Article Text

Abstract
Objective The Fontan operation is a staged palliation for complex congenital heart disease and single ventricle physiology. Perioperative survivors of the Fontan operation experience long-term cardiac complications, including death. Liver and renal dysfunction are reported in these patients and have a direct effect on morbidity and mortality. This study aims to investigate whether the Model for End-stage Liver Disease eXcluding INR score (function of creatinine and total bilirubin, MELD-XI) predicts risk for cardiac mortality or transplantation in patients with Fontan circulation.
Design and setting Retrospective, single-centre study. Time of first evaluation was the time of the earliest available MELD-XI score measurement, and follow-up was terminated by a cardiac event or by the last clinical evaluation.
Patients Patients surviving after Fontan surgery and evaluated at Boston Children's Hospital between 1993 and 2008.
Main outcome measure Composite endpoint of sudden death, death from congestive heart failure or cardiac transplantation.
Results The MELD-XI score was calculated as MELD-XI=11.76(loge creatinine)+5.112(loge total bilirubin)+9.44. Ninety-six patients were included (52 male, median age 26 years). After a mean follow-up period of 5.7 years, 18 patients (19%) experienced the composite end point. Baseline MELD-XI score was independently and directly related to the incidence of the composite endpoint (HR for high MELD-XI score group of 7.76, 95% CI 2.05 to 29.33, p=0.008).
Conclusions Fontan patients with a higher MELD-XI score have shorter freedom from sudden cardiac death, death from congestive heart failure and cardiac transplantation.
- Congenital Heart Disease
- Heart Failure
Statistics from Altmetric.com
Background
The Fontan operation is performed as the anticipated culmination of staged surgical palliation in patients with complex congenital heart disease and single ventricle physiology.1 ,2 The original surgical approach has undergone multiple modifications, and the total cavopulmonary anastomosis, which combines a bidirectional Glenn shunt with rerouting of the inferior vena caval flow to the pulmonary artery via an intra-atrial baffle or extracardiac conduit, has now become the preferred technique.
Disadvantages of the resulting Fontan physiology include chronic venous hypertension and a limited cardiac output.3 It is now recognised that perioperative survivors of the Fontan operation almost invariably experience increasing long-term cardiac morbidity and mortality. Usual cardiac modalities of death include arrhythmias, congestive heart failure or thromboembolic events.4
In an effort to identify predictors of long-term morbidity and mortality, clinical and laboratory markers of multiple organ dysfunction have been sought in patients surviving with congenital heart disease.5 Patients living with Fontan circulation, in particular, are prone to chronic renal insufficiency, hepatic fibrosis and cardiac cirrhosis. These pathological changes seem to correlate with pre-Fontan morbidity, chronic cyanosis and chronic elevation of systemic venous pressures after Fontan surgery.6 ,7
Recent studies have investigated the utility of the Model for End-Stage Liver Disease (MELD) score as a potential predictor of poor outcomes in patients with heart disease.8 ,9 A logarithmic function of creatinine, total bilirubin and International Hospitalized Ratio (INR), the MELD score in many ways serves as a simple marker of multiple organ dysfunction. Originally developed to predict mortality in patients being considered for transjugular intrahepatic portosystemic shunt placement, the MELD score has been demonstrated to correlate strongly with early pretransplant waiting list mortality and is now used in the USA to prioritise organ allocation for liver transplantation.10 ,11
One limitation of the MELD score is that in patients receiving warfarin, the INR becomes dissociated from liver synthetic function, largely nullifying the prognostic significance of the score. In 2007, a modification of the MELD score eXcluding INR (MELD-XI score) was validated against the original MELD score. The MELD-XI score, although it omits INR from the calculation, is nearly as accurate in predicting short-term survival in patients with liver cirrhosis.12 Our study aims to investigate the hypothesis that the MELD-XI score would predict increased risk for cardiac mortality or transplantation in patients with Fontan circulation.
Methods
Population
Patients surviving after Fontan surgery and evaluated in the outpatient cardiology clinic at Boston Children's Hospital between 1993 and 2008, were considered for enrolment. Eligible individuals were identified from two previously published cohorts of patients with Fontan circulation.4 ,13 Patients were included if at least one set of creatinine and total bilirubin measurements was obtained within a 7-day period during outpatient follow-up. In patients with multiple such measurements allowing for calculation of the MELD-XI score, multiple data points were collected. Patients were not excluded on the basis of pre-existing renal or hepatic diseases.
Demographics and clinical data including primary congenital defect, surgical details and results of cardiac catheterisation before the Fontan procedure and during the follow-up period were collected through search and review of departmental and hospital electronic health records and reports.
The comparison group consisted of a group of adult patients evaluated during the same study period in the Partners Healthcare system (Brigham and Women's Hospital and Massachusetts General Hospital, Boston, Massachusetts, USA) without cardiac disease and with an established diagnosis of liver cirrhosis due to chronic hepatitis C infection.
MELD-XI score calculation
The MELD-XI score was calculated using the previously described formula MELD-XI=11.76(loge creatinine)+5.112(loge total bilirubin)+9.44.12 Creatinine and total bilirubin were measured as mg/dl. As previously described, creatinine and total bilirubin values <1 mg/dl were set to 1 mg/dl for the purpose of calculating MELD-XI score. Conversely, creatinine was set at 4 mg/dl for patients with measured creatinine values >4 mg/dl or in those receiving renal replacement therapy.
Endpoint and definition
A composite endpoint of sudden death, death from congestive heart failure or cardiac transplantation was defined. Sudden death was defined as death occurring within 1 h of symptom onset in a patient with otherwise stable clinical condition. Death from congestive heart failure was defined as death occurring in the setting of long-standing cardiac decompensation with progressive clinical deterioration requiring escalating diuretic dose or inhospital management with inotropic/vasopressive support.
Cyanosis was defined as the presence of resting systemic oxygen saturation less than 90%.
Patients were classified as being treated with a medication if they were taking it at the time of baseline MELD-XI score assessment.
Study design
In this retrospective, cohort study, the time of first evaluation was considered to be the date of the earliest available MELD-XI score measurement. In cases where creatinine and total bilirubin were measured on different days, the earlier date was considered the date of MELD-XI score measurement. The follow-up was terminated by the date of the composite endpoint or by the date of last clinical evaluation in the outpatient clinic in patients who did not experience the composite endpoint during the follow-up period. This study was compliant with the Health Insurance Portability and Accountability Act, and a waiver of informed consent was approved by the institutional review boards of Boston Children's Hospital and Brigham and Women's Hospital.
Statistical analysis
Patient characteristics were described with median (range) and counts and percentages. A Wilcoxon rank sum test was used to compare the distribution of MELD-XI scores between the Fontan and hepatitis C groups. Recursive partitioning was used to identify the cut-off points that best categorised initial MELD-XI score, creatinine and total bilirubin in terms of predicting the development of the composite endpoint. Log-rank tests were used to compare Kaplan-Meier survival curves across these groups. Univariate and multivariate Cox proportional hazards models were used to identify baseline patient and clinical characteristics independently associated with time to the composite outcome. In order to estimate the effect of ‘change’ in MELD-XI score over time on the development of the composite endpoint, a Cox proportional hazards model with a time-varying covariate of the difference in MELD-XI score between the two most recent measurements was fit in the subset of patients with ≥ two MELD-XI measurements. In order to adjust for the variation in timing of MELD-XI measurements across patients, an additional model was fit which included time since last MELD-XI measurement as a time-dependent variable. In all tests, statistical significance was achieved with a two-sided p value<0.05. Statistical analyses were performed with SAS software, 9.2 of the SAS System for Windows (SAS Institute, Cary, North Carolina, USA) and S-plus, 8.0 (TIBCO Software, Palo Alto, California, USA).
Results
Baseline characteristics
Of the 383 patients included in the original cohorts, 96 matched the inclusion and exclusion criteria. Table 1 summarises the baseline characteristics of the study population. Seventy per cent of patients had a morphological left ventricle serving as the systemic ventricle, 19% had a systemic right ventricle and 11% had right and left ventricular heart with univentricular physiology. No patient was prescribed or was known to be using advanced pulmonary arterial hypertension or pulmonary vasodilator therapy at the time of, or within 6 months of, baseline MELD-XI score assessment.
Baseline characteristics of the study population
The Fontan operation was performed using a lateral tunnel approach in 42% of the patients; 45% of the cohort received a modified classic Fontan with right atrial-to-pulmonary artery anastomosis. Nine patients with tricuspid atresia and a right ventricular outflow chamber had a right atrium-to-right ventricular conduit, while in three patients an extracardiac conduit was used to complete the cavopulmonary anastomosis.
A serological profile for hepatitis B and C infections was available in 29 patients (30%). Of those, 21 (22%) had no evidence of chronic infection from hepatitis B or hepatitis C viruses; eight (8%) had chronic hepatitis C infection.
Forty-five patients (48%) experienced a non-fatal complication of Fontan circulation prior to the first MELD-XI score evaluation. Ten patients (11%) developed protein-losing enteropathy (PLE). Twenty-three patients (24%) had evidence of thrombus within the Fontan pathway. In 13 patients the diagnosis of thrombus within the Fontan pathway was made by transoesophageal echocardiography; in three the diagnostic modality was cardiac MRI and in one case the diagnosis was made incidentally during cardiac catheterisation. In the remaining six cases, the patient had a reported diagnosis of thrombus within the Fontan pathway without a diagnostic study available for review. Only two and five patients, respectively, were on aspirin or warfarin at the time of the diagnosis of thrombus within the Fontan pathway. Ten patients (11%) had non-fatal stroke, five of whom also had evidence of thrombus within the Fontan pathway.
No significant difference is found between the frequency distributions of MELD-XI scores between patients with Fontan circulation compared with the group of patients with established cirrhosis due to chronic hepatitis C infection (see online supplementary material figure S1). The two populations had clinically similar median (range) MELD-XI scores (9.4 (9.4–26.2) vs 10.8 (9.4–30.6), p=0.02).
MELD-XI score was higher in patients who presented with cyanosis at the time of the first MELD-XI assessment (14±5.8 vs 11.9±3.3, p=0.03). There was no significant association between baseline MELD-XI scores and age at the MELD-XI score assessment (R2=0.09, p=0.004) or time from Fontan surgery (R2=0.006, p=0.5). There was no significant difference between baseline MELD-XI scores in patients with classic right atrium-to-pulmonary artery Fontan and those with lateral tunnel Fontan (12.1±3.6 vs 12.6±5, p>0.5).
Interestingly, patients who were on renin-angiotensin system inhibition at the time of baseline MELD-XI score assessment presented significant lower baseline MELD-XI scores compared with the rest of the cohort (11.7±6 vs 13.8±3, p=0.02). Patients who were receiving warfarin at the time of baseline MELD-XI score assessment presented slightly higher values of MELD-XI score than patients who were not on warfarin therapy (13.3±5.1 vs 11.5±2.9, p=0.03).
No difference in baseline MELD-XI score distribution was found in patients who experienced non-fatal complication of Fontan circulation before the MELD-XI score assessment, such as PLE, thrombus formation within the Fontan pathway or stroke compared with the rest of the cohort (12.4±4.1 vs 12.5±4.6, p=0.9).
Considering only the 29 patients with known hepatitis serology, we compared the baseline MELD-XI score between patients with known chronic infection by hepatitis C virus with patients with negative serology. No significant difference was found between those two groups of patients (10.9±2.6 vs 12.6±5.5, p=0.6, see online supplementary material figure S2).
Relation between MELD-XI score and cardiac haemodynamics
There was no significant correlation between pre-Fontan cardiac index and either baseline MELD-XI score or last MELD-XI score during follow-up (R2=0.01, p=0.25; R2=0.01, p=0.4 respectively). Similarly, no relation has been identified between pre-Fontan systemic venous pressure and baseline MELD-XI score or last MELD-XI score during follow-up (R2=0.009, p=0.4; R2=0.02, p=0.4 respectively). Eighty-six patients underwent cardiac catheterisation after Fontan surgery. Of those, 50 patients had their haemodynamic assessment within 1 year from the baseline MELD-XI score assessment. In this subgroup of patients no significant association was identified between cardiac index and baseline MELD-XI score values (R2=0.02, p=0.3) or systemic venous pressure (Fontan pressure) and baseline MELD-XI score (R2=0.03, p=0.20).
Relation between baseline MELD-XI score and cardiac mortality or transplantation
During the mean follow-up period of 5.7 years, 18 patients (19%) experienced the composite endpoint of sudden death, death from congestive heart failure or cardiac transplantation, yielding a crude composite endpoint rate of 3.2%/year. Nine patients died from refractory congestive heart failure, five patients died suddenly and four patients underwent cardiac transplantation. One hepatitis C patient, with refractory congestive heart failure and cardiohepatorenal syndrome, succumbed to fungal peritonitis in the setting of large volume ascites and liver cirrhosis. No other complications of liver cirrhosis were detected during follow-up.
The results of the univariate analysis of the relationship between clinical variables and mortality are reported in table 2. There was a significant association between the composite endpoint and therapy with warfarin or aspirin (HR 0.21, 95% CI 0.06 to 0.76, p=0.02) or therapy with diuretics (HR 12.89, 95% CI 1.72 to 96.88, p=0.01).
Risk factors for composite endpoint
Recursive partitioning identified the categories of baseline MELD-XI score best able to predict the composite endpoint. Accordingly, the study population was divided into three subgroups (below 11, 11 to 18, and above 18). Forty-seven patients had a baseline MELD-XI score below 11; 38 patients had a baseline score of 11 to 18; and 11 patients had a baseline score above 18 (see online supplementary material figure S3). Univariate analysis of the relationship between baseline MELD-XI score and the composite endpoint is shown in table 2, using the lowest MELD-XI score as the reference group.
Kaplan-Meier estimates of the proportion of patients remaining free of the composite endpoint in each of the three MELD-XI score subgroups are shown in figure 1. The time from first MELD-XI measurement to composite endpoint occurrence in 25% of patients was more than 16 years in patients with a baseline MELD-XI score less than 11, almost 5 years in patients with an intermediate MELD-XI score of 11 to 18, and 54 days in patients with a baseline MELD-XI score above 18.
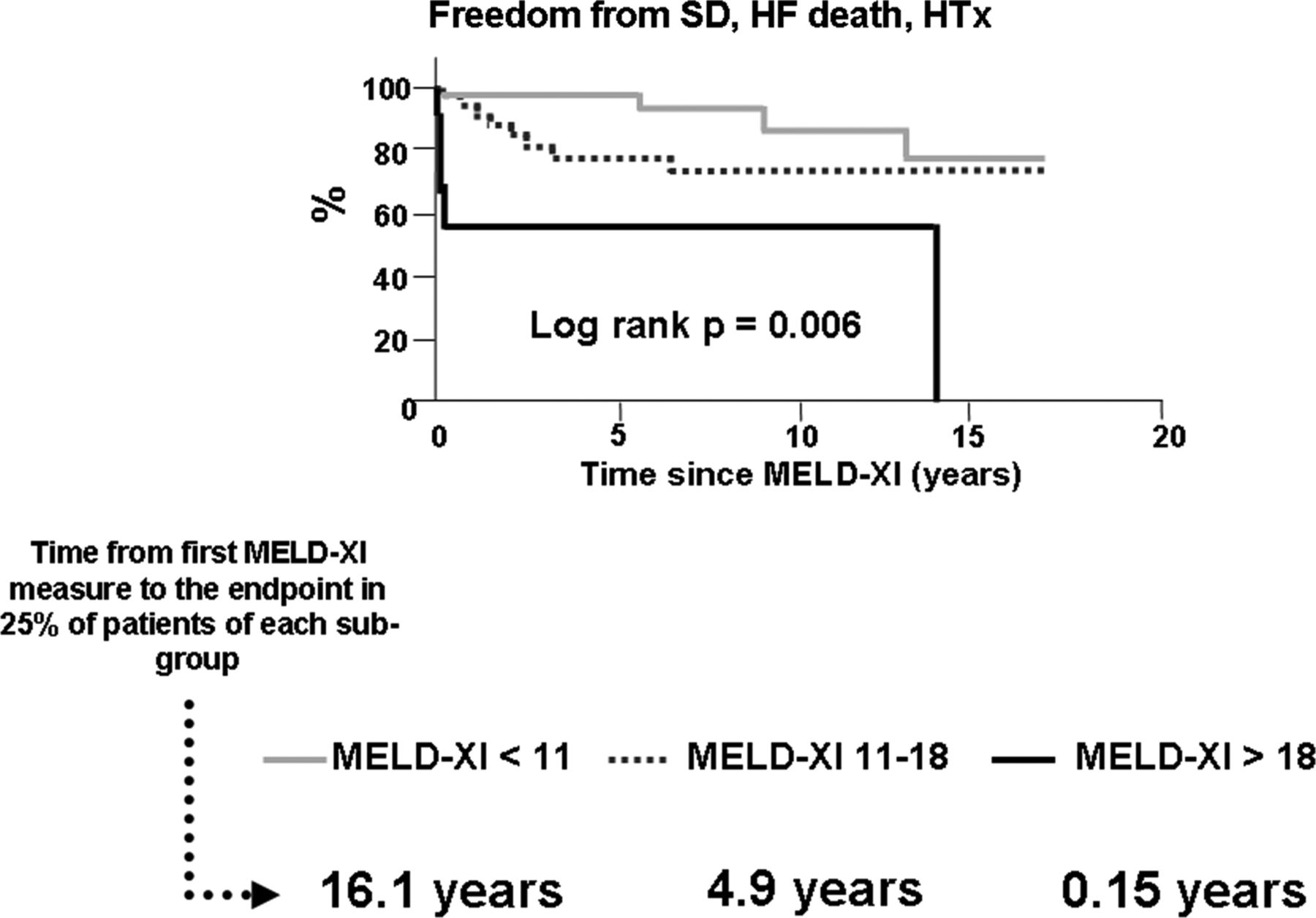
Kaplan-Meier estimates of the freedom from the composite endpoint of sudden cardiac death, death from congestive heart failure and cardiac transplantation, based on the baseline Model for End-stage Liver Disease eXcluding INR (MELD-XI) score. The time to the endpoint occurring in 25% of patient population since MELD-XI measurement is reported for each subgroup. Sudden death (SD), Heart Failure (HF) Heart transplant (HTx).
In a Cox proportional hazards regression model which included therapy with warfarin or aspirin, therapy with diuretics and time since Fontan surgery, the baseline MELD-XI score remained independently and directly related to the incidence of the composite endpoint of sudden death, death from congestive heart failure or cardiac transplantation during the follow-up period (HR for high MELD-XI score group vs low MELD-XI score of 7.76, 95% CI 2.05 to 29.33, p=0.008, table 2).
Change in MELD-XI score over time and cardiac mortality or transplantation
In 79 patients, more than two MELD-XI measurements were longitudinally collected (see online supplementary material figure 4,5).
Keeping time since last MELD-XI measurement constant, for each 10-unit increase in MELD-XI score compared with the previous, there was a 3.84-fold increase in the risk of sudden death, congestive heart failure death or cardiac transplantation (95% CI 1.31 to 11.26, p=0.01, see online supplementary material table S1).
Creatinine and bilirubin alone for predicting cardiac mortality or transplantation
Patients with creatinine above 2.0 mg/dl had a HR for the composite endpoint of 8.2 (95% CI 2.84 to 23.78, p=0.001) (see online supplementary material figure S5). All five patients in this group also had a MELD-XI score above 18.
Patients were stratified using two different cut-off points for total bilirubin. No independent association between bilirubin values and composite endpoint occurrence was identified. For patients with a total bilirubin above 2.4 mg/dl, the HR for the composite endpoint was 2.11 (95% CI 0.59 to 7.51, p=0.22) (see online supplementary material figure S5). A generalised Nagelkerke R2 for Cox proportional hazard was performed with generalised R2 values being 0.67, 0.70 and 0.09 for MELD-XI score, creatinine and total bilirubin, respectively.
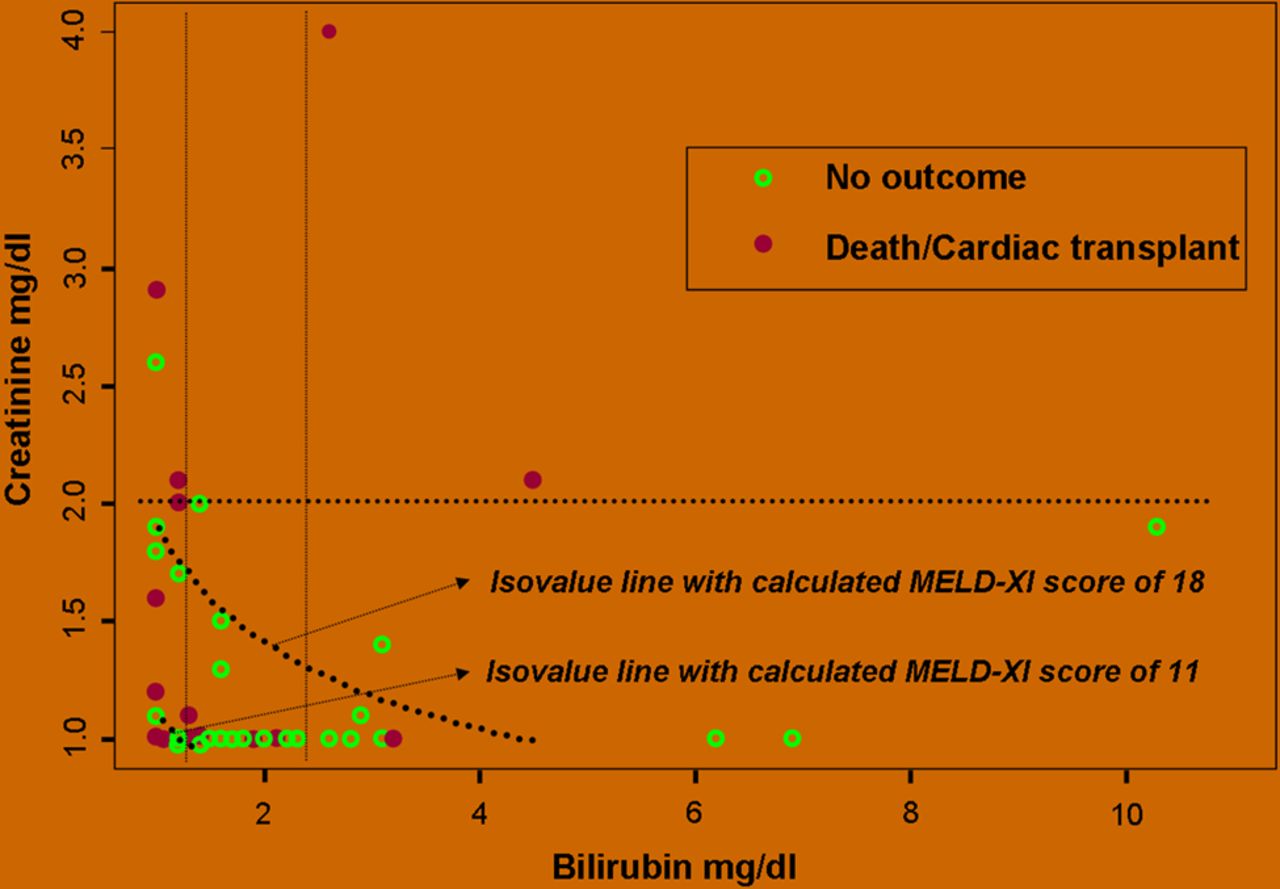
Figure 2 summarises creatinine and total bilirubin values for each patient of the study cohort. This representation shows that adverse outcomes occurred in five patients with low baseline MELD-XI score. Four of these five patients presented a marked interval increase of the MELD-XI score during the follow-up before the outcome (from 9.4±0 to 23.9±4.2, p=0.06). One patient died in the setting of refractory congestive heart failure; she was a 17-year-old girl with a right atrial-to-pulmonary artery Fontan and suffered from PLE and thrombus within the Fontan pathway, complicated by non-fatal stroke.
{kind=link}
{kind=link}
Creatinine versus total bilirubin scatter plot. Open circles represent patients who did not experience the composite endpoint, while filled circles represent patients with unfavourable clinical outcome (sudden death, death from congestive heart failure or cardiac transplantation). Vertical and horizontal lines represent cut-off points for total bilirubin and creatinine respectively, as identified with recursive partitioning. Curvilinear dotted lines identify isovalue points with a calculated Model for End-stage Liver Disease eXcluding INR (MELD-XI) score of 11 and 18 (MELD-XI=11.76(loge creatinine)+5.112(loge total bilirubin)+9.44)10 respectively, see text for details.
Discussion
This investigation is the first to demonstrate that patients surviving after Fontan surgery exhibit a similar MELD-XI score distribution compared with a cohort of patients with established liver cirrhosis due to hepatitis C infection. Higher MELD-XI scores identified a subgroup of patients after Fontan operation with a shorter time to the composite endpoint of sudden death, death from refractory heart failure or cardiac transplantation. The longitudinal analysis of MELD-XI scores confirmed that an increasing score over time was associated with unfavourable clinical outcome.
The Fontan operation allows short-term and intermediate-term palliation in a variety of complex congenital heart defects which share univentricular physiology. Early operative mortality is currently reported to be between 2% and 5%, based on different surgical series.4 ,14 Early survivors experience improved functional capacity and systemic oxygen saturation. Long-term survival is reported in this group of patients, but with ongoing attrition due to cardiac complications including refractory heart failure, sudden death and thromboembolic events.14 ,15 These complications seem to be time-dependent and collectively suggest that aspects of the Fontan circulation may include maladaptive mechanisms which eventuate in long-term failure and cardiac death.
In this study, the MELD-XI score is able to risk stratify patients after Fontan surgery, identifying a subgroup of patients with longer period of clinical stability. Total bilirubin alone did not provide the same prognostic implication as the MELD-XI score. The equally strong R2 values of creatinine and MELD-XI score demonstrates a similar predictive strength, but the additional value of the MELD-XI score in predicting clinical outcome in this cohort of patients seems to come from the ability to further stratify patients in the low-creatinine group who would otherwise be understaged. This is particularly notable for those patients with a MELD-XI score of 11 to 18 in whom risk appears raised compared with patients with a low MELD-XI score.
In patients with heart failure from acquired (non-congenital) cardiac diseases, well-established data support the notion that renal dysfunction is one of the most important independent risk factors for poor outcomes.16 This finding has been replicated in a large, single-centre cohort of adult patients with congenital heart disease,5 although only a minority had Fontan circulation. Interestingly, high central venous pressure and increased intra-abdominal pressure are postulated to play a major role in the deterioration of renal function in patients with decompensated heart failure.17 Although these haemodynamic abnormalities are often described in Fontan survivors who experience long-term complications, we did not find any significant association between high MELD-XI score and profound haemodynamic derangement. The haemodynamic characterisation of patients surviving with Fontan physiology is challenging, because Fontan pathway filling pressure, single ventricular end-diastolic pressure, cardiac index and pulmonary vascular resistances are affected by numerous factors including diuretic therapy, ventilation modality at the time of cardiac catheterisation, volume status, single ventricular contractility and diastolic function. In this setting, MELD-XI score could be a more accurate correlate of functional haemodynamic status than current catheterisation-based measures.
Congestive hepatopathy and hepatic fibrosis have been documented in patients surviving after Fontan palliation.7 ,18 Although the process of chronic liver injury in this population is not completely understood, the increase in central venous pressure and impaired oxygen delivery have been proposed as potential mechanisms of hepatocyte atrophy and necrosis and replacement liver fibrosis.6–7
Limited options exist today for adult patients experiencing progressive Fontan failure, especially in those countries where access to heart transplantation is limited due to scarcity of donor organs or due to healthcare policy. However, our data suggest that the MELD-XI score can be used to identify patients at increased risk of poor outcomes in the short-term to mid-term, and potentially before the establishment of irreversible and profound end-organ dysfunction which could impact their eligibility for, or potential to benefit from, advanced therapeutic approaches such as pharmacological modulation of pulmonary vascular resistance or consideration for cardiac transplantation.19–24
Limitations
This is a retrospective study, and the decision to collect laboratory data in this population was based on individual and uncontrolled physician decisions. This might have the effect of skewing the study cohort towards a more ill group of patients. Indeed, the overall endpoint rate of ∼3.0%/year in our study is higher than that reported in other published cohorts.4 ,14 ,15 In addition, our data have been collected from a tertiary referral centre for adults with congenital heart disease which might have determined unmeasured selection bias. These results will need to be replicated in a larger, prospective cohort of patients. However, even in this selected population of patients with Fontan circulation, low MELD-XI score was associated with a very low risk of unfavourable outcome during the follow-up period. This would seem to reinforce our hypothesis that MELD-XI score is predictive of clinical outcome in adults with Fontan circulation. We were unable to collect data on hepatitis serology in a large proportion of our patients, therefore we cannot exclude the possibility that at least some of these patients were exposed to hepatotropic viruses and could have ongoing injury from chronic infection. However, recognising this limitation, in this cohort, the impact of known hepatitis infection on liver function appeared relatively contained, without affecting MELD XI score distribution. While we expect prospective studies to improve our understanding of concomitant viral inflammation and effects on MELD-XI score in this population, we do not believe that the absence of this information limits the use of our results in a ‘real world’ cohort of patients with Fontan circulation.
Finally we were not able to consistently record data on the ‘arrhythmic burden’ of this population. We believe that this gap should be filled in a prospective study with rigorous ambulatory telemetric monitoring and additional arrhythmic data collection.
Conclusion
Fontan patients with a higher MELD-XI score are expected to have a worse clinical outcome due to the occurrence of sudden cardiac death, death from congestive heart failure and cardiac transplantation. The longitudinal change in MELD-XI score in this group of patients appears to carry additional unfavourable prognostic implications. As such, if confirmed by prospective study, the MELD-XI score may become a useful clinical risk factor for predicting short-term and mid-term cardiac mortality or transplantation in this growing population of patients with highly complex congenital heart disease.
Acknowledgments
We acknowledge the clinical and administrative staff of the Boston Adult Congenital Heart (BACH) and Pulmonary Hypertension Program, and the Clinical Research Program of Children's Hospital, Boston, for their invaluable care and support for these patients. We thank Kimberlee Gauvreau, ScD, for her significant contribution in the study design.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
Egidy Assenza: MELD-XI score and Fontan failure.
-
Contributors GEA had a primary role in study plan, data analysis and interpretation and manuscript drafting. DAG had a primary role as statistical consultant. MJL, AMV and MNS had primary roles in study plan, data interpretation and manuscript drafting. AB had a primary role in data collection and data analysis. SF had a primary role in data collection, data analysis and interpretation. KJM had a primary role in data collection, data analysis and data interpretation. CU had a primary role in study design, data interpretation and manuscript drafting. FW had a primary role in study design, data collection and interpretation and manuscript drafting.
-
Funding This study has been supported, in part, by the Dunlevie Fund of the Boston Adult Congenital Heart (BACH) and Pulmonary Hypertension Program, Children's Hospital Boston and Brigham and Women's Hospital.
-
Competing interests None.
-
Ethics approval Internal Review Board of Boston Children's Hospital.
-
Provenance and peer review Not commissioned; externally peer reviewed.