the 5-year composite of CV death or MI, the routine invasive strategy was associated with a lower hazard in subjects aged 65–74 years (unadjusted HR 0.72, 95% CI 0.58 to 0.90, p=0.003) and those aged ≥75 years (unadjusted HR 0.71, 95% CI 0.55 to 0.91, p=0.007), but not in those aged <65 years (HR 1.11, 95% CI 0.90 to 1.38, p=0.33), p=0.001 for interaction between treatment strategy and age. This interaction was driven by a reduction in MI in patients aged 65–74 years (unadjusted HR 0.69, 95% CI 0.53 to 0.90, p=0.006) and those aged ≥75 years (unadjusted HR 0.60, 95% CI 0.43 to 0.83, p=0.002), while there was a numerical excess of MI in patients aged <65 years (10.2% in the routine invasive group vs 9.1% in the selective invasive group). Regarding CV death, no heterogeneity in differences were observed. The Kaplan–Meier curves (figure 2) indicated that the hazard in patients aged <65 years was caused by early MI. After adjustment for the FIR risk score and study or predictors for outcomes in multivariable Cox proportional hazards models, the HRs did not change materially. Unadjusted and adjusted HRs for cumulative event rates according to treatment strategy are shown in table 3.

(A) Kaplan–Meier curves for cardiovascular death or myocardial infarction after a routine invasive or selective invasive strategy according to age (p value by log-rank test). (B) Kaplan–Meier curves for cardiovascular death or myocardial infarction after a routine invasive or selective invasive strategy according to age (p value by log-rank test). CV, cardiovascular; MI, myocardial infarction; RI, routine invasive; SI, selective invasive.
Cumulative event rates for 5-year composite and individual outcomes according to treatment strategy and age
Gender
There was an interaction between treatment strategy and gender with a larger benefit in men than women (p=0.009 for interaction). In men the routine invasive strategy was associated with a lower hazard in those aged 65–74 years (unadjusted HR 0.60, 95% CI 0.47 to 0.79, p<0.001) and those aged ≥75 years (unadjusted HR 0.63, 95% CI 0.46 to 0.86, p=0.004), but not in men aged <65 years (HR 1.04, 95% CI 0.81 to 1.33, p=0.78), p<0.001 for interaction. The interaction was mainly driven by the individual component MI while there was no heterogeneity regarding mortality. No difference between the treatment strategies was observed in any of the age categories in women with regard to the composite or individual outcomes. The HRs for the composite outcome were 1.34 (95% CI 0.88 to 2.06, p=0.17) for women aged <65 years, 1.10 (95% CI 0.74 to 1.62, p=0.66) for those aged 65–74 years and 0.87 (95% CI 0.57 to 1.33, p=0.52) for women aged ≥75 years, p=0.83 for interaction. Figure 3 shows Kaplan–Meier curves for CV death or MI after a routine or selective invasive strategy according to age and gender, and indicates a larger early hazard and less long-term benefit in women than men regardless of age. After taking age and gender into account, other clinical risk factors did not interact with and were unable to further identify specific responses to a routine invasive strategy.

Kaplan–Meier curves for cardiovascular death or myocardial infarction after a routine invasive or selective invasive strategy according to age and gender (p value by log-rank test). CV, cardiovascular; MI, myocardial infarction; RI, routine invasive; SI, selective invasive.
Baseline risk profile
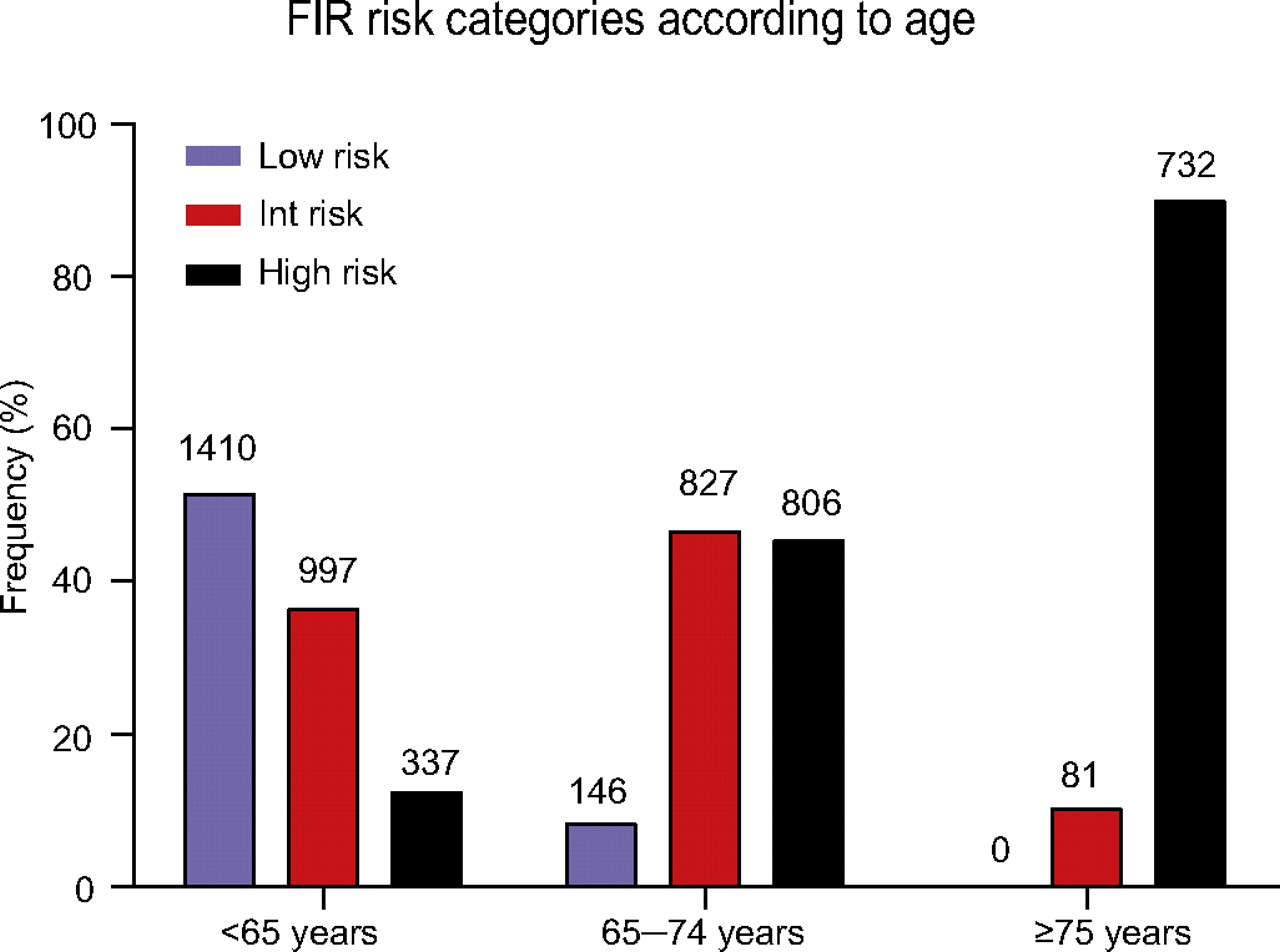
We compared the treatment strategies regarding CV death or MI according to FIR baseline risk (without age as a component) in the different age categories. The FIR low-risk group was redefined as a risk score of 0–2, the intermediate-risk as a score of 3–5 and the high-risk group as a score of ≥6. In the three age study groups no interaction was observed between treatment strategy and FIR baseline risk (p=0.41 for interaction the group aged <65 years, p=0.56 for interaction in the group aged 65–74 years and p=0.07 for interaction in the group aged ≥75 years). Figure 4 shows the distribution of patients in the redefined FIR risk groups according to age.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
FIR risk score categories according to age. FIR risk categories were redefined, age was excluded as a component of the risk score. FIR, FRISC II–ICTUS–RITA-3 trials.
Bleeding
Of 3006 patients with available data regarding initial in-hospital bleeding, bleeding rates were significantly higher in older patients: 1.7% (29 bleeds) in those aged <65 years, 2.2% (21 bleeds) in those aged 65–74 years and 6.1% (23 bleeds) in those aged ≥75 years (p<0.001 for trend).
In total there were 44 (2.9%) in-hospital bleeds in the routine invasive group and 29 (1.9%) in the selective invasive group (p=0.069). The number of bleeds was higher with the routine invasive strategy in each of the three age categories, although numbers were small and p values all >0.1.
Discussion
The current meta-analysis of the FRISC II–ICTUS–RITA-3 trials shows that the long-term reduction in the composite of CV death or MI with the routine invasive strategy compared with a selective invasive strategy is mainly seen in patients aged ≥65 years. In younger patients aged <65 years this effect is attenuated by an excess of early MI. However, these events did not have consequences for effects on survival which showed no heterogeneity in relation to age. The early hazards were larger and the long-term benefits smaller in women in all age groups. Other clinical risk factors at baseline were not able to better identify specific responses to a routine invasive treatment strategy.
Previous treatment strategy trials
The TIMI IIIB and VANQWISH trials were performed in the early 1990s, before routine availability of coronary stents and glycoprotein IIb/IIIa inhibitors, and compared an early invasive strategy with an early conservative strategy.6 7 Regarding outcomes in elderly patients, these trials yielded conflicting results. While the overall TIMI IIIB trial showed equivalence between treatment strategies, a reduction in 1-year death or MI was observed in elderly patients (≥65 years). In contrast, the VANQWISH trial suggested a potential hazard of early invasive treatment in patients aged >60 years. This was partly explained because of a high 30-day event rate in high-risk patients undergoing CABG.
In one of the more contemporary studies, the TACTICS-TIMI 18, patients were randomised to an early invasive or conservative treatment strategy.5 At 6-month follow-up a reduction in death or MI was observed with the early invasive strategy in patients aged ≥65 years. Outcomes were similar in patients aged <65 years. Although the benefit was also observed in patients aged >75 years, this was accompanied by significantly increased major bleeding. This was probably the result of the combination of the invasive procedure and use of glycoprotein IIb/IIIa inhibitors. Glycoprotein IIb/IIIa inhibitors were used in 94% of the PCIs during initial hospitalisation in the ICTUS trial. In the RITA-3 trial glycoprotein inhibitors were used in about 25% of the PCI procedures. Our current results are in line with the TACTICS-TIMI 18 trial and extend the evidence with sustained benefit at long-term follow-up. Although in-hospital major bleeding was numerically higher with the routine invasive strategy than with the selective invasive strategy, the number of bleeds was small and the evidence for a difference was weak.
The long-term results of the FRISC II and RITA-3 trials showed a benefit of the routine invasive strategy over a selective invasive strategy.12 13 This reduction in death and MI increased with increasing baseline risk. While the assessment of baseline risk was based on multiple clinical factors collected at baseline, age was one of the strongest contributors to baseline risk.13 14 Also, in the ICTUS trial, increasing event rates were observed with higher baseline risk profiles but no difference was observed between treatment strategies in any of the risk strata.10 This heterogeneity between the three pooled trials has also attenuated the reduction in both mortality and MI as observed in the FRISC II and RITA-3 trials, with less crossover to revascularisation.
Gender
Taking gender into account, the benefit of the routine invasive strategy was mainly observed in men, as reported in previous meta-analyses.15 16 One of these analyses showed a benefit of the routine invasive strategy in female high-risk patients.15 In our current analysis women aged ≥75 years were few, so results in this higher risk group should be interpreted with caution. The observed gender difference was mainly driven by the FRISC II and RITA-3 trials, which have previously shown that a reduction in death and MI was mainly observed in male patients.17 18 No clear gender differences were observed in the ICTUS trial.10
Baseline risk profile
A previous report on NSTE-ACS registry data discussed the risk-treatment paradox, showing that older higher-risk patients are managed more conservatively.8 One possible explanation is the underestimation of the risk profile of elderly patients by physicians. The authors showed that the baseline risk profile, as indicated by the GRACE risk score, was significantly higher in older patients. This is corroborated by our current results, showing higher FIR risk scores with increasing age. Thus, the reason for undertreatment of elderly patients might be an overestimation of the procedural risk and an underestimation of the long-term benefits in elderly patients, with more comorbidities indicating higher risk. However, the present results show that additional clinical risk factors, beyond age and eventually gender, have no significant impact on the long-term benefits of a routine invasive treatment strategy. Accordingly, these risk factors do not seem useful but rather might be misleading if used for selection of patients for a routine invasive strategy. Although laboratory parameters might assist in this process, these were not completely available in the FIR database. Finally, we have to keep in mind that there is a preferential recruitment of lower-risk patients into clinical trials,19 with a possibility that higher risk elderly patients were not recruited to the FIR trials.
FIR risk score and treatment strategy
We have previously shown that the FIR integer risk score, which reflects the baseline risk profile, can be used to identify patients who have the largest benefit of the routine invasive strategy.11 The current results show that the main driver of the FIR baseline risk profile is age, and that no other FIR risk score factors identify responders to the routine invasive strategy. Gender, which is not a component of the FIR risk score, did assist in the identification of responders. In conclusion, although the FIR risk score adequately discriminates patients at low, intermediate or high risk for long-term outcomes, age and gender are the most important factors in the triage of patients to a routine or selective invasive strategy in the FIR dataset. As mentioned above, laboratory parameters might assist in the selection of treatment strategies.
Limitations of the study
Several limitations of the current analysis are worthy of note. First, there was heterogeneity between trials regarding the revascularisation rates and timing of revascularisation in the routine invasive and selective invasive strategies. The high revascularisation rate in the selective invasive arm of the ICTUS trial will have attenuated the benefits of a routine invasive strategy.10 Second, the outcome MI was composed of all spontaneous and procedure-related MIs from the FRISC II, ICTUS and RITA-3 trials, and a uniform definition could not be achieved. The use of a uniform definition of MI would have allowed a more accurate assessment of treatment effects on the clinical outcomes spontaneous and procedure-related MI.20
Conclusion
The current analysis of the FIR patient-pooled dataset indicates that the long-term benefit of the routine invasive strategy over the selective invasive strategy is attenuated in younger patients aged <65 years and in women because of the raised risk of early events. However, these events seem to have no consequences for mortality. No other clinical risk factors were able to identify patients with differential responses to a routine invasive strategy.
Acknowledgments
We would like to thank all investigators from the FRISC II, ICTUS and RITA-3 trials and all patients participating in these trials.
References
Footnotes
See Editorial, p 173
Competing interests The collaboration and meta-analysis were conducted using resources from the host institutions for the respective studies (KAAF is supported by the British Heart Foundation; LW is supported by the Swedish Heart Foundation) and from the London School of Hygiene and Tropical Medicine. KAAF has received grants and honoraria from Sanofi-Aventis/Bristol-Myers Squibb, GlaxoSmithKline, Lilly and AstraZeneca. SJP has consulted for The Medicines Company and has served on a Boston Scientific-sponsored Data Monitoring Committee.
Ethics approval British, Dutch and Swedish local ethics committees approved the original studies.
Provenance and peer review Not commissioned; externally peer reviewed.