Article Text

Abstract
Objectives Early detection of microvascular dysfunction after acute myocardial infarction (AMI) could identify patients at high risk of adverse clinical outcome, who may benefit from adjunctive treatment. Our objective was to compare invasively measured coronary flow reserve (CFR) and hyperaemic microvascular resistance (HMR) for their predictive power of long-term clinical outcome and cardiac magnetic resonance (CMR)-defined microvascular injury (MVI).
Methods Simultaneous intracoronary Doppler flow velocity and pressure measurements acquired immediately after revascularisation for AMI from five centres were pooled. Clinical follow-up was completed for 176 patients (mean age 60±10 years; 140(80%) male; ST-elevation myocardial infarction (STEMI) 130(74%) and non-ST-segment elevation myocardial infarction 46(26%)) with median follow-up time of 3.2 years. In 110 patients with STEMI, additional CMR was performed.
Results The composite end point of death and hospitalisation for heart failure occurred in 17 patients (10%). Optimal cut-off values to predict the composite end point were 1.5 for CFR and 3.0 mm Hg cm−1•s for HMR. CFR <1.5 was predictive for the composite end point (HR 3.5;95% CI 1.1 to 10.8), but not for its individual components. HMR ≥3.0 mm Hg cm−1 s was predictive for the composite end point (HR 7.0;95% CI 1.5 to 33.7) as well as both individual components. HMR had significantly greater area under the receiver operating characteristic curve for MVI than CFR. HMR remained an independent predictor of adverse clinical outcome and MVI, whereas CFR did not.
Conclusions HMR measured immediately following percutaneous coronary intervention for AMI with a cut-off value of 3.0 mm Hg cm−1 s, identifies patients with MVI who are at high risk of adverse clinical outcome. For this purpose, HMR is superior to CFR.
- Acute myocardial infarction
- Cardiac magnetic resonance (CMR) imaging
- Percutaneous coronary intervention
Statistics from Altmetric.com
- Acute myocardial infarction
- Cardiac magnetic resonance (CMR) imaging
- Percutaneous coronary intervention
Introduction
Coronary microvascular dysfunction frequently occurs following successful angioplasty for acute myocardial infarction (AMI). The proposed mechanisms underlying microvascular dysfunction in this setting include capillary plugging with thromboembolic material and leucocytes, extravascular compression by oedema, haemorrhagic microvascular destruction and an elevated left ventricular pressure.1–3 Microvascular dysfunction after AMI can be assessed by cardiac magnetic resonance (CMR) and is referred to as microvascular injury (MVI). MVI is encountered in up to 50% of patients with ST-segment elevation myocardial infarction (STEMI) despite thrombolysis In myocardial infarction (TIMI) III flow1 2 and in 14% of patients with non-ST-segment elevation myocardial infarction (NSTEMI).4 Strategies aimed at counteracting microvascular dysfunction and improving myocardial perfusion are being investigated, for example, ischaemic postconditioning, pressure-controlled intermittent coronary sinus occlusion and adjunctive pharmacological treatment.5–8 Because microvascular dysfunction does not occur in all patients with AMI, the design of such studies could be improved by initial selection of patients at increased risk, in whom adjunctive treatment could actually be beneficial. The therapeutic window for treatment of microvascular dysfunction after AMI occurs immediately after reperfusion has been established.9 CMR-defined MVI is unsuitable for the purpose of risk stratification, since it is not available at the time of angioplasty. Coronary flow reserve (CFR) and hyperaemic microvascular resistance (HMR) can be both measured with coronary pressure-flow guidewires immediately after epicardial patency has been restored and inform on microvascular dysfunction.10–15 Alternatively, these measurements could also be used as end point to evaluate therapeutic efficacy of intracoronary pharmacological interventions.
In this study, we pooled simultaneous measurements of coronary pressure and Doppler flow velocity from all currently available AMI datasets. The primary objective was to investigate whether CFR or HMR is superior in predicting adverse clinical outcome as well as CMR-defined MVI as previous work by Carrick et al has already determined that a combination of microvascular resistance and CFR does not have improved prognostic utility compared with microvascular resistance alone.16
Methods
Study population
Prospectively collected data was pooled from patients in whom combined coronary pressure and Doppler flow velocity measurements were performed for research purposes.10 12 13 17 Patients with both STEMI and NSTEMI were analysed. Stable patients without coronary artery disease served as a reference cohort (details can be found in the online supplementary material).18 Study protocols including documentation of clinical follow-up, were approved by the institutional review boards and complied with the principles of the Declaration of Helsinki.
Patients with AMI
Patient were treated according clinical guidelines.19 20 Further details on treatment are provided in the online supplementary material. After angiographic reperfusion was established, simultaneous intracoronary Doppler flow velocity and distal pressure measurements were performed. TIMI flow grade, corrected TIMI frame count (cTFC) and ST-segment resolution of more than 70% 1 hour after reperfusion were defined as previously described.21 Cardiac enzymes troponin-I, troponin-T and creatine kinase myocardial band (CK-MB) were determined according to the respective study protocol.
Invasive measurements
Invasive measurements were obtained in similar fashion in patients with AMI and stable control patients. Prior to the measurements, 200–300 µg nitrates were administered intracoronary. Aortic pressure was recorded from the guiding catheter. A 0.014 inch guidewire (ComboWire, Volcano Philips, USA) equipped with both a distal pressure sensor and a Doppler crystal was passed through the guiding catheter. Distal pressure was equalised with aortic pressure at the tip of the guiding catheter. Then, the guidewire was passed just distal to the site of intervention and the wire was manipulated to obtain a high-quality Doppler signal. Average Doppler flow peak velocity (APV), mean aortic pressure and mean distal pressure were simultaneously recorded with the ComboMap console (Volcano Phillips; figure 1). Recordings were made during resting conditions and during hyperaemia induced by intracoronary bolus injection of 150 µg adenosine or 15–20 mg papaverine, or intravenous infusion of 140 µg/kg/min adenosine or 150 µg/kg/min ATP. Fractional flow reserve (FFR) was calculated as the ratio between hyperaemic mean distal pressure and aortic pressure. CFR was calculated as the ratio between hyperaemic and resting APV. HMR was calculated as the ratio between hyperaemic mean distal pressure and hyperaemic APV. Hyperaemic stenosis resistance index was calculated as the ratio between the hyperaemic pressure gradient (mean aortic-distal pressure) and APV.22

Patient with ST-elevation myocardial infarction enrolled into the study. This patient presented with acute chest pain for 180 min and ST-segment elevation in the anteroseptal leads, with reciprocal depression in the inferior leads (panel A). Emergency coronary angiography was performed showing a proximal left anterior descending artery occlusion (panel B). After primary percutaneous coronary intervention, thrombolysis In myocardial infarction III flow was restored (panel C). Simultaneous Doppler flow velocity and distal pressure measurements were performed in the distal left anterior descending artery (LAD) with intracoronary adenosine 150 µg, yielding a coronary flow reserve (CFR) of 1.7 and hyperaemic microvascular resistance (HMR) of 5.2 mm Hg·cm−1 s (panel D). (Panels E and F) Cardiac MRI with late gadolinium enhancement showed a large area of hyperenhancement consistent with an anteroseptal infarction. Within this area, a hypoenhanced core is visible consistent with extensive microvascular injury (indicated by arrows). Panel E is a short-axis view and panel F is a long-axis view. FFR, fractional flow reserve.
Clinical outcomes
To evaluate clinical outcome, a composite end point consisting of death and hospitalisation resulting from congestive heart failure was used. Follow-up was retrospectively obtained for patients with AMI by the local investigators (GF, DdW, HK, RW, MS) via visitation of the outpatient clinic, telephone contact or review of the medical record. The local investigators did not have access to the merged invasive measurement dataset when end points were ascertained. Hospitalisation for heart failure was defined as hospitalisation because of symptoms of heart failure in combination with a positive chest radiograph and a clinical diagnosis of congestive heart failure.
CMR imaging protocol
For patients with STEMI, CMR imaging was performed according to the different protocols at each site as described in the previous publications.10 12 13 CMR was performed between 24 hours and 2 weeks (when MVI most frequently occurs23) after the index procedure and analysed by the local investigators. In brief, CMR cine images were acquired to calculate left ventricular end systolic and diastolic volumes and left ventricular ejection fraction. Late gadolinium enhancement imaging was performed 10–15 min after intravenous administration of a gadolinium-based contrast agent to calculate the infarct size as percentage of the left ventricle and to assess MVI.
Statistical analysis
Details on statistical analysis are found in the online supplementary material.
Results
Patient characteristics
The flow of patients through the study is shown in figure 2. After exclusion of 16 patients, 176 patients remained for analysis (131 STEMI and 45 NSTEMI). The reference cohort consisted of 51 stable patients with 96 measurements in normal coronary arteries. Table 1 describes the baseline characteristics.

Flow diagram shows the enrolment and flow of patients through the study. CMR, cardiac magnetic resonance imaging; LGE, late gadolinium enhancement; NSTEMI, non-ST-segment elevation myocardial infarction; STEMI, ST-segment elevation myocardial infarction.
Baseline characteristics
Clinical outcomes of patients with AMI
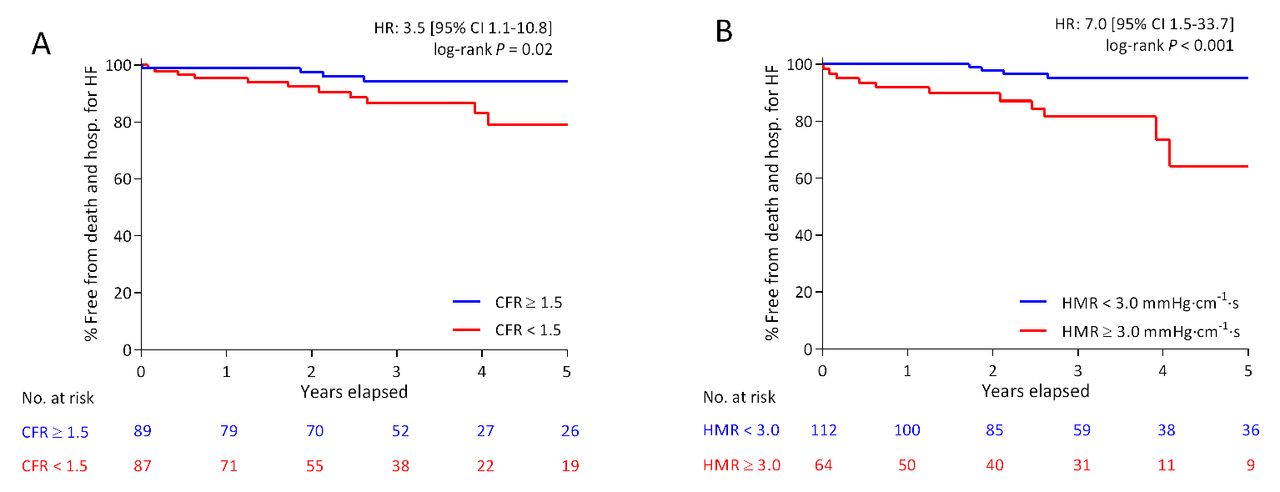
Median follow-up time was 3.2 years (IQR 2.0–5.1), with a maximum follow-up time of 9.2 years. The composite end point of death and hospitalisation for heart failure occurred in 17 patients (9.7%). Eight patients (4.5%) died during the follow-up time (five STEMI and three NSTEMI). Nine patients (5.1%) underwent hospitalisation for heart failure (six STEMI and three NSTEMI). For CFR, the optimal cut-off value to predict the composite end point was 1.5 or lower, with a sensitivity of 53% and specificity of 77%. The composite end point occurred in 14.9% when CFR was low and in 4.5% when CFR was high. The optimal cut-off value for HMR to predict the composite end point was 3.0 mm Hg cm−1 s or higher, with a sensitivity of 77% and specificity of 69%. The composite end point occurred in 3.6% when HMR was low and in 20.3% when HMR was high. For CFR, Kaplan-Meier analysis stratified according to cut-off values (figure 3A) showed progressive divergence of the curves throughout the entire follow-up duration. Kaplan-Meier analysis for HMR (figure 3B) showed a similar pattern, but with more pronounced divergence of the curves. CFR at a cut-off of 1.5 was not significantly associated with either of the individual components of the composite end point: HR 2.8 (95% CI 0.6 to 14.2) for death and 4.0 (95% CI 0.8 to 19.4) for hospitalisation for heart failure. HMR ≥3.0 mm Hg cm−1 s was significantly associated with both individual end points of the composite end point: HR 6.4 (95% CI 1.3 to 32.0) for death and 7.0 (95% CI 1.5 to 33.7) for hospitalisation for heart failure.

Kaplan-Meier for composite of death and hospitalisation for heart failure. Kaplan-Meier analysis for the composite end point consisting of death and hospitalisation for heart failure. Panel A shows the Kaplan-Meier curves for CFR stratified according to the optimal cut-off value of 1.5. Panel B shows the Kaplan-Meier curves for HMR stratified according to the optimal cut-off value of 3.0 mm Hg cm−1 s. CFR, coronary flow reserve; Hosp. for HF, hospitalisation for heart failure; HMR, hyperaemic microvascular resistance.
Angiographic characteristics and biomarkers
Table 2 shows the infarct characteristics of patients with AMI for the whole group and stratified according to the HMR cut-off. Patients with high HMR had significantly greater cardiac enzyme release than patients with low HMR and more signs indicative of the no-reflow phenomenon, with lower cTFC, less frequent TIMI flow grade III and less frequent ST-segment resolution >70%. Table 3 and online supplementary table 1 show the multivariable models for the prediction of the composite end point and CMR-defined MVI. HMR, but not CFR, remained an independent predictor for both outcome and MVI after correction for other significantly predictive clinical and haemodynamic variables available immediately after revascularisation.
Infarct characteristics
Cox proportional hazard model for prediction of death and hospitalisation for heart failure in patients with AMI
Occurrence of CMR-defined MVI
Among patients with STEMI, CMR imaging was performed in 110 patients. MVI occurred in 56 patients (51%). Figure 4 shows the receiver operating characteristic curve analysis for CMR-defined MVI. HMR had a significantly better diagnostic performance than CFR for identification of MVI.
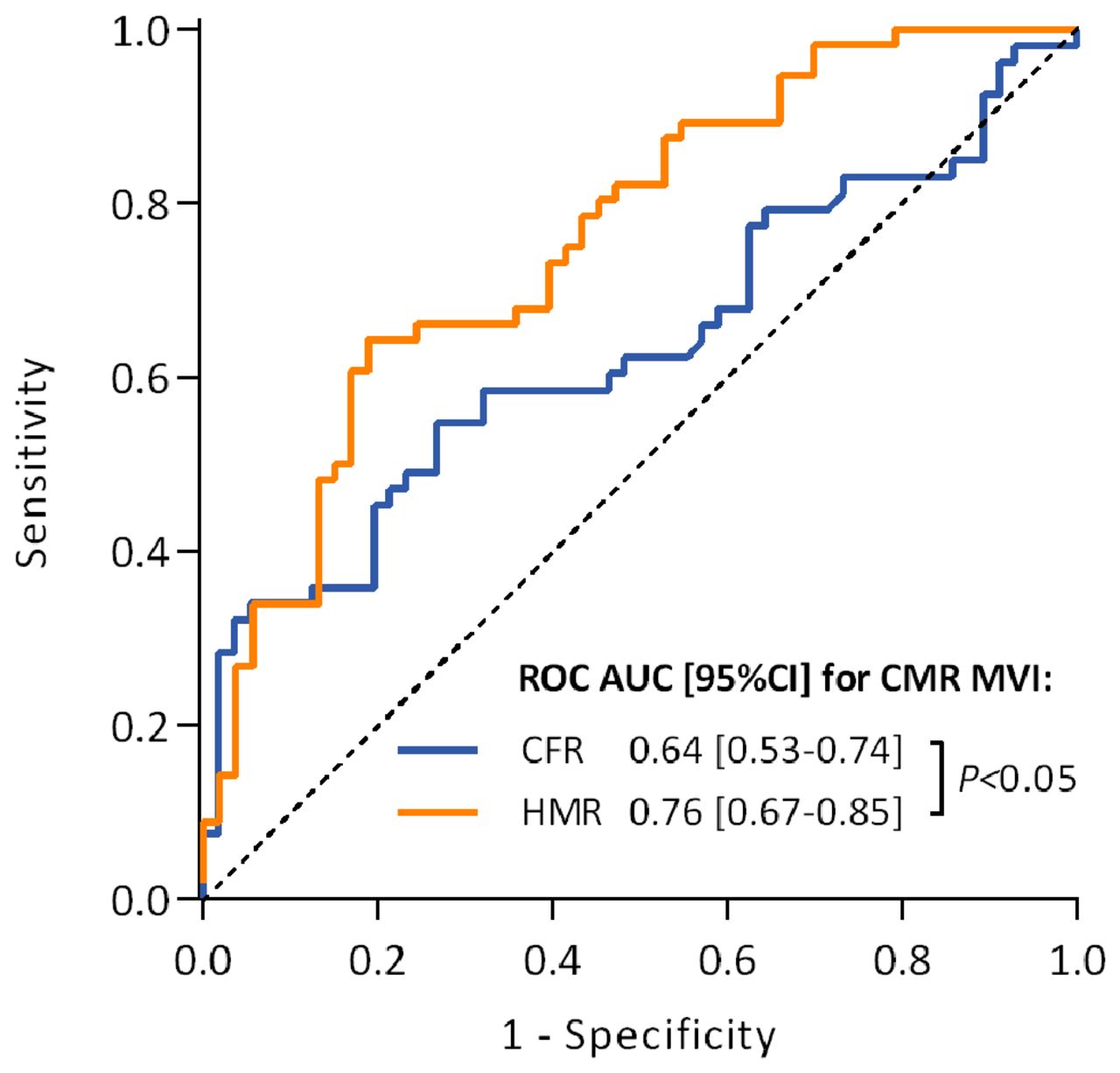
Receiver operating characteristic curves for CMR-defined MVI HMR has a significantly greater area under the receiver operating characteristic curve than CFR for the prediction of CMR-defined MVI in patients with STEMI. CFR, coronary flow reserve; CMR, cardiac magnetic resonance imaging; HMR, hyperaemic microvascular resistance; MVI, microvascular injury; ROC AUC, area under the receiver operating characteristic curve.
Invasive haemodynamics
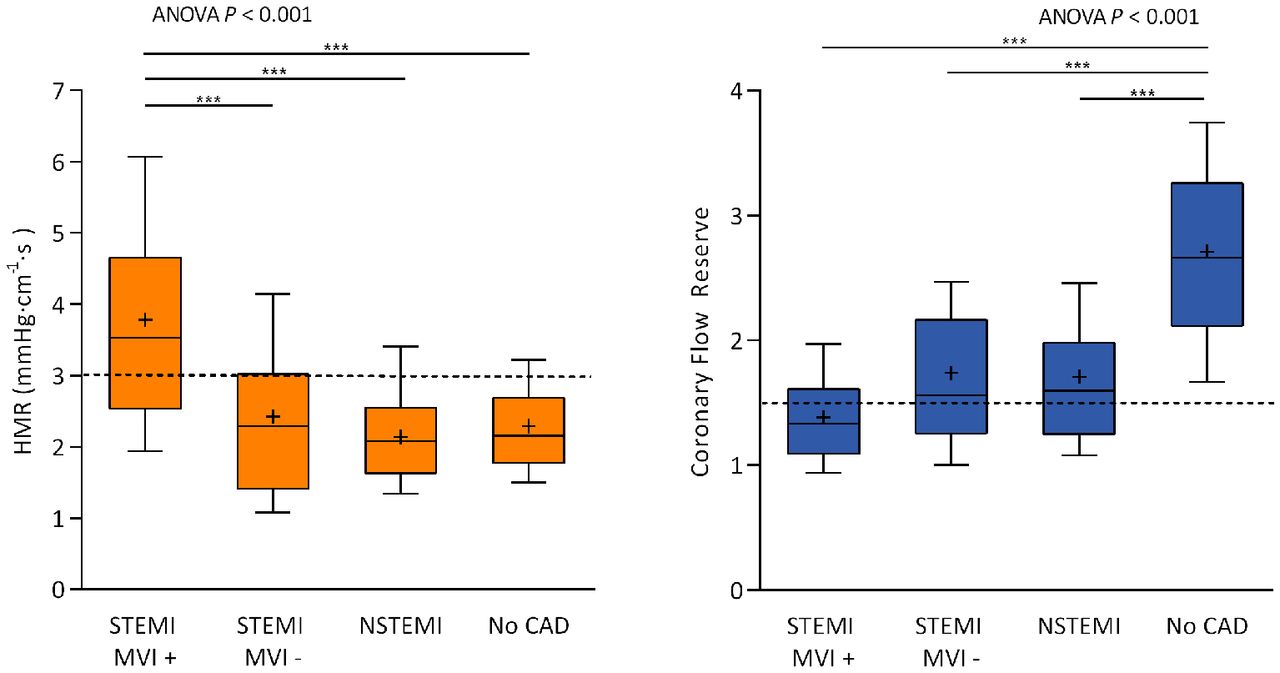
Haemodynamic characteristics in AMI culprit vessels as compared with normal coronary arteries in stable patients are shown in online supplementary table 2. CFR was significantly lower and HMR was significantly higher in patients with AMI compared with control patients. In figure 5, CFR and HMR are stratified according to pathophysiological manifestation: STEMI with the presence of MVI, STEMI without the presence of MVI, NSTEMI and control patients. CFR is depressed in all manifestations of AMI as compared with control patients, but no differences in CFR were detected across the three AMI groups. In four patients with STEMI (2.3%), CFR was <1.5 and FFR was <0.75 and two of these patients had CMR-defined MVI. HMR was significantly increased in patients with STEMI with MVI compared with the other three groups. HMR was not elevated in patients with STEMI without MVI or patients with NSTEMI compared with stable patients. The optimal cut-off value for HMR to predict CMR-defined MVI was 3.1 mm Hg·cm−1·s, with a sensitivity of 64% and specificity of 81%. This HMR value was close to the optimal cut-off for the composite end point of 3.0 mm Hg cm−1 s, which had a sensitivity of 67% and specificity of 72% to predict MVI. Other CMR data stratified according HMR are shown in online supplementary table 3. Patients with STEMI with HMR ≥3.0 mm Hg·cm−1·s had worse CMR infarct parameters compared with patients with low HMR.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Different pathophysiological manifestation of AMI and stable patients CFR and HMR are stratified according to four different groups: patients with STEMI with and without CMR-defined MVI (n=56 and n=54, respectively), patients with NSTEMI (n=45) and stable patients without obstructive CAD (n=96). Patients with STEMI without CMR were not included in this analysis. Panel A: CFR was significantly lower in all clinical manifestations of AMI as compared with stable control patients. Among the different manifestations of AMI, no significant differences in CFR were observed suggesting that a decreased CFR is not specific indicator of microcirculatory injury. Panel B: HMR was significantly higher in patients with STEMI with MVI as compared with the other three groups, indicating that HMR is specifically increased in patients with AMI with microcirculatory injury. Boxes represent median and IQR, with whiskers as the 10th through 90th percentile. The dashed line indicates cut-off values for CFR at 1.5 and for HMR at 3.0 mm Hg cm−1 s. *** indicates a significance level of p<0.05 after post hoc comparison with Bonferroni correction. + represents the mean. ANOVA, analysis of variance; CAD, coronary artery disease; CFR, coronary flow reserve; CMR, cardiac magnetic resonance; HMR, hyperaemic microvascular resistance; MVI, microvascular injury; NSTEMI, non-ST-segment elevation myocardial infarction; STEMI, ST-segment elevation myocardial infarction.
Discussion
This patient-level pooled analysis combines all available studies that have performed simultaneous Doppler flow velocity and distal pressure assessments immediately after revascularisation of AMI. Our findings are: (1) CFR and HMR are both predictive for a composite of death and hospitalisation for heart failure, but HMR remains independently associated with the composite outcome after correction for baseline and procedural characteristics. (2) HMR, but not CFR, is a significant predictor for both individual components of the composite end point. (3) HMR is a superior predictor for CMR-defined MVI compared with CFR. (4) A well-defined cut-off value for HMR of 3.0 mm Hg·cm−1·s exists that can be used to identify patients at high risk for adverse outcome.
HMR predicts adverse outcome better than CFR
Among patients with AMI, both CFR at a cut-off of 1.5 and HMR at a cut-off of 3.0 mm Hg·cm−1·s are associated with the composite end point of death and hospitalisation for heart failure. However, high HMR is associated with a higher HR for the occurrence of the composite end point than low CFR and also with both individual components of the end point, whereas low culprit CFR is not. These findings corroborate earlier studies performed with Doppler flow wires, but without a pressure sensor. Jin et al also found that hyperaemic coronary resistance predicted a composite of cardiac death and rehospitalisation for heart failure.24 van de Hoef et al reported long-term follow-up of an earlier study by Bax et al 25 and also found that culprit CFR was not predictive of cardiac mortality alone, although non-culprit CFR was.26 Furthermore, HMR, but not CFR, remained an independent predictor for adverse outcome and MVI after multivariable correction. The analysis according to AMI group in figure 5 clarifies why HMR is a superior predictor of long-term adverse clinical outcome, despite both CFR and HMR being significantly altered in the setting of AMI. After stratification of patients with AMI, CFR was equally depressed in all clinical manifestations of AMI compared with stable patients. HMR, however, was specifically elevated in STEMI with MVI and was not increased in STEMI without patients with MVI or NSTEMI, with stable controls as reference. Together, these findings suggest that CFR is generally decreased in the setting of AMI and not specifically in patients with MVI. However, HMR is only elevated in patients with MVI and remains within normal range if the microvasculature is unharmed. Based on our findings, we presume that the superior performance of HMR in identification of patients with MVI in whom microvascular dysfunction occurs at the most extreme levels, translates into better prediction of long-term adverse clinical outcome. This is supported by earlier work that has shown the prognostic utility of CMR-defined MVI for adverse clinical outcome.27
Why is HMR superior to CFR for prediction of MVI?
CFR quantifies the amount of autoregulatory reserve that the microvascular bed harbours.18 To meet the metabolic demand of the underlying myocardium, arterioles vasodilate in the presence of a coronary stenosis diminishing the autoregulatory reserve.18 Therefore, CFR represents microvascular dysfunction and is also lowered when residual coronary narrowing is present. On average, FFR was slightly lower and the hyperaemic stenosis resistance index was slightly higher in revascularised culprit vessels than in normal control arteries, reflecting minor residual stenosis (see online supplementary table 2). A second explanation relates to the fact that the metabolic myocardial demand is typically increased after AMI leading to reactive hyperaemia.28 We found a significantly higher heart rate and an increased APV in patients with AMI as compared with stable controls. CFR is calculated as the ratio of hyperaemic and resting APV. In patients with AMI resting APV is increased, leading to a decrease in CFR. However, we have previously shown that there is no relationship between resting flow immediately after AMI and infarct size.29 Residual stenosis and increased metabolic demand thus both affect CFR,18 but are not restricted to patients with MVI specifically. This is illustrated by figure 5A, where CFR was reduced in all pathophysiological manifestations of AMI as compared with stable patients, but could not accurately discriminate patients with MVI. In contrast, residual stenosis only influences HMR if it is functionally severe with FFR <0.60,30 which never occurred in our study. Also, the issue of reactive hyperaemia does not apply to HMR since it is measured during hyperaemia where autoregulation is exhausted by administration of a hyperaemic agent. Since HMR is not influenced by residual stenosis or increased baseline flow, it is the better parameter to identify patients with AMI with microvascular dysfunction than CFR.
Other measures of microvascular dysfunction
Besides CFR and HMR, risk stratification is also possible based on cTFC, ST-segment resolution of 70%, various CMR parameters, cardiac enzyme release, temporal evolution of CFR or the pressure at zero flow.3 10 31 However, all of these parameters are either not available immediately after revascularisation or require offline calculation. The fact that HMR is immediately available after revascularisation is of paramount importance, since a window for adjunctive therapy still exists. Physiological measurements in non-culprit vessels also provide prognostic information,26 but are not indicative of CMR-defined MVI.10 Index of microcirculatory resistance (IMR) is another method to quantify microvascular resistance. IMR is measured with a wire that combines a distal pressure sensor and a temperature sensor to measure coronary flow through the thermodilution technique. Studies by Fearon et al and Carrick et al have shown that IMR predicts adverse clinical outcome at a threshold >40.16 32 Carrick et al also showed that IMR was predictive of various CMR outcomes and that a combination of IMR and CFR did not confer improved prognostic utility as compared with IMR alone. Despite similarities, notable differences with the study by Carrick et al are that we measured Doppler flow velocity, performed a multicentre study, omitted heart failure during the index procedure from our end point, enrolled a smaller cohort and also evaluated patients with NSTEMI and stable patients to better understand the pathophysiology. In a meta-analysis on study level, Bulluck et al found IMR >41 to be predictive of CMR-defined MVI.33 However, IMR was not found to be predictive of MVI in two of the six included studies.11 34 Furthermore, in a comparative study between HMR and IMR, Patel et al found HMR to be predictive of infarct transmurality and size, whereas IMR was not.13 A difference between HMR and IMR is that Doppler velocity measurements are indexed to vessel size, whereas IMR uses mean transit time as a surrogate of absolute coronary flow. Therefore, contrary to HMR, IMR not only depends on microvascular function, but also on subtended myocardial mass. However, measuring HMR is probably more challenging than measuring IMR, with higher failure rates related to measurement quality. Additional studies are needed to establish whether HMR or IMR is better suited for identification of patients at increased risk after AMI. Our study demonstrates that HMR is also predictive of clinical outcome and provides a clear cut-off value for this purpose. As such, HMR and IMR can now both be used for risk stratification after AMI.
Limitations
First, the centres participating in this study did not use a uniform study protocol. However, acquisition methodology of the invasive and imaging data was similar and all centres used contemporary Doppler flow and pressure wires as well as advanced CMR imaging techniques. Second, invasive measurements had to be excluded in 8% either due to poor Doppler flow signals or iatrogenic coronary dissection related to the measurement in one patient. Third, no core laboratory analysis of the invasive measurements and CMR was performed and data were used as reported in the original publications. However, the studies all used a similar protocol and HMR remained strongly predictive of clinical outcome and CMR-defined MVI even without core laboratory analysis, supporting routine clinical use. Fourth, no clinical events committee to adjudicate the end points was in place. Finally, although this study is the largest study to perform detailed physiological characterisation by combined Doppler flow velocity and pressure measurement in the context of AMI, sample size remains limited.
Conclusion
Invasive HMR measured immediately after revascularisation for acute myocardial infarction is predictive of death and hospitalisation for heart failure. HMR has superior predictive value to CFR, presumably through better identification of patients suffering from microcirculatory injury. This is evidenced by the finding that HMR has a better performance to detect CMR-defined MVI than CFR. For risk stratification in clinical practice, a cut-off value of 3.0 mm Hg cm−1 s can be used for HMR to identify patients at high risk who might benefit from adjunctive treatment.
Key messages
What is already known on this subject?
Microvascular dysfunction after angiographically successful revascularisation for acute myocardial infarction occurs in approximately 40%–50% of patients. These patients may benefit from adjunctive therapy, but can not be identified from the coronary angiogram alone.
What might this study add?
This study shows that hyperaemic microvascular resistance can be used to detect patients at risk of adverse clinical outcome and with cardiac magnetic resonance imaging defined microvascular injury. For this purpose, hyperaemic microvascular resistance at a cut-off value of 3.0 mm Hg cm−1 s was superior to coronary flow reserve at a cut-off value of 1.5.
How might this impact on clinical practice?
The results of this study indicate that hyperaemic microvascular resistance could be used for risk stratification of patients and to select those who might benefit from adjunctive treatment targeted at microvascular dysfunction.
References
Footnotes
GAW and GF contributed equally.
Contributors GAdW, GF, PFAT, DdW, NP, MS, RW and HK performed study procedures and ascertained follow-up. RK, SU, PK, NvR, TA and DP supervised the study at the respective sites. GAdW and NvR drafted the manuscript. GAdW and PvdV performed statistical analysis. All authors critically reviewed the manuscript and made revisions.
Funding This study was funded by institutional grants from the Oxford Biomedical Research Centre, Volcano Corporation, Biotronik, Turkish Academy of Sciences and National Institute for Health Research.
Competing interests GAdW, DP, RK and NvR have received speaking/advisory board honoraria from Volcano Corporation. The other authors report no conflicts of interest pertaining to this study.
Patient consent Obtained.
Ethics approval VU University Medical Center.
Provenance and peer review Not commissioned; externally peer reviewed.
Correction notice Since this paper first published online the Oxford Acute Myocardial Infarction (OxAMI) Study investigators have been added to the author line.