Article Text

Abstract
Background Dabigatran etexilate, a new thrombin inhibitor, has been shown to be comparable to warfarin in patients with atrial fibrillation (AF). However, there is a limited body of evidence on the efficacy and safety of using dabigatran among patients undergoing AF catheter ablation.
Objective A random effects meta-analysis was performed of controlled trials comparing dabigatran and warfarin in paroxysmal/persistent AF patients undergoing catheter ablation.
Methods Data sources included Medline, Embase, and Cochrane (from inception to April 2013). Three independent reviewers selected studies comparing warfarin to dabigatran. Descriptive and quantitative information was extracted from each selected study, regarding periprocedural all cause mortality, thromboembolic events and major bleeding, as well as modalities of periprocedural anticoagulation bridging.
Results After a detailed screening of 228 search results, 14 studies were identified enrolling a total of 4782 patients (1823 treated with dabigatran and 2959 with warfarin). No deaths were reported. No significant differences were found between patients treated with dabigatran and warfarin as regards thromboembolic events (0.55% dabigatran vs 0.17% warfarin; risk ratios (RR)=1.78, 95% CI 0.66 to 4.80; p=0.26) and major bleeding (1.48% dabigatran vs 1.35% warfarin; RR=1.07, 95% CI 0.51 to 2.26; p=0.86). No difference was found between the 110 mg twice daily and 150 mg twice daily dabigatran dosages concerning major bleeding (0% vs 1.62%, respectively; RR=0.19, 95% CI 0.01 to 3.18; p=0.25) and thromboembolism (0% vs 0.40%, respectively; RR=0.72, 95% CI 0.04 to 12.98; p=0.82).
Conclusions In the specific setting of AF catheter ablation, this first pooled analysis suggests that patients treated with dabigatran have a similar incidence of thromboembolic events and major bleeding compared to warfarin, with low event rates overall.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/
Statistics from Altmetric.com
Introduction
Atrial fibrillation (AF) is the most prevalent sustained arrhythmia and its prevalence is likely to rise steeply until 2050.1 Stroke and systemic embolism are among the most feared complications of AF and can be effectively tackled by anticoagulation.2
Catheter ablation is currently recommended (class IIa, level of evidence C) as an interventional alternative for the treatment of patients with AF having symptomatic recurrences despite antiarrhythmic therapy.3 Over the last 13 years this has become a very commonly performed procedure for the treatment of symptomatic AF patients.4
Rigorous anticoagulation in the setting of AF catheter ablation has been demonstrated to be of prime importance. The recent large phase III trials involving the use of novel oral anticoagulants5–7 confirmed the non-inferiority, and even superiority in some cases, of dabigatran, rivaroxaban, and apixaban compared to warfarin in AF patients. However, since a planned AF catheter ablation procedure was listed as an exclusion criteria in those trials, the efficacy and safety results cannot be extended to that setting. The 2012 Expert Consensus Statement on the management of patients with AF, by the Heart Rhythm Society, European Heart Rhythm Association, and European Cardiac Arrhythmia Society,8 highlights the limited clinical experience with the new anticoagulants in AF catheter ablation. Thus, even though dabigatran is being widely used and has been in vogue longer than the other new agents, strong evidence towards its utilisation in patients undergoing AF ablation is lacking. Further, the presence of controversial results9 in controlled trials with warfarin has led cardiologists to question its safety and efficacy.
We therefore aimed to systematically evaluate, using a meta-analysis, all evidence concerning the use of dabigatran versus warfarin in catheter ablation for AF. The main objectives of this study were: (1) evaluate the efficacy and safety of dabigatran compared to warfarin; (2) determine whether there were significant differences between the 110 mg twice daily and 150 mg twice daily dosages of dabigatran; and (3) study the management of periprocedural bridging anticoagulation.
Methods
Data sources and search strategy
We performed a search on Medline (via Ovid and PubMed), Embase, and Cochrane (from inception to 13 April 2013) databases using the following search string: “atrial fibrillation” AND “ablation” AND “dabigatran”.
The reference lists of the accessed full text articles were further researched for sources of potential information relevant to this analysis. Experts in the field were contacted to ensure that all important studies in this area were covered. Abstract authors in congresses were also contacted by email in order to retrieve additional information. The databases were reassessed before the completion of the manuscript to find if any of the included abstracts had been published as full text meanwhile.
Inclusion and exclusion criteria
The population, intervention, comparison, and outcome approach was used for conducting the meta-analysis.10 The population of interest included patients with AF. The intervention was catheter ablation of AF and the associated periprocedural anticoagulation. Comparisons were performed between the following groups: warfarin versus dabigatran; dabigatran 110 mg twice daily vs 150 mg twice daily. The primary outcomes were: major bleeding, thromboembolism, and all cause mortality. The presence of minor bleeding, when reported, was also assessed.
Only controlled trials (full text articles or conference abstracts) of patients undergoing catheter ablation of AF and treated either with warfarin or dabigatran before the procedure were selected.
The minimum necessary follow-up for study inclusion was until discharge after the procedure. Additionally, to be included, studies needed to provide information on assessment of all three major clinical outcome parameters: major bleeding, thromboembolism, and death.
The following exclusion criteria were defined: trials with no comparator (ie, warfarin), namely observational studies including only patients treated with dabigatran; starting of dabigatran treatment only after catheter ablation; and evaluation of efficacy restricted to laboratory or imaging end points.
To ensure that trials met the prespecified inclusion criteria, search results were reviewed by three investigators (RP, AB, BC), who needed to be in agreement for study selection.
Data extraction and presentation for the preparation of this manuscript followed the recommendations of the PRISMA group.11
Study quality was formally evaluated using the Delphi Consensus criteria for randomised controlled trials12 and a modified Newcastle–Ottawa Quality Assessment Scale for Case Control Studies13 by three reviewers (RP, AB, BC). An agreement, between the three reviewers was mandatory for the final classification of studies.
End point definition for meta-analysis
Classification of bleeding was based on previous reports and suggested recommendations.14 The following end points were defined for the generation of forest plots on meta-analysis.
The primary end points were:
-
All cause periprocedural death
-
Thromboembolism—a composite of stroke, transient ischaemic attack (TIA), systemic or pulmonary embolism. Asymptomatic cerebral embolism detected on routine or protocol MRI or CT (ie, imaging end points with no clinical manifestation) was not included in the analysis.
-
Major bleeding—comprising cardiac tamponade, bleeding necessitating intervention or transfusion, massive haemoptysis, haemothorax, retroperitoneal bleeding or any other life-threatening bleed leading to prolongation of hospitalisation.
Secondary end point was:
-
Minor bleeding—defined as puncture site bleeding, thigh ecchymosis or haematoma, pericardial effusion with no haemodynamic compromise, minor gastrointestinal bleeding, epistaxis or any bleeding treated conservatively with no need for transfusion, surgery or prolonged hospitalisation.
Assessment of periprocedural bridging of anticoagulation
The following data were extracted for assessing periprocedural bridging anticoagulation: periprocedural warfarin regimen (uninterrupted drug or discontinuation); timing of dabigatran interruption and restart; target activated clotting time (ACT).
Statistical analysis
Data were pooled using random effects, according to the Mantel–Haenszel model, through Review Manager (RevMan), V.5.1. (Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2011). The measurement of treatment effect was performed using risk ratios (RR) and 95% CIs. Pairwise comparisons were performed for all end points between patients treated with dabigatran and warfarin, and a separate sub-analysis (sensitivity analysis) was performed among patients treated with dabigatran, according to the dosage mentioned in the trials (150 mg twice daily vs 110 mg twice daily). Sensitivity analysis was also performed restricting the analysis of data to: trials whose patients were treated with uninterrupted warfarin, prospective studies, investigations published as full text articles, studies whose follow-up was at least 30 days, and studies in which five of the nine items on the Delphi Consensus criteria for randomised controlled trials and a modified Newcastle–Ottawa Quality Assessment Scale for case–control studies were deemed satisfactory.
Statistical heterogeneity on each outcome of interest was assessed and quantified using the Cochran Q test and the I2 statistic, respectively. The presence of publication bias was evaluated by the use of funnel plots.
Results
Search results
Overall, 228 entries were retrieved for title and abstract analysis. Of these, 169 were excluded as they did not meet inclusion criteria for the meta-analysis. The remaining 59 results were carefully screened, and after analysis of the full text (in the case of journal articles), only 14 studies (nine full text papers9 ,15–22 and five conference abstracts23–27) were deemed adequate for our review's purpose. The stepwise selection process is illustrated in figure 1. There was a good agreement between investigators on the inclusion of the selected trials.
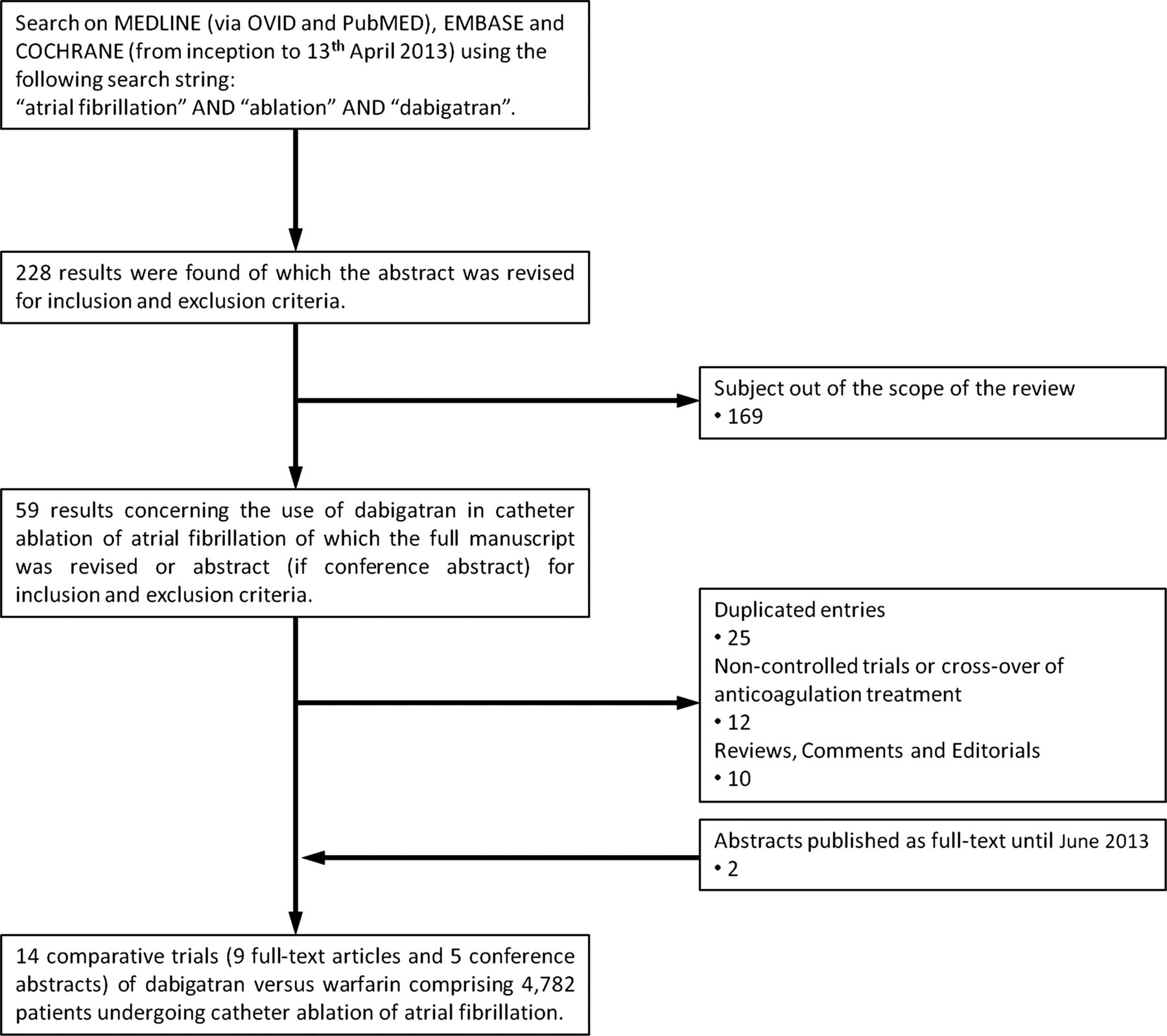
Flowchart diagram illustrating study selection.
Baseline data and the design of selected trials are summarised in tables 1 and 2. The final population for this meta-analysis was composed of 4782 patients (1823 treated with dabigatran and 2959 with warfarin). Table 3 illustrates the assessment of the included studies through the Delphi criteria for randomised studies and the Newcastle–Ottawa Scale for non-randomised case–control studies.
Baseline characteristics of included studies
Description of periprocedural anticoagulation
Assessment of the quality of included studies: Delphi criteria for randomised studies and Newcastle–Ottawa Scale for non-randomised case-controls studies
The observed I2 values showed a low to moderate heterogeneity in the main end point comparisons (I2=0 for stroke and 41% for major bleeding).
Efficacy and safety of dabigatran versus warfarin
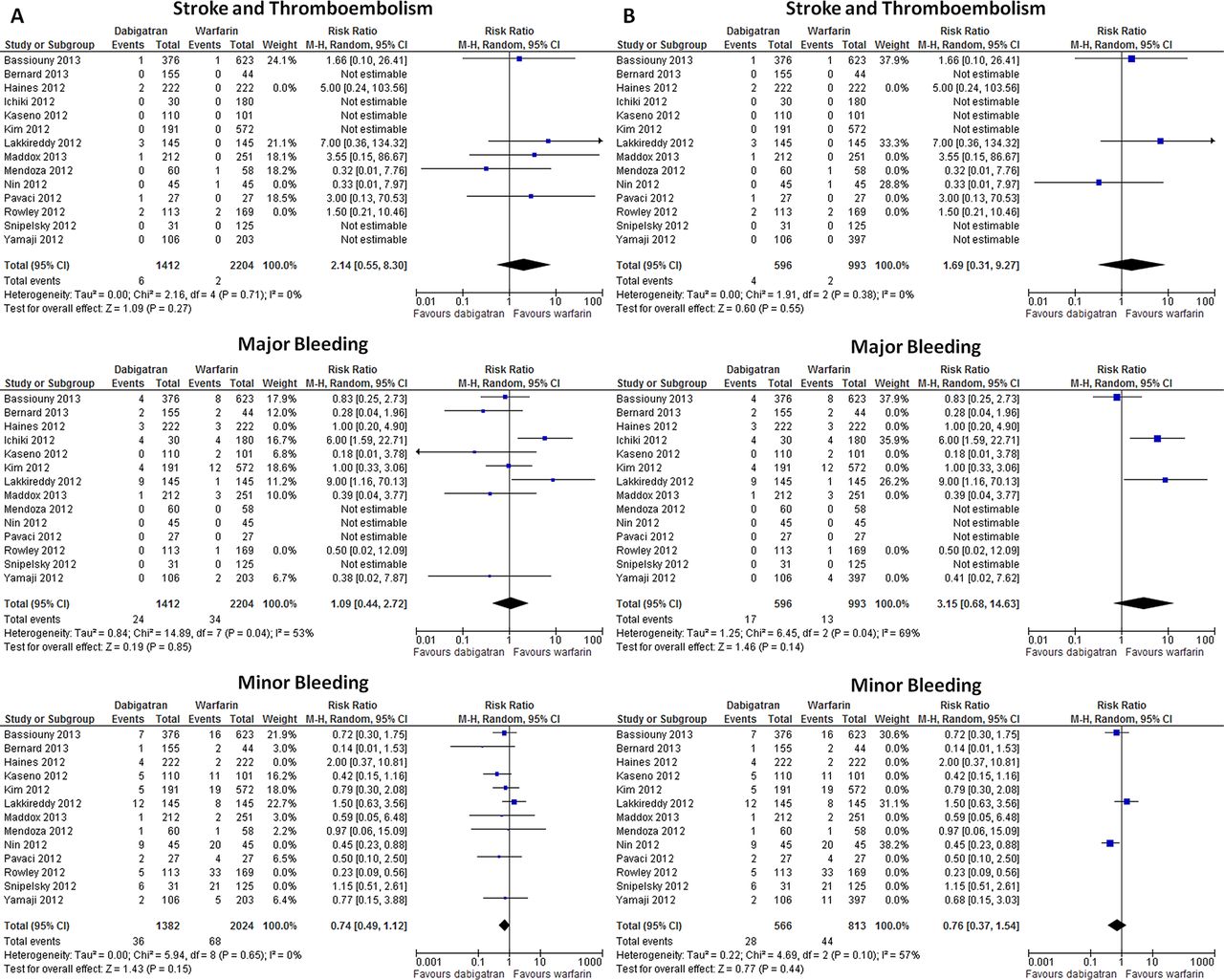
The main efficacy and safety outcomes (prevention of embolism and major bleeding) observed in the comparison between dabigatran and warfarin are displayed in figure 2 and table 4. The funnel plot to ascertain publication bias is shown in figure 3.
Comparison of endpoints across studies

Main efficacy and safety outcomes of the comparison of dabigatran versus warfarin among patients with atrial fibrillation treated with catheter ablation. (A) Stroke and thromboembolism. (B) Major bleeding. M-H, Mantel–Haenszel.
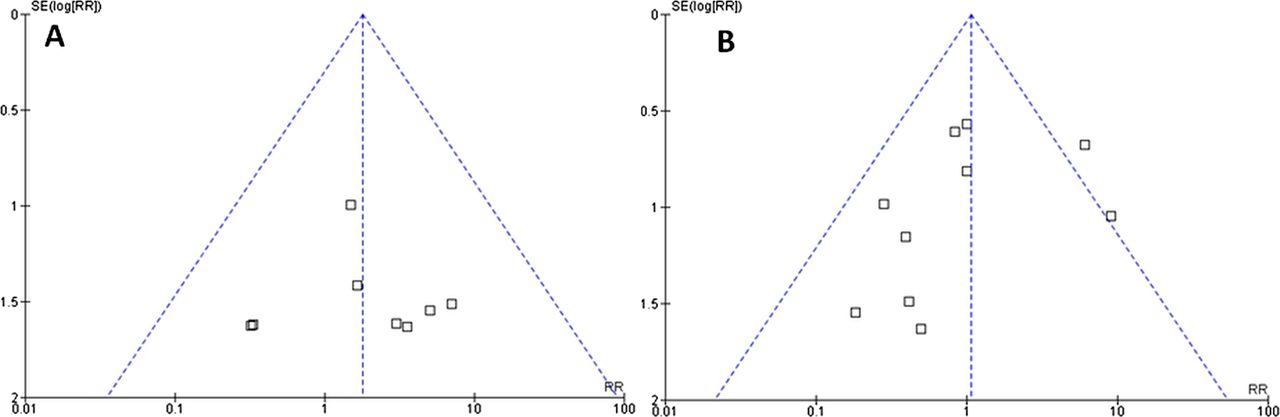
Funnel plots representing the studies used in the assessment of: (A) stroke and thromboembolism; and (B) major bleeding. The inverted and symmetrical funnel aspect can be observed for the assessed end points, with 95% of the studies lying within the confidence limit lines. This suggests that publication bias is not present among the selected studies for the meta-analysis.
Death and thromboembolism
No deaths were observed in any of the intervention groups. Thromboembolic events were reported in only 0.31% of patients (15 out of 4782) and no significant differences were found between dabigatran and warfarin: 0.55% vs 0.17%, respectively (RR=1.78, 95% CI 0.66 to 4.80; p=0.26).
Major bleeding
Among all 14 studies, 67 events (accounting for an overall 1.40% incidence) of major bleeding were reported, with no significant differences observed between the two treatment arms (1.48% dabigatran vs 1.35% warfarin; RR=1.07, 95% CI 0.51 to 2.26; p=0.86).
Minor bleeding
Information on minor bleeding was not reported in one of the selected studies.24 In the remaining, comprising 4572 participants, 210 minor bleeding events (overall incidence 4.59%; 3.35% dabigatran vs 5.40% warfarin) were reported, with a relative risk reduction of 35% (95% CI 7 to 55%; p=0.02) in favour of dabigatran (figure 4).
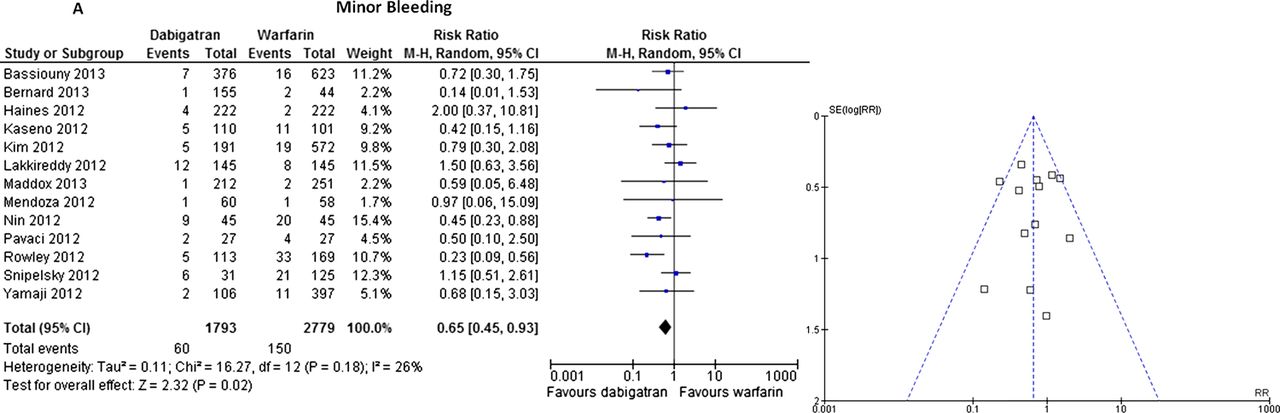
Incidence of minor bleeding among patients treated with dabigatran or warfarin. (A) Forest plot. (B) Funnel-plot. M-H, Mantel–Haenszel.
Sensitivity analysis
Sensitivity analysis confirmed the lack of interference of uninterrupted warfarin, prospective studies, full text articles, studies whose follow-up was at least 30 days, and higher methodological quality studies (figures 5⇓–7) in the overall results concerning the main end points: stroke and thromboembolism and major bleeding. However, as regards minor bleeding these analyses suggested a lack of significant differences.

Forest plot illustrating the sensitivity analysis restricting data to: (A) trials whose patients were treated uninterrupted warfarin; and (B) prospective studies. M-H, Mantel–Haenszel.

Forest plot illustrating the sensitivity analysis restricting data to: (A) investigations published as full text articles; and (B) studies whose follow-up was at least 30 days. M-H, Mantel–Haenszel.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Forest plot illustrating the sensitivity analysis restricting data to higher quality full text articles (Delphi criteria or Newcastle–Ottawa Scale ≥5). M-H, Mantel–Haenszel.
Effect of dabigatran dosage: 150 mg twice daily vs 110 mg twice daily
Information on the dose of dabigatran used was available for 1392 patients (155 with 110 mg twice daily and 1237 with 150 mg twice daily). No significant differences were found between the two dosage groups (110 mg twice daily vs 150 mg twice daily, respectively) regarding major bleeding (0% vs 1.62%; RR=0.19, 95% CI 0.01 to 3.18; p=0.25) and thromboembolism (0% vs 0.40%; RR=0.72, 95% CI 0.04 to 12.98; p=0.82). Concerning minor bleeding, more events were observed with the 110 mg twice daily dosage: 9.03% vs 2.51% (RR=3.60, 95% CI 1.96 to 6.62; p<0.0001).
Management of periprocedural anticoagulation
The different periprocedural regimens used in patients treated with dabigatran are displayed in table 2. The timing of the first withheld dose ranged from the morning of procedure (in four studies) to 48 h before; the time interval for restarting ranged from 3–4 h (in six studies) to 24 h after ablation. In one study, uninterrupted dabigatran was used.19
One third of all strokes or TIAs were associated with suspension of dabigatran for ≥24 h before procedure (one stroke in Haines et al16 and one stroke and one TIA in Rowley et al27). Additionally, of all stroke and TIA in patients treated with dabigatran, 50% was related to a later timing (≥12 h) for restarting the drug post-procedure (two strokes and two TIAs16 ,27). On the other hand, a higher incidence of major bleeding was reported by Lakkireddy et al,9 where dabigatran was stopped only in the morning of the procedure and restarted 3 h post-procedure. Albeit suggesting a similar safety and efficacy profile, with non-inferiority versus warfarin, data concerning uninterrupted dabigatran results exclusively from one trial.19
Among the patients of the warfarin group, safety and efficacy outcomes were similar irrespective of whether warfarin was continued or interrupted.
In addition, target ACT during procedure was 300–350 s in most studies, >350 s in five,9 ,15 ,19–21 and 250–300 s in one.26 A higher value for target ACT9 ,15 ,19–21 was not associated with a lower incidence of thromboembolic events. Furthermore, in the investigation by Lakkireddy et al9 a higher rate of cardiac tamponade in dabigatran treated patients (9/145) was observed. Importantly, a 3.7% rate of stroke was observed in the single study featuring a target ACT of 250–300 s.26 However, due to the low number of participants, the possibility of a false positive association cannot be excluded.
Discussion
The low rate of thromboembolic complications and major bleeding seen with dabigatran (which was also similar to that observed with warfarin) seems to provide favourable support for its use, as an alternative to warfarin, in the setting of catheter ablation of AF. These results add important information on the use of dabigatran in this setting. They also serve to potentially alleviate some of the concerns raised by the rather unfavourable results in earlier studies (2.1% stroke or TIA and 6.2% major bleeds),9 suggesting that dabigatran significantly increased the risk of bleeding or thromboembolic complications compared with uninterrupted warfarin therapy.
A very low rate of stroke and thromboembolic events was found in this meta-analysis among patients treated with dabigatran (0.55%), similar to what has been found in a recent analysis of Medicare beneficiaries (0.6–0.9%).28 A lower, but not significantly different, prevalence of embolism was found in the warfarin arm of this meta-analysis (0.17%), composed mainly of patients with uninterrupted treatment. This value is similar to the one described by Hussein et al29 in patients with uninterrupted warfarin. Therefore, we think that despite showing similar results compared to warfarin in this meta-analysis (and presenting values for thromboembolic complications similar to what has been reported in large registries of patients using anti-vitamin K agents28), validation of these results in future randomised controlled trials with blinded analysis may be justified. Furthermore, the use of uninterrupted dabigatran may also merit assessment, taking into account the promising results of the recently available study with this treatment regimen.19
The proportion of patients referred for AF ablation who are on longstanding dabigatran therapy is progressively increasing. This is likely to pose new challenges for the practising cardiologist, including the question of performing the procedure without discontinuation of dabigatran. The pooled data in this study from a large sample of patients provides an opportunity to address some of these issues.
In this meta-analysis comprising 14 controlled trials, dabigatran performed similarly to warfarin with regard to major bleeding and thromboembolism. Moreover, no deaths were observed in any of the treatment strategies. These results are in agreement with the favourable profile that was observed in an early observational non-controlled trial by Winckle et al.30 Furthermore, a recent analysis of the US Food and Drug Administration (FDA) Mini-Sentinel database for the period from 19 October 2010 (the date of dabigatran approval) to 31 December 2011, found that bleeding rates associated with dabigatran use during the period of interest did not appear to be higher than those associated with warfarin.31
Though the present analysis suggests a lower rate of minor bleeding with dabigatran, there were pronounced differences in the reporting of this end point across the different studies. Furthermore, on sensitivity analysis these results did not remain significant. Thus, while this result needs to be interpreted with caution, it seems, that at the very least, dabigatran is unlikely to be inferior to warfarin in this regard.
No significant differences in major bleeding and thromboembolism were observed between the two assigned dabigatran dosages. However, the low number of patients in each group (resulting from under-reporting of the dosage used in most selected studies), and the low rate of observed events, limit the extent to which firm conclusions can be drawn. The suggestion of less frequent minor bleeding with the 150 mg twice daily dosage is hard to interpret due to the differences in reporting of this end point and in sample size.
The various transition regimens used in patients treated with dabigatran, and the low number of observed events in each of those, renders difficult the task of establishing an ideal transition regimen in this setting. However, the great inter- and sometimes intra-study variability notwithstanding, certain factors are likely to be important for decision making.
The timing for drug interruption before the procedure must take into account the patient's renal function, as 80% of the drug is excreted by this pathway.
In patients with normal renal clearance, the best option may be drug suspension on the morning of the procedure, or the night before, but always <24 h before the procedure.
If renal function is compromised, the drug should probably be interrupted sooner, depending on the degree of renal dysfunction.
There may be a rationale for restarting dabigatran 3–4 h after assuring haemostasis, considering its short half-life and rapid onset of action.
The target ACT during catheter ablation in patients treated with dabigatran should be between 300–350 s (similar to warfarin), as no additional benefits were found for higher values.
Finally, as there seems to be no inherent advantage of any of the studied dabigatran dosages, the creatinine clearance and bleeding risk (HAS-BLED score) should be taken into account for deciding the dosage to be used.
Limitations
Important strengths of this study include the consistent reporting for thromboembolism (almost absent heterogeneity, I2=0%) across studies. However, there are certain limitations, inherent to any meta-analysis.
First, heterogeneity was observed regarding major bleeding (I2=41%; moderate heterogeneity). This may be explained by the pronounced diversity in ablation strategy, anticoagulation regimen, intraprocedural use of heparin, and follow-up between the incorporated studies. However, heterogeneity was low (I2=12%) in the sensitivity analysis including only higher methodological quality studies, which confirms the small and similar incidence of major bleeding in both treatment arms already suggested by the forest plot that included all studies.
Secondly, as already highlighted, certain comparisons are limited by the low number of subjects and low event rates.
Thirdly, in some cases of abstract related data, even with the best attempts to gather information by directly contacting the authors, some data remained incomplete. However, these were mainly with regard to minor bleeding (a secondary end point) and details concerning periprocedural drug transition; hence, missing data are unlikely to have significantly affected the primary results of the analysis.
Fourthly, only a minority of trials was randomised or prospective and a blinded analysis and/or central adjudication of end points was performed in none (ie, the higher level of data quality). Therefore, these data must be considered preliminary and interpreted with some caution.
Conclusions
The rate of thromboembolic complications and/or major bleeding in patients on dabigatran undergoing AF catheter ablation is low and similar to that seen with warfarin.
These results may suggest the feasibility and safety of AF catheter ablation in patients regularly treated with dabigatran. However, further prospective and randomised studies are still necessary to confirm these findings and clarify which periprocedural regimen can minimise the risk of thromboembolic complications with dabigatran.
References
Footnotes
-
Contributors RP, SB were involved in the conception and design of the study. RP, AB and BC collected all data. RP, JPA, SC, AB, BC, NC, KN, EM and SB have critically revised the obtained data and provided suggestions for the preparation of the first version of the manuscript. RP, SB, EM, KN wrote the first version of the manuscript. RP, JPA, SC, AB, BC, NC, KN, EM and SB carefully and critically revised this version and suggested the necessary changes for its improvement. The final version of the manuscript was revised by RP, JPA, SC, AB, BC, NC, KN, EM and SB and a group discussion was conducted with all authors before the final approval of the manuscript.
-
Competing interests RP has received honoraria for serving as a speaker and consultant for Boehringer-Ingelheim and as a co-investigator in the ENGAGE-AF TIMI 48 trial. There are no conflicts of interest for other co-authors.
-
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Heartbeat