Article Text

Abstract
Hypereosinophilic syndrome (HES) is a heterogeneous group of conditions that is defined at its core by hypereosinophilia (HE) (blood eosinophil count of >1.5×109/L) and organ damage directly attributable to the HE. Cardiac dysfunction occurs frequently in all forms of HES and is a major cause of morbidity and mortality. Once a significantly elevated eosinophil count is identified, it must be confirmed on repeat testing and the aetiology for the HE must be rigorously sought out with a focus on identifying whether organ dysfunction is occurring. Echocardiography is routinely performed to assess for cardiac involvement, looking for evidence of left ventricular and/or right ventricular apical obliteration or thrombi or a restrictive cardiomyopathy. Cardiac magnetic resonance imaging and CT are often useful adjuncts to establish the diagnosis but endomyocardial biopsy remains the gold standard. To decrease the degree of eosinophilia, treatment can include corticosteroids and/or imatinib based on the aetiology. Anticoagulation, standard heart failure therapy for a restrictive cardiomyopathy and finally cardiac transplantation may be indicated in the treatment algorithm.
Statistics from Altmetric.com
Introduction
Hypereosinophilic syndrome (HES) is a group of conditions in which there is an overproduction of eosinophils that subsequently infiltrate and damage multiple organs. Cardiac manifestations, particularly eosinophilic myocarditis (EM) and endomyocardial fibrosis (EMF), are a typical cause of morbidity and mortality in HES. This review will briefly discuss the definition and aetiology of HES with an overview of the clinical cardiac presentations/diagnoses. In addition, a focused discussion of cardiac management and treatment will be reviewed.
Definition
An eosinophil is a granulocyte whose function is not clearly understood, but likely plays a role in host immune response to infection and inflammation. Typically, eosinophils are not normally found in all of the organs (they are seen in the thymus, spleen, gastrointestinal tract, lymph nodes and uterus). The production of eosinophils is controlled by specific cytokines: IL-5, IL-3 and GM-CSF.1 These cytokines are typically produced by activated T lymphocytes, mast cells and stromal cells, and are usually responsible for reactive eosinophilia. Clonal eosinophils are typically derived from mutated progenitors (such as in tyrosine kinase receptors, platelet-derived growth factor receptor β and fibroblast growth factor receptor 1).2 The Year 2011 Working Conference of Eosinophil Disorders and Syndromes (Vienna, Austria; 27–28 May 2011) was tasked with reviewing the criteria for establishing the definition of various disorders related to eosinophilic abnormalities. The goal was to simplify the prior classifications into a contemporary multidisciplinary scheme.2 Hypereosinophilia (HE) is defined as an elevated eosinophil count (>1.5×109/L) noted on two separate tests greater than a month apart or the finding of tissue HE (which includes >20% eosinophils on bone marrow section, extensive tissue infiltration by eosinophils validated by a pathologist or marked deposition of eosinophilic granule proteins in tissue). HE is further subdivided into a hereditary (familial) variant, HE of undetermined significance, primary (clonal/neoplastic) variant and a secondary (or reactive) HE.2 The HESs are then those conditions with peripheral HE for any reason, along with organ damage directly attributed to tissue HE (table 1). The organ damage must be due to HE and not related to an alternative cause. HES can be idiopathic, primary (neoplastic) or secondary (reactive) based on the cause of the HE (table 2). In prior classifications, HES was defined as HE in which an aetiology was not found; the new proposed classification has modified the diagnosis for HE and HES. Primary or neoplastic HES indicate a stem cell, myeloid or eosinophilic neoplasm and are considered clonal. Secondary or reactive HES has multiple potential causes. The HE in these states is caused by an overproduction of eosinophilopoietic cytokines (such as IL-5) and is polyclonal. Parasitic infections are common cause of HE in developing countries3 and can result in HES. Certain solid tumours and T-cell lymphoma where there is HE can also result in end organ dysfunction and damage. HE can occur in other conditions but it is unknown if it is directly related to the disease presentation and complications. These include eosinophilic granulomatosis with polyangiitis (Churg–Strauss) and Hyper-IgE syndrome (an autosomal dominant hyperimmunoglobulin E syndrome often accompanied by eczema and facial abnormalities).2 In upto 75% of cases of HE, an underlying cause is not found; thus, affected individuals are frequently labelled with idiopathic HES.4
Definition of eosinophil abnormalities based on suggested revised classification
Categories of HES
Epidemiology
HESs are rare and the overall incidence and prevalence have not been well characterised. Identifying patients with HES through the Surveillance, Epidemiology and End Results (SEER) database, the incidence was approximately 0.035 per 100 000.5 Over the 5 year period (2001–2005) reported in SEER, the median age at diagnosis was 52.5 with a male to female ratio of 1.47.5 Certain HES variants appear to occur exclusively in males where others have an equal distribution between the sexes.4 Until relatively recently, the prognosis was quite poor, but with recent advances in the management of HES along with the earlier diagnosis and treatment of organ involvement, an 80% survival at 5 years and a 42% survival at 10–15 years has been reported.6
Pathophysiology/Clinical presentation
The extensive infiltration of eosinophils into tissues can in and of itself cause damage if the proliferation is significant enough, but the organ damage may occur through an associated fibrosis.7 Activated eosinophils may cause tissue damage through the release of toxic granules, release of cytokines or recruitment of inflammatory cells.8
As HES can be a multisystem condition, patients may present with signs and symptoms related to any organ system. Typically symptom onset evolves slowly and can be very nonspecific. Weakness, fatigue, cough, myalgias, shortness of breath, rash and diarrhoea may be presenting complaints.2 There is significant heterogeneity in the extent and degree of organ involvement in a given individual.4 A rash and cough/dyspnoea are the two most common symptoms followed by gastrointestinal disturbances. Cardiac and neurologic signs and symptoms are rarer but potentially life threatening due to rapid progression of complications.4 Eosinophilic cardiac disease was first described in 1936 by Wilhelm Loffler who described a ‘fibroplastic parietal endocarditis with blood eosinophilia’ that is consistent with the EMF seen in HES at later stages. Historically, cardiac involvement was felt to be present in up to 40%–50% of HES9 ,10 but may be even higher.11 Cardiac disease is a major cause of morbidity and mortality.6 ,12 ,13 A more recent retrospective review over a 19-year period, identifies cardiac dysfunction as the major cause of death in 247 HES patients.11 The cardiac pathology of HES has been divided into three stages: (1) an acute necrotic stage, (2) a thrombotic stage and (3) a fibrotic stage (table 3). The development of the cardiac disease in HES can be unpredictable and the stages may overlap.12 Sustained eosinophilia does not necessarily always equate to the development of EM and conversely, the degree of cardiac dysfunction does not directly correlate with the degree of eosinophilia.
Stages of cardiac pathology in HES
The first phase of acute necrosis is the result of EM. Eosinophils and lymphocytes infiltrate cardiac tissue, releasing toxic proteins from degranulating eosinophils.14 ,15 At this stage, myocardial necrosis and apoptosis occurs. However, typically no cardiac symptoms are endorsed by patients at this stage. However, due to small microemboli that may form on the endocardial surface, conjunctival or subungual splinter haemorrhages may be identified.12 Rarely, a more fulminant course of EM may occur that can be rapidly fatal without early diagnosis and treatment.12
The second stage occurs when thrombus forms along the damaged endocardium. Thrombus formation occurs due to multiple reasons but is likely directly the result of the disrupted endothelium, exposing von Willebrand factor and collagen which bind platelets and tissue factor (which are vital for the development of fibrin thrombus).15 The thrombi most often develop within both ventricles, typically at the apex but may extend toward the base of the heart into the subvalvular regions and less commonly the outflow tracts.16 These thrombi can them embolise causing strokes and ischaemic extremities.17 ,18 Overall, it appears that up to 25% of patients with HES develop thromboembolic complications and that 5%–10% die from those complications.15
The final cardiac stage is one in which fibrosis replaces the thrombi on the denuded endocardium. EMF leads to scarring. A restrictive cardiomyopathy develops, with symptoms of dyspnoea and signs of left-sided or right-sided heart failure.18 ,19 Restriction of the valve leaflets from fibrosis results in valvular regurgitation, with mitral regurgitation seen most commonly.16 The fibrosis is irreversible and may be the point at which the patient is first diagnosed with HES.
The clinical presentation for cardiac involvement as noted above can vary depending on the stage of myocardial damage. Cardiac involvement correlates with the occurrence of embolisation, clinical heart failure and need for cardiac surgery and can be confirmed with echocardiography.9 In an older review, more than half of the patients with HES and cardiac pathology, presented with dyspnoea; chest pain and cough were seen less often. In that same review, 75% of patients who were evaluated had signs and symptoms of heart failure.18 Arrhythmias may occur as a result of fibrosis of the conduction system or due to the scarring of the myocardium. Myocardial infarctions are rare but can occur as the result of an embolic phenomenon from the left ventricular (LV) apex or outflow tract. Cardiac symptoms typically evolve over weeks to months but can be more prolonged than that.9
It is important to note that EM can occur separately for HES. The aetiologies are varied and include malignancy, hypersensitivity myocarditis (HSM), parasitic infections and eosinophilic granulomatosis with polyangiitis (formerly referred to as Churg–Strauss). Pathologically, EM is characterised by myocardial inflammation with eosinophils, often with associated eosinophilia, not necessarily HE, and is distinct in its presentation as it is often more acute than indolent.20 HSM is an autoimmune reaction in the heart, typically related to a drug reaction and can present as rapidly progressive heart failure or sudden death. Multiple drugs have been implicated and patients frequently have fever, rash, ECG abnormalities and peripheral eosinophilia. On myocardial biopsy, the pattern is one of interstitial infiltrate with eosinophils but with minimal cell necrosis.21 EMF can be a separate syndrome in which fibrosis typically at the apices of the left and/or right ventricles (RV), presents with symptoms related to a restrictive cardiomyopathy (with left-sided and right-sided heart failure).22 Although EMF resembles the late stages of the cardiac involvement in HES, there is not a consistently identified serum or myocardial eosinophilia.23 Whether transient eosinophilia is the culprit is unclear. Infectious and/or environmental aetiologies have been implicated.24
Diagnosis
Per the definition for HES, there must a peripheral eosinophilia (eosinophil count >1.5×109/L) or tissue HE (figure 1). This elevation in eosinophils must be present on two separate laboratory tests at least 1 month apart. A careful review of the individual's history for travel to determine parasitic exposure, complete review of medication usage along with a thorough history and exam are important to determine causes for HE. Even if asymptomatic, the patient with HE requires a comprehensive evaluation to assess for presence and degree of organ involvement. This may dictate the urgency of other testing as well as potential aetiologies. Initial testing could include some of the following: a complete blood count, serum vitamin B12 levels, serum immunoglobulins, peripheral blood smear, serum chemistries, creatinine, liver function tests, chest X-ray, ECG, troponin level (which has been shown to correlate with the presence of cardiomyopathy25) and stool samples or serology for parasites (for those from endemic areas or with a travel history). Assessing for organ involvement is important to establish the diagnosis of HES over HE alone. This evaluation would include further testing with pulmonary function testing, echocardiography, abdominal imaging (CT most commonly) and tissue biopsies as appropriate. As part of the haematological assessment, peripheral blood screening would be undertaken and possibly bone marrow biopsy with tissue typing for the characterisation of the aetiology of the HE. There are many variants that would be screened for to assess for clonal aetiologies. One myeloproliferative variant (Fip1-like1-platelet-derived growth factor receptor α (FIP1L1-PDGFRA) fusion), which has a poor prognosis, is characterised by elevated serum tryptase which is of importance from a treatment standpoint.25 This particular cause of HES has an increased incidence of more profound cardiac disturbances with greater mortality without treatment.26

Shown are focal intact eosinophils in myocardium, and focal intact and degranulated eosinophils within fresh (probably biopsy-related) thrombus, suggestive of eosinophilic heart disease.
Cardiac diagnosis is typically initially suspected based on signs and symptoms of cardiac dysfunction. ECG is typically nonspecific and can consist of T-wave inversions, left atrial enlargement, LV hypertrophy, premature ventricular complexes or first degree atrioventricular block.18 These changes indicate some potential underlying cardiac abnormality but are not specific for HES. Echocardiography is a critical diagnostic tool in the evaluation of cardiac disease in HES. During the initial stage of cardiac involvement (necrotic stage of EM), echocardiography is typically normal, although wall thickening may be identified if there is significant oedema within the myocardium due to the inflammatory process. In the thrombotic stage, thrombi can be identified within the apices of either the LV or RV or both (figure 2). The appearance can be mistaken for LV noncompaction, apical hypertrophic cardiomyopathy (HCM) or even typical LV apical thrombus due to an apical wall motion abnormality. The use of contrast agents, to better define the apex, can help differentiate thrombi from apical HCM and noncompaction and can also reveal the preserved systolic function at the apex in HES that distinguishes it from an apical infarction with thrombus27 (figure 3). Three-dimensional echocardiography may improve visualisation of the apices and identify thrombus in lieu of a contrast agent. The progression from thrombus to fibrosis is not well identified specifically on echocardiography but does have change in the clinical presentation (more heart failure symptoms vs embolic phenomena). The apices remain obliterated but now with fibrosis and less so with thrombus. It is at this stage that valvular regurgitation may be better identified. The posterior leaflet of the mitral valve can become thickened and adherent to the underlying endocardium of the posterobasal wall, restricting its motion. The mural thombofibrotic material between the posterior mitral leaflet and posterobasal LV wall limit the excursion of that leaflet and ultimately tether it (figure 4 Significant mitral regurgitation can be seen and is typically posteriorly directly due to the restricted motion of the posterior leaflet. In addition, a restrictive cardiomyopathic picture emerges with characteristic mitral valve Doppler indices of poor LV compliance and elevated filling pressures (figure 5). This restrictive physiology is typically related to the endocardial/myocardial fibrosis that occurs; however these hemodynamics may be seen due to the small LV cavity caused by a large noncompliant apical ‘mass’.28 There is limited data on the use of myocardial strain imaging to assess systolic function in patients with EM but it may be helpful to differentiate a true restrictive cardiomyopathy from merely restrictive filling.28

Transthoracic echo imaging: apical four-chamber view demonstrates a large thrombus filling the left ventricular cavity.

Transthoracic echo imaging: (A) (left) demonstrates an apical four-chamber view. Contrast echocardiography clear delineates thrombus present at the left ventricular apex (white arrow points to black defect of thrombus). (B) Shows the corresponding parasternal short-axis view and also highlights the benefit of contrast echocardiography at identifying thrombus (white arrow).
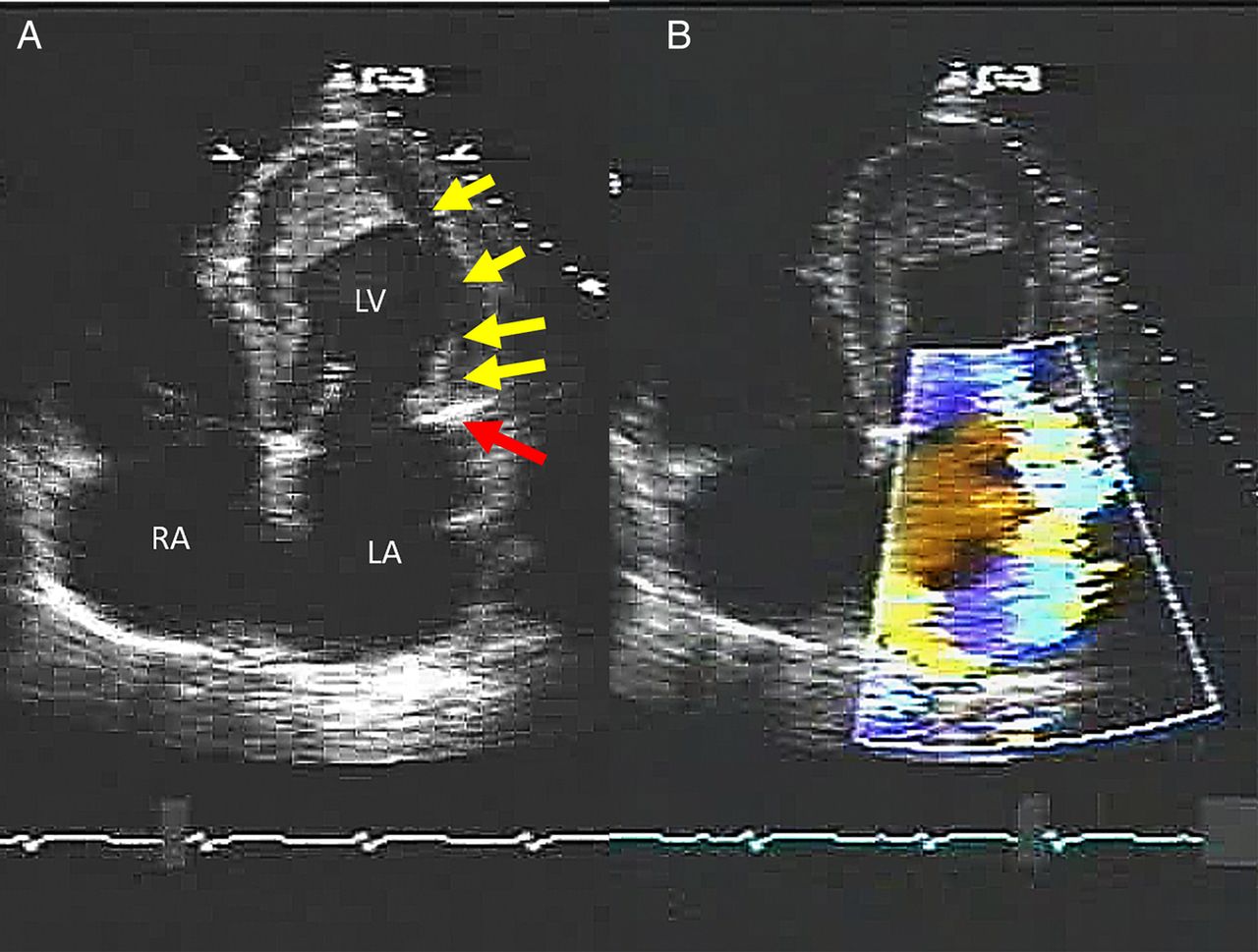
Shown in (A) to the left, is an apical four-chamber view demonstrating the endomyocardial fibrosis extending along lateral wall of the ventricle (yellow arrows) all the way down to the posterior mitral leaflet (red arrow). The posterior mitral valve leaflet has suffered direct tissue injury and now demonstrates reduced leaflet excursion leading to severe eccentric mitral regurgitation shown in (B) to the right (RA, right atrium; LA, left atrium; LV, left ventricle). Image courtesy of Dr Natesa G Pandian.

Shown is the characteristic mitral Doppler inflow pattern of a restrictive cardiomyopathy pattern (A, left). The mitral valve deceleration time is 105 ms, with a peak early inflow velocity of 1.1 m/s. The mitral annular tissue Doppler (B, right) also demonstrates classic findings of a restrictive cardiomyopathy with a markedly reduced early diastolic longitudinal relaxation velocity (0.04 m/s).
Cardiac magnetic resonance (CMR) imaging has emerged as a newer modality for the diagnosis of cardiac disease in HES.29–31 CMR can detect ventricular thrombi with a higher degree of sensitivity and specificity than echocardiography and in addition contrast-enhanced CMR can identify inflammation and fibrosis (figures 6 and 7).31 ,32 Thus, CMR may be able to detect myocardial abnormalities in the early stages of the cardiac involvement in HES (the acute myocarditis/necrotic stage) prior to echocardiographic abnormalities. CMR can be an important adjuvant imaging tool that may be useful in following the cardiac disease course.33 CT imaging has been described as a potential tool as well to identify LV thrombus and concomitantly assess for coronary artery disease as a potential culprit for the presence of apical thrombus.34

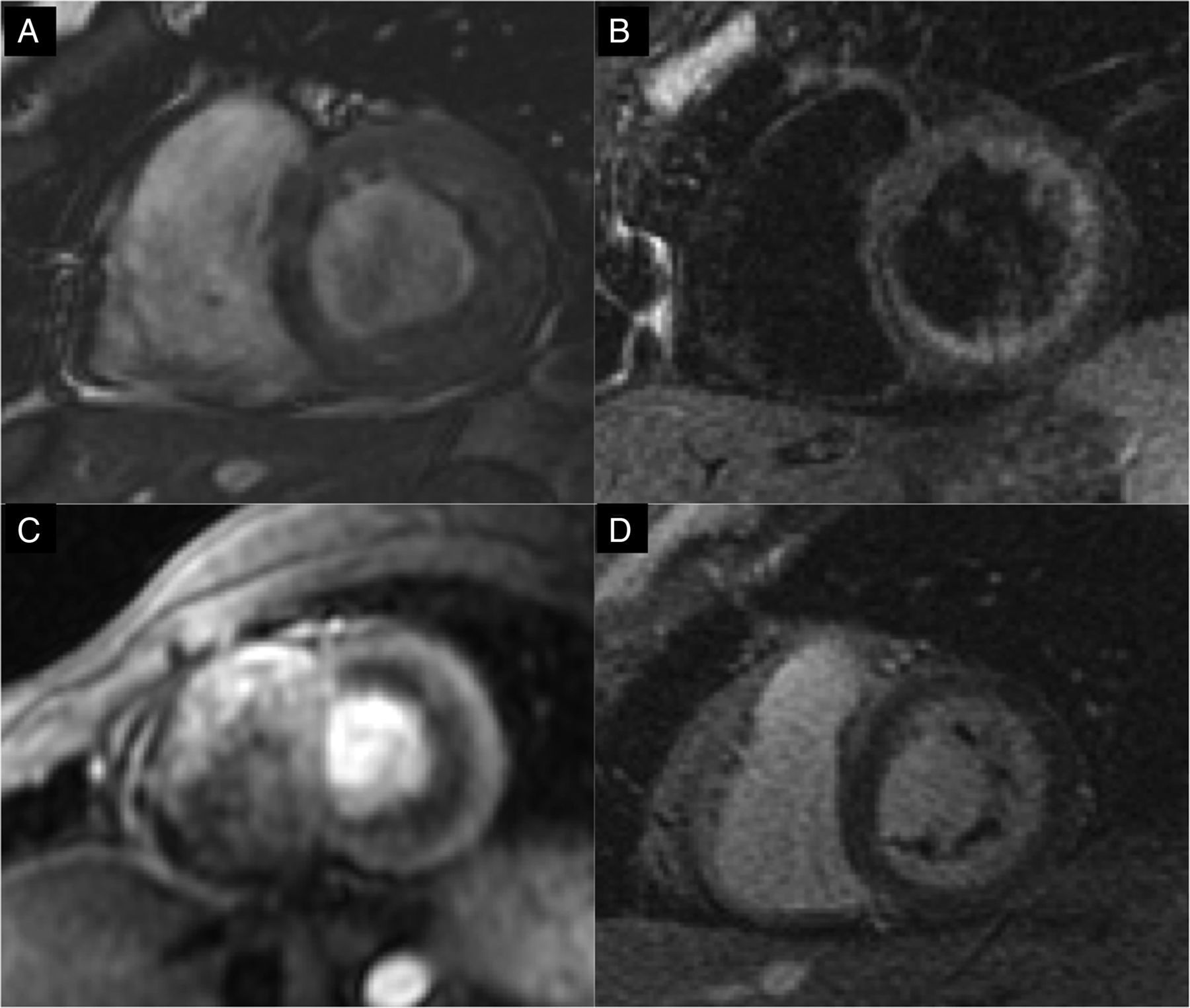
Selected short-axis images from cardiac MRI study in a patient with eosinophilic myocarditis. (A) Steady state free precession (SSFP) imaging demonstrates marked thickening of the anterior, lateral and inferior walls of the left ventricle. (B) Marked increase in T2 signal involving the same walls that were thickened on SSFP imaging, suggesting oedema. (C) First pass perfusion imaging demonstrates an inner rim of non-enhancing thrombus. (D) Delayed enhancement imaging demonstrates hyperenhancement involving the subendocardial region with associated nonenhancing rind of thrombus along the subendocardial surface.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Delayed enhancement images demonstrating intense hyperenhancement of the subendocardial surface with a large, nonenhancing thrombus filling the left ventricular cavity.
However, despite the importance of the noninvasive imaging tools, endomyocardial biopsy (EMB) remains the gold standard for the diagnosis of cardiac involvement in HES, particularly early in the course to differentiate EM from other forms of myocarditis. Serial EMB can be used to assess course and treatment response. Infiltration of eosinophils into the myocardium may be detected; however, more often fibrosis, mural thrombus and inflammation of intramural coronary vessels are detected.35 However, it must be recognised that EMB may be negative if the process primarily involves the LV rather than the RV.9
Management of HES cardiac disease
HE has multiple potential treatment options, based on the aetiology. The management of cardiac disease in HES is to normalise the damaging HE. Corticosteroids are one of the cornerstones of therapy for HES to reduce eosinophil count and counteract inflammation.36 Patients with the FIP1L1-PDGFRA mutation should be treated with a tyrosine kinase inhibitor (imatinib) given its possible effectiveness37 along with steroids (with cardiac involvement, steroids should be used along with the imatinib to prevent the occurrence of acute heart failure from necrotising myocarditis).38 The haematological abnormalities can remiss with this treatment but advanced cardiac disease may not be affected. Other second line treatment options are available for refractory cases.
Echocardiography should be used to follow documented cardiac disease at relatively frequent intervals (<6 months).15 If no cardiac abnormalities are seen initially in the evaluation of HES, repeat evaluation and imaging should take place at least every 6 months.11 LV or RV thrombi or embolic phenomena would indicate the need for anticoagulation therapy. The duration of the therapy is best determined by the ongoing presence of ventricular thrombi along with the status of the endomyocardial disease activity. There is no data to suggest that prophylactic use of anticoagulation can alter the progression of the disease.15 Congestive heart failure should be managed by current heart failure guidelines, which include diuretic therapy, β blockade, ACE inhibitors to name a few.
Valvular disease that is significant and contributing to ongoing heart failure symptoms may require surgical intervention. Given the rarity of HES, there is limited data in regard to valve surgery in these patients. However, both valve repair and valve replacement have been described.39–41 Replacement appears to be more common than repair. The type of valve used, mechanical versus bioprosthetic, is an important consideration in this group of patients. There appears to be a high risk of valve thrombosis in the mechanical valve group despite anticoagulation.42 Thus, bioprosthetic valves may be the better option; however, this may require a repeat procedure due to valve deterioration, particularly in a relatively young patient. It is important that the eosinophilia be controlled prior to valve surgery. In the setting of a restrictive cardiomyopathy with refractory symptoms, heart transplantation may be considered. Limited data are available but has been reported.43
Conclusion
HES is a rare condition that may have several aetiologies. Cardiac involvement is frequent and carries with it a high rate of morbidity and mortality. Identifying cardiac dysfunction early and following it serially can help determine treatment approaches in a timely fashion. Echocardiography is an integral part of the diagnosis of cardiac involvement but CMR appears to have an important role. Overall prognosis has improved for HES, but limited data exist on the best course for cardiac disease.
References
Footnotes
Twitter Follow Rekha Mankad at @RMankadMD and Sunil Mankad at @MDMankad
Contributors All authors contributed in a significant manner to the writing of this manuscript.
Competing interests None declared.
Provenance and peer review Commissioned; externally peer reviewed.