Article Text

Abstract
Background: There is evidence that new portable echocardiographic devices are useful in evaluating heart anatomy and function, but a lack of Doppler modes has up to now been an important limitation in obtaining haemodynamic data.
Objectives: To report the Doppler capabilities of a new hand held echocardiographic device.
Design: Blinded comparison of two types of echocardiography machine.
Setting: Tertiary care centre.
Patients: 98 consecutive patients were randomly imaged with the hand held device, with a standard platform as reference.
Outcome measures: Pulsed wave transmitral Doppler inflow tract velocities, deceleration time, and continuous wave Doppler measurements of aortic ejection and tricuspid regurgitation peak velocities were recorded.
Results: There was excellent agreement between the hand held device and standard echocardiography for the evaluation of diastolic E and A waves, E/A ratio, and deceleration time with pulsed wave Doppler (intraclass correlation coefficients of 0.97, 0.93, 0.90, and 0.78, respectively). In addition, good agreement was found between continuous wave Doppler measurements of aortic ejection and tricuspid regurgitation velocities (intraclass correlation coefficients of 0.96 and 0.80). However, there was a significant difference between patients with tricuspid regurgitation measured with the hand held device (25.5%) and by standard echocardiography (65.3%), resulting in misdiagnosis of eight patients with pronounced pulmonary hypertension.
Conclusions: New hand held devices with Doppler capabilities overcome previous limitations in evaluating haemodynamic variables. With colour Doppler they are now suitable for the complete evaluation of valvar disease and diastolic function. However, important limitations remain in the evaluation of pulmonary pressures.
- echocardiography
- Doppler
- point of care system
Statistics from Altmetric.com
Echocardiography is the most widely used imaging technique for assessing cardiovascular anatomy and function. It is an evolving technology in a rapid phase of development and improvement. The more widespread use of echocardiography was limited by the size and cost of the machines until the arrival of new miniaturised hand held echocardiographic devices.
Previous studies of hand held devices showed that their diagnostic ability was superior to physical examination1 and that they had good accuracy when compared with standard echocardiographic platforms.2–7 However, there were important limitations in their assessment of haemodynamic data and valve function because of the absence of pulsed and continuous wave Doppler facilities.
Doppler capabilities have now been introduced into hand held devices, along with other improvements (M mode imaging, ECG synchronisation, storage memory, and multiple peripheral connections), which may help to overcome these limitations. Our study was designed to evaluate the accuracy of Doppler measurements made with a hand held device in comparison with standard echocardiography, and to assess the agreement between the two types of equipment.
METHODS
Hand held device
We used the SonoHeart Elite (SonoSite Inc, Bothell, Washington, USA) portable echocardiographic system. The device has an integrated 12.7 cm TFT colour liquid crystal display with brightness and contrast controls, is 33.8 cm in height, 19.3 cm in width, and 6.35 cm in depth, weighs 2.6 kg, and is battery (rechargeable lithium ion) or AC mains powered. It is equipped with a 15 mm broadband (4–2 MHz) phased array transducer for transthoracic imaging and delivers continuous and pulsed wave Doppler. Together with Doppler capabilities, SonoHeart offers cross sectional images enhanced by extended resolution harmonics and synchronised to the patient’s ECG, along with M mode and directional colour power Doppler. Control settings resemble the standard platform and it has an internal storage memory of up to 119 images. It can be connected to a videocassette recorder, video printer, or external monitor. In order to expedite calculation it is provided with an integrated trackball for navigation, two sets of distance callipers, and a cardiac calculation software package.
Standard echocardiography
Standard echocardiography was done using Sonos 5500 (Philips Technologies, Andover, Massachusetts, USA) and Acuson Sequoia 256 (Siemens Technologies, Mountain View, California, USA) instruments, both equipped with harmonic imaging, pulsed and continuous wave Doppler, and multifrequency transducers.
Study population
We studied 98 consecutive unselected patients (50 female, 48 male; mean age 64.2 years), referred to the echocardiography laboratory for a transthoracic echocardiogram. Patients enrolled were referred by their physician and were either admitted to hospital or seen in outpatients. The indications for referral were: 23 patients for ischaemic heart disease, 17 with hypertension, 16 being investigated for arrhythmias, 12 with valvar heart disease, 9 to clarify a cardiac murmur, 6 for heart failure, and 15 for miscellaneous indications.
Study design
To test Doppler accuracy of the hand held device, we did a validation study based on a side by side comparison with standard echocardiography measurements of pulsed and continuous wave Doppler. All patients underwent two consecutive echocardiographic examinations by two cardiologists with experience in echocardiography (expertise level II according to the American Society of Echocardiography8).
Patients were first imaged with the hand held device and immediately after, a second investigator did the standard examination, blinded to the results of previous study. Both undertook a complete cardiac examination based on the parasternal long and short axis views and apical two, three, and four chamber views.
Diastolic left ventricular inflow tract velocities were obtained using pulsed wave Doppler echocardiography by positioning the sample volume at the tip of the mitral leaflets from the apical four chamber view, following recommendations of the American Society of Echocardiography.9 Measures of the E and A wave velocities (in sinus rhythm), their ratio, and the deceleration time of the E wave were recorded.
Continuous wave Doppler measurements of maximum velocities of aortic ejection and tricuspid regurgitation were obtained from the apical five chamber and apical four chamber view, respectively, maintaining as far as possible a parallel orientation between the sound beam and the blood flow.9
As a secondary objective, haemodynamic information obtained after transformations of continuous wave Doppler measurements was compared in order to calculate the sensitivity and specificity of the hand held device in evaluating aortic stenosis and pulmonary hypertension. Aortic and tricuspid regurgitation velocities were transformed into pressure gradients by applying the simplified Bernoulli equation: pressure gradient = 4V2.
Aortic maximum velocities were recoded into mild, moderate, and severe aortic stenosis according to preset limits (250–350 cm/s mild, 350–400 cm/s moderate, and > 400 cm/s severe aortic stenosis). Right ventricular systolic pressure was calculated as described previously.10 It was assumed to be identical to systolic pulmonary artery pressure when the absence of a gradient across the pulmonary valve and normal morphology of the right ventricular outflow tract could be demonstrated. Pronounced pulmonary hypertension was defined as a calculated systolic pulmonary artery pressure ⩾ 50 mm Hg, and the patients were classified into two groups: those with a pressure ⩾ 50 mm Hg, and those with a lower pressure.
To compute interobserver variability, the investigator who operated the hand held device retrieved standard echocardiographic videotapes and reported upon several sets of cross sectional data and measurements, blinded to patient identity, in a way described previously.2,5
Statistical analysis
Descriptive statistics are reported as medians and interquartile ranges, owing to a non-normal distribution of variables. Agreement between Doppler measurements was assessed with reliability analysis using intraclass correlation coefficients,11,12 considering values below 0.4, between 0.4 and 0.75, and above 0.75 to represent poor, fair to good, and excellent agreement, respectively. As neither of the two devices compared provides an unequivocally correct measurement, we also assessed the degree of agreement using a graphical technique described by Bland and Altman.13,14
Agreement between data reported in a categorical way was appraised using a linearly weighted κ index,15 considering values ⩽ 0.2, 0.21–0.4, 0.41–0.6, 0.61–0.80, and ⩾ 0.81 to represent poor, fair, moderate, good, and excellent agreement.
RESULTS
Pulsed wave Doppler
Measurement of the E wave was feasible in all patients with the standard echocardiographic device and in all except two with the hand held device. After exclusion of patients with atrial fibrillation, the A wave was measured in all the remainder with standard echocardiography, and in all except three with the hand held device. An E/A ratio was then computed if both measures were available. Table 1 summarises the results of the measurements of pulsed and continuous wave Doppler. The median (interquartile range) for E wave measurements was 77 (36.5) cm/s with the standard platform and 76.5 (34.7) cm/s with the hand held device; A wave measurements were 79 (40) cm/s with the standard platform and 79.5 (31) cm/s with the hand held device. The E/A ratios calculated with the standard device and with the hand held device were 0.9 (0.6) and 1.0 (0.5), respectively. Excellent agreement between measurements with both devices was found, with intraclass correlation coefficients of 0.97, 0.93, and 0.9 for the E wave, A wave, and E/A ratio, respectively.
Doppler measurements with standard echocardiography and with a hand held device
Using pulsed wave Doppler we assessed the deceleration time interval and found good agreement between the two devices: 216.8 (123.8) ms with the standard device and 242.4 (119.5) ms with the hand held device, with an intraclass correlation coefficient of 0.78.
Continuous wave Doppler
Measures of aortic forward maximum velocity and tricuspid regurgitation maximum velocity with both examination techniques are shown in table 1.
The median value of continuous wave Doppler velocities obtained with the standard device was higher than that obtained with the hand held device; nevertheless, agreement between the two techniques was excellent (intraclass correlation coefficients of 0.96 and 0.8 for aortic forward and tricuspid regurgitation peak velocity, respectively).
Information obtained after transformation of continuous wave Doppler aortic measurements is shown in table 2. A 96% agreement was found, with a weighted κ of 0.86 (excellent agreement), but a one grade underestimation of the degree of severity of aortic stenosis with the hand held device was encountered in four patients.
Agreement over classification of aortic stenosis severity, assessed by peak aortic velocity, between standard and hand held echocardiographic devices
A significant difference was found between the number of patients with tricuspid regurgitation measured with the hand held device (23.5%) and with standard echocardiography (65.3%).
As shown in table 3, among the 23 patients measured by both devices, three had pronounced pulmonary hypertension and all of these were appropriately classified with the hand held device. However, among the remaining patients only measured by standard echocardiography, eight with pronounced pulmonary hypertension were misdiagnosed.
Presence or absence of pronounced pulmonary hypertension (⩾50 mm Hg) classified according to peak tricuspid regurgitation velocity measured with both standard and hand held echocardiographic devices
Graphical analysis
Figures 1 and 2 show the graphical method described by Bland and Altman13,14 to compare a new method of measurement with an established technique. The plot of differences against the mean of measures obtained with both devices allows us to check the distribution of the differences within two standard deviations, offering limits of agreement between the echocardiographic devices compared.

Bland-Altman plot, showing the differences between pulsed wave Doppler measurements by hand held echocardiography and standard echocardiography. The mean of the differences and 1.96 standard deviations (SD) of the mean difference are shown.
{kind=link}
{kind=link}
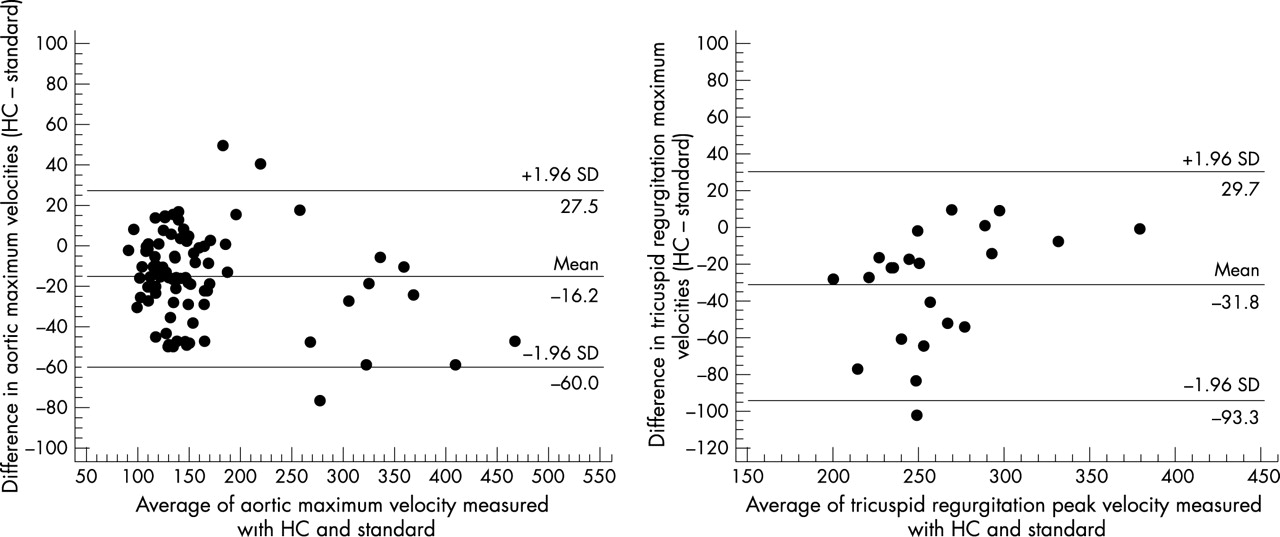
Bland-Altman plot showing the magnitude of the difference between continuous Doppler measurement of aortic maximum velocity and tricuspid regurgitation velocity measured by hand held echocardiography and standard echocardiography. 1.96 (SD), 1.96 standard deviations of the mean difference.
Figure 1 shows the graphical analysis of pulsed Doppler E and A waves. The mean of the differences of the measurements with both methods stands near the null value and the agreement limits are around ±25–30 cm/s, being tighter for measuring the E wave than the A wave. Limits of agreement for continuous Doppler measurements (fig 2) oscillate between −93 and −60 cm/s (lower limit) and between 27 and 30 cm/s (upper limit), being wider for measuring maximum velocities in tricuspid regurgitation. The mean of the differences between the two devices is negative, implying lower values with the hand held device.
Interobserver variability
There was a good correlation between the two independent investigators, with an interobserver variability of 3%.
DISCUSSION
Echocardiography is a widely used technique in cardiology and supplies accurate anatomical and functional data. The use of Doppler echocardiography provides unique haemodynamic information which would not otherwise be available without invasive monitoring. To date, the widespread use of this technique has been limited by the size and cost of the equipment. However, miniaturisation in the form of hand held ultrasound imagers the size of a laptop computer and digital technology may overcome these barriers. Several hand held ultrasound units have been developed for point of care cardiac examination, aiming to extend the accuracy of the bedside physical examination and allowing more rapid assessment of cardiovascular anatomy, physiology, and function.
Limited comparative studies with small numbers have indicated that these devices are more accurate than physical examination1 and, although their diagnostic performance is generally inferior to standard echocardiography, there appears to be close agreement between the two types of device.2–7,16,17 Previous comparative studies have been carried out by cardiologists with experience in echocardiography (levels II or III) and following the indications of the American Society of Echocardiography guidelines.8,18 Competence at the second level denotes sufficient experience to interpret images from the echocardiographic examination accurately and independently.8
Hand held devices seem suitable for evaluating cardiac morphology and function,2,5,6 left ventricular hypertrophy,3 and even for screening aortic aneurysms.4 However, signs of pulmonary hypertension, inflow or outflow obstruction, and diastolic dysfunction may be missed owing to the lack of spectral Doppler facilities.19,20
Recently, spectral Doppler technology has been incorporated into hand held devices in order to overcome this limitation, but up to now there has been no published information on this new technology. Our study showed an excellent correlation between pulsed and continuous wave Doppler measurements made with the hand held device and with a standard echocardiographic platform. This should lead to an improvement in cardiac evaluation, in particular the assessment of valve function and diastolic function.
Evaluation of diastolic function
Diastolic dysfunction of the left ventricle appears to be the earliest manifestation of myocardial ischaemia,21 and is a principal cause of congestive heart failure with preserved systolic function, accounting for up to 40% of incident cases.22 Doppler echocardiography is one of the most useful clinical tools for assessing left ventricular diastolic function and should be part of the routine echocardiographic evaluation of patients suspected of having heart failure. Doppler indices of left ventricular filling are easy to obtain and provide immediate information about diastolic function.
Standard platforms are additionally equipped with colour M mode and tissue Doppler to provide an accurate evaluation of diastolic function. These new Doppler applications have been shown to provide an accurate estimate of left ventricular relaxation and appear to be relatively insensitive to the effects of preload compensation.
Hand held devices are designed so that an echocardiographic examination can easily be undertaken at the time the patient is evaluated. Doppler evaluation of diastolic function with a hand held device using inflow tract velocities will add valuable screening information that can later be checked using standard echocardiography.
Evaluation of aortic outflow obstruction
The lack of spectral Doppler in hand held devices was an important limitation for complete valve evaluation. Previously, valve studies with hand held devices were limited to morphological assessment and to the subjective evaluation of valve regurgitation by colour Doppler. Despite limitations, valve regurgitation was accurately detected with first generation hand held devices.2 The new Doppler capabilities will allow complete valve evaluation including valve stenosis.
Doppler measurements are easily transformed to haemodynamic information using the Bernoulli equation. This formula is very accurate in estimating the pressure gradient across a restrictive orifice under most physiological conditions,23–25 and when tricuspid regurgitation is present application of the equation to the peak tricuspid regurgitation velocity provides a close estimate of the peak pressure gradient between the right ventricle and the right atrium.10 In contrast, in the absence of a restricted orifice26 the simplified Bernoulli equation is inaccurate for assessing intracardiac pressure gradients. In our study, although most patients did not have valve stenosis and although the use of peak gradient alone is not accurate enough to detect aortic stenosis, diagnostic agreement between the two echocardiographic devices reached 96% and in only four patients was the degree of stenosis misdiagnosed, corresponding always to one grade less in severity. As shown in fig 2, the maximum possible disagreement is 60 cm/s, which will result in no more than a one grade difference in estimating the degree of severity.
Evaluation of pulmonary hypertension
The determination of pulmonary artery pressures and right ventricular function is a critical part of the echocardiographic examination. The main limitation of echocardiography in evaluating pulmonary pressures is poor image quality and low Doppler signal strength. Moreover, the absence of a recordable tricuspid regurgitant jet does not indicate normal pulmonary pressures. In our study we found a good agreement in the evaluation of pulmonary pressures; however, significant differences in the number of patients in whom tricuspid regurgitation was detected led to misdiagnosis in an important number of patients.
Conclusions
Our results support the diagnostic value of a spectral Doppler facility built into hand held echocardiographic devices when they are used by cardiologists with experience in echocardiography. In such devices, Doppler can provide accurate measurements, comparable with these of standard platforms, overcoming the limitations encountered in previous studies. Thus, the new Doppler capabilities of hand held devices may lead to the more widespread use of echocardiography in clinical practice. However, a major limitation of these devices is the important number of patients with pulmonary hypertension who are missed when pulmonary artery pressures are determined.
Further studies are required to clarify the role of this new technology and the competence level required to undertake studies with the hand held device.
Acknowledgments
We are grateful to the research unit of the Gregorio Marañón General Hospital and, in particular to JM Bellón, for expert statistical advice. We would also like to thank Professor JC Kaski and Dr D Roy for useful comments and constructive criticism.