Article Text

Abstract
Objective: To study the diagnostic contribution of repeated transthoracic (TTE) and transoesophageal echocardiography (TOE) among patients with suspected infective endocarditis.
Methods: 262 patients with 266 episodes of suspected infective endocarditis were referred for TTE and TOE over three years in a 423 bed university cardiology hospital. Patients were a mean (SD) of 47.6 (17.9) years old. 139 (52.3%) episodes occurred in men and 127 (47.7%) in women. The diagnostic information obtained from repeated TTE and TOE examinations was evaluated relative to the diagnosis of endocarditis.
Results: TTE examinations were repeated in 192 (72.2%) and TOE examinations were repeated in 49 (18.4%) of 266 episodes. A mean of 2.4 TTE and 1.2 TOE examinations were performed for each episode of suspected endocarditis. The second and third TTEs added diagnostic information in 34 (26.7%) and the second and third TOEs added diagnostic information in 25 (19.7%) of 127 episodes with definite endocarditis. After the third TTE or TOE no additional diagnostic information was obtained.
Conclusions: The diagnostic contribution of repeated TTE or TOE for the diagnosis of endocarditis decreased as the number of repetitions increased. In this setting, the data do not substantiate more than three TTE or TOE examinations as an efficient strategy to increase the diagnostic yield for all but selected patients with suspected endocarditis.
- endocarditis
- echocardiography
- diagnosis
Statistics from Altmetric.com
Echocardiography is a valuable tool in the diagnostic evaluation of patients with suspected infective endocarditis.1–5 Patients with different pre-test probabilities of infective endocarditis are referred to echocardiography laboratories for evaluation.6–8 Repeated echocardiographic examinations were recommended for patients with high clinical suspicion of endocarditis and initial non-diagnostic echocardiographic findings.5 In clinical practice, repeated echocardiographic examinations are more common in clinical settings associated with greater diagnostic challenge, such as patients with cardiac valve prostheses, mainly soon after cardiac surgery,9,10 for patients with cardiac pacing devices,11,12 and for patients with acute disease before the results of blood cultures are available or when blood cultures are negative.13,14 Medical care of these patients evolved and the concept of the overuse of transthoracic echocardiography (TTE),15 mainly for patients with suspected endocarditis in native valves,16 has recently been introduced in the medical literature. Thus, the repetition of echocardiography deserves further studies in a variety of clinical settings.
The aim of this study was to evaluate the frequency and the diagnostic yield of repeated TTE and transoesophageal echocardiograms (TOE) among selected patients with suspected infective endocarditis referred for echocardiographic evaluation in a referral university hospital devoted to cardiological care including cardiac surgery.
METHODS
Study protocol
A prospectively cohort of 262 patients with 266 episodes of suspected infective endocarditis was studied. Patients were referred from April 1996 through August 1999 to the echocardiography laboratory of a tertiary 423 bed university cardiology hospital that performs about 400 cardiac operations monthly.
Patients were referred for echocardiographic evaluation by the physician in charge, following previously published criteria.4,5 The timing of the repeated examination was set by the physician in charge of the patient’s care. Blood cultures were often not available by the time the first echocardiograms were recorded.
During the period of the study, all patients with suspected infective endocarditis were submitted to a first TTE, as well as to a first TOE. Subsequent TTE examinations were performed whenever the previous study had not provided diagnostic findings. Subsequent TOE studies were performed whenever previous TOE examinations had not yielded diagnostic findings.
The first TTE and TOE studies were performed within five days of hospital admission. In 192 of the 266 (72.2%) episodes the examinations were done within 72 hours after hospital admission.
Patient characteristics
Table 1 presents the clinical and laboratory characteristics of the patients.
Clinical characteristics of 262 patients with 266 episodes of suspected infective endocarditis
Endocarditis was diagnosed according to Duke’s criteria.4 The diagnosis of endocarditis was classified as definite in 127 (47.8%) episodes, 112 (88.2%) of which were classified by clinical criteria and 15 (11.8%) by pathological criteria (table 1). Seventy six (29%) of the 262 patients were examined in the first 10 postoperative days.
Infective endocarditis occurred on prosthetic mitral valves in 46 (36.2%) episodes, on prosthetic aortic valves in 33 (26%), on the prosthetic pulmonary valve in 1 (0.8%), on native mitral valves in 25 (19.7%), on native aortic valves in 14 (11%), on native tricuspid valves in 2 (1.6%), on a native pulmonary valve in one (0.8%), on artificial cardiac pacemakers in 3 (2.4%), and on ventricular endocardium in 2 (1.6%).
Streptococci were isolated in blood cultures of 26 (20.5%) of the 127 patients with definite endocarditis (viridans group streptococci in 20), coagulase negative staphylococci in 26 (20.5%), Staphylococcus aureus in 21 (16.5%), Gram negative bacteria in 10 (7.8%), enterococci in 5 (3.9%), a combination of two microorganisms in 3 (2.4%), and fungi in 3 (2.4%) patients. In 33 (26%) patients, blood cultures were negative.
Echocardiographic techniques
TTE examinations were done by two dimensional imaging and by spectral and colour flow mapping with a 2.75 MHz transducer or a 2–4 or 3–5 MHz phased array transducer as previously described,17 with an Apogee CX 200 ultrasound system (Interspec, Inc, Ambler, Pennsylvania, USA), and with an HDI 3000 or HDI 5000 device (Advanced Technology Laboratories, Bothell, Washington, USA).
TOE examination followed local pharyngeal anaesthesia with 1% lidocaine spray. Intravenous midazolam was titrated from 0.5–5 mg according to the patients’ needs at the physicians’ discretion. Patients fasted for at least four hours before the examination. TOE examinations were carried out with patients in the lateral decubitus position and with two dimensional imaging and spectral and colour flow mapping as previously described.18 TOEs were recorded with a 5 MHz multiplane transducer (Apogee CX 200 ultrasound system) or a 5 MHz multiplane phased array transducer (model HDI 3000 or HDI 5000). Routine prophylactic antibiotics were not administered.
Images were recorded on VHS videotape and were evaluated by two physicians. The examiner was not blinded to clinical events and to echocardiographic findings from the previous examination. The tapes were reviewed later by one of the authors (MLCV) blinded to clinical events and to previous echocardiographic findings. In the event of disagreement between the two observers, the final echocardiographic diagnosis was made by a third observer not blinded to clinical events or to previous echocardiographic findings. We followed previously published criteria for the echocardiographic diagnosis of vegetations,1,19,20 valvar abscesses,21,22 and prosthetic valve dehiscence.23,24
The interobserver agreement for the diagnosis of vegetations, abscess, and prosthetic dehiscence was > 98%. The quality of the 330 TTE images recorded before the TOE examinations was defined relative to myocardial and valvar imaging identification as: (1) adequate in 256 (77.6%) examinations—when the myocardium and all four cardiac valves were well visualised; (2) regular in 52 (15.7%) examinations—when myocardium and at least three cardiac valves were well visualised; and (3) inadequate in 22 (6.7%) examinations—when the myocardium was not well visualised or only two cardiac valves were well visualised.
The variables we studied were the repetition of TTE and TOE examinations and the diagnosis of infective endocarditis, relative to the patients’ age, sex, and underlying cardiac conditions, the infecting microorganism, procedures associated with bacteraemia, and previous antimicrobial administration.
Statistical analysis
The associations between the repetition of the TTE and TOE studies and the demographic and laboratory data were analysed by the χ2 test or Fisher’s exact test. A probability value of p < 0.05 was considered significant.
Ethics
The study was approved by the hospital’s ethics committee on human research.
RESULTS
In 127 episodes with a definite diagnosis of infective endocarditis, 363 TTE (2.8 per episode) and 183 TOE (1.4 per episode) studies were performed. In 81 episodes with a possible diagnosis of infective endocarditis, 170 TTE (2.1 per episode) and 87 TOE (1.1 per episode) studies were performed (table 2). In 58 episodes with a rejected diagnosis of infective endocarditis, 96 TTE (1.6 per episode) and 60 TOE (1 per episode) examinations were made. Figure 1 is a flow chart of the sequence of echocardiographic examinations relative to diagnostic information. Table 3 presents the intervals between sequential echocardiographic examinations.
Diagnostic category change (Duke’s criteria) in 262 patients with 266 episodes of suspected infective endocarditis who underwent repeated transthoracic or transoesophageal examinations
Time interval in days between repeated TTE and repeated TOE in 262 patients with 266 suspected episodes of infective endocarditis
{kind=link}
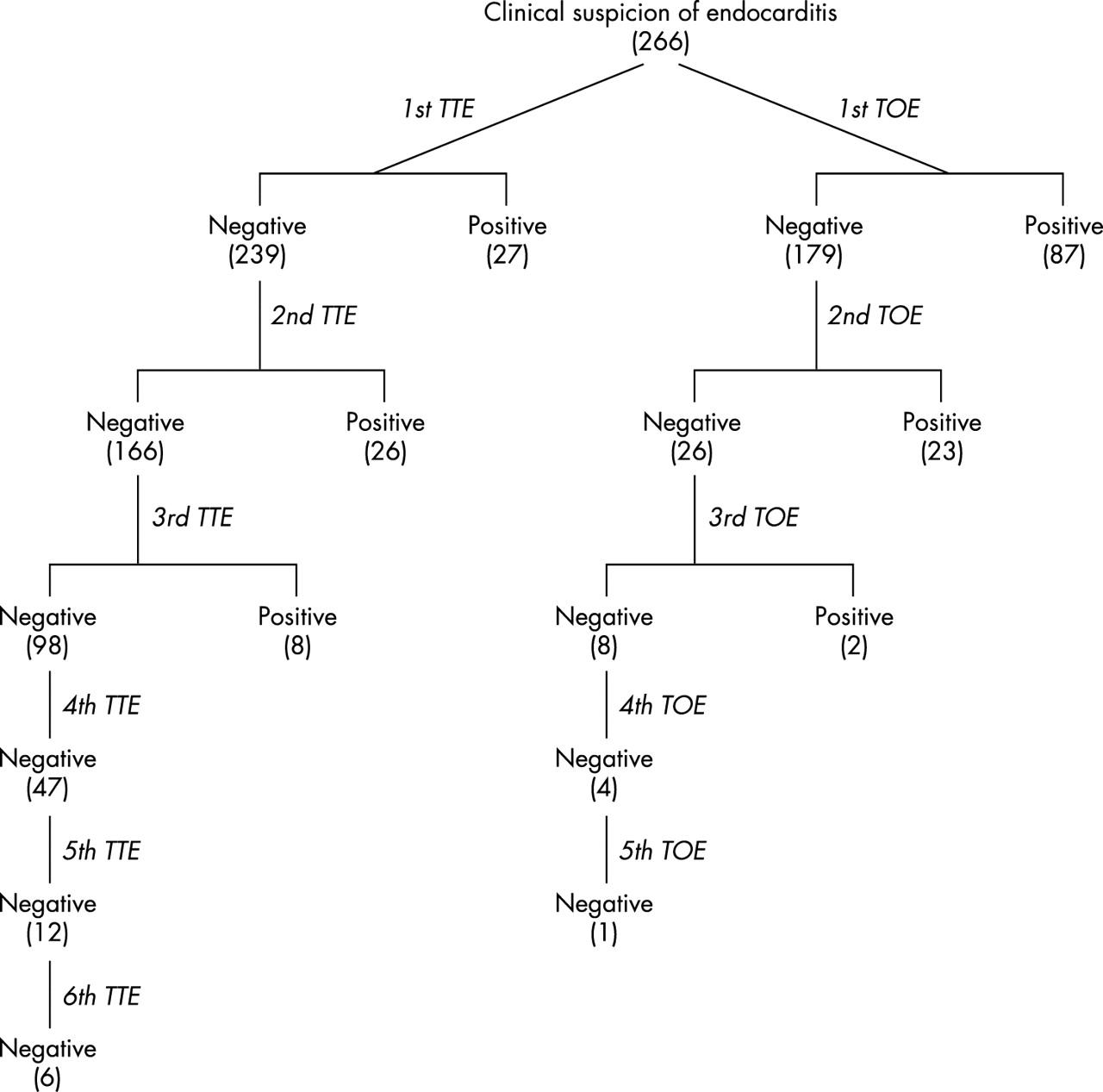
Transthoracic (TTE) and transoesophageal echocardiographic (TOE) investigation relative to positive and negative diagnostic findings in 262 patients with 266 episodes of suspected infective endocarditis. The numbers in parenthesis refer to the number of episodes with clinical suspicion of infective endocarditis.
Diagnostic findings after repeated TTE examinations
The first TTE was diagnostic in 27 (15 patients with native valve endocarditis and 12 with prosthetic valve endocarditis) of the 127 (21.2%) episodes in patients with a definite diagnosis of infective endocarditis and non-diagnostic in 100 episodes (24 patients with native valve endocarditis, 68 with prosthetic valve endocarditis, 5 with congenital heart disease, 3 with cardiac pacemaker). The findings of the first examination were vegetations in 21 patients, valvar abscesses in two, and prosthetic dehiscence in two.
The second TTE added diagnostic information in 26 (13.5%) of 192 patients who repeated the study once. The findings after the second examination were vegetations in 26 patients and valvar abscesses in three. The third TTE added diagnostic findings in eight (7.5%) of 106 patients who underwent TTE investigation three times. The findings after the third examination were vegetations in all eight patients.
After the third TTE, no additional diagnostic information was obtained. In 51 episodes with non-diagnostic findings on TTE, the quality of the image was considered adequate in 41 (80.4%) episodes, regular in seven (13.7%), and inadequate in three (5.9%) episodes.
Thus, after repeated examinations, the TTE findings were considered diagnostic in 61 (48.03%) of the 127 episodes with definite diagnosis of endocarditis.
Diagnostic findings after repeated TOE examinations
The first TOE was diagnostic in 87 (64 patients with prosthetic valve endocarditis, 22 with native valve endocarditis, and 1 with artificial cardiac pacemaker) of the 127 (68.5%) episodes in patients with definite diagnosis of infective endocarditis and non-diagnostic in 40 episodes (17 patients with native valve endocarditis, 16 with prosthetic valve endocarditis, 5 with congenital heart disease, and 2 with artificial cardiac pacemaker). The findings on the first TOE were vegetations in 87 patients, valvar abscesses in 20, and prosthetic dehiscence in 6.
The second TOE added diagnostic findings in 23 (46.9%) of 49 patients who repeated the study once. The findings on the second TOE were vegetations in 23 patients and valvar abscesses in 17. The third TOE added diagnostic findings in two (20%) of 10 patients who underwent the study three times; the findings after the third examination were vegetations.
After the third TOE, no additional diagnostic information was obtained.
Thus, after repeated examinations, the TOE findings were considered diagnostic in 112 (88.2%) of the 127 episodes with definite diagnosis of endocarditis.
Repeated TOE examinations and diagnostic reclassification
Repeated TOE examinations led to diagnostic reassignment from the category possible endocarditis to the category definite endocarditis in 51 (40.1%) of 127 patients with definite endocarditis diagnosis.
These 51 patients comprised 34 (42.5%) of 80 patients with prosthetic valve endocarditis (31 with bioprostheses and three with mechanical prostheses), 14 (35.9%) of 39 patients with native valve endocarditis, and all 3 (100%) patients with artificial cardiac pacemaker infections. In these episodes, the size of the vegetations were < 5 mm in 11 episodes, between 6–10 mm in 34 episodes, and larger than 10 mm in 6 episodes. In these 51 episodes with diagnostic reclassification, the imaging quality of the TTEs was considered adequate in 41 (80.4%) cases. Table 2 shows the changes in diagnostic category after each repeated echocardiographic examination.
There was no significant association between diagnostic findings on repeated echocardiographic TTE or TOE examinations leading to diagnostic category reassignment relative to the patients’ age, sex, and underlying cardiac conditions, the infecting microorganism, procedures associated with bacteraemia, and previous antimicrobial administration.
DISCUSSION
The present series includes a significant proportion of patients among whom the diagnosis of endocarditis may be challenging such as patients with prosthetic heart valves (55.3%), patients in the early postoperative period (29%), and a high rate of negative blood culture endocarditis (26%). Moreover, patients with different pre-test probabilities of the disease were enrolled in this study as shown by the diagnosis later established. There was a high proportion of prosthetic valve endocarditis (63%) and of patients submitted to surgical treatment (73.2%), which characterise a group of patients with severe disease and a high rate of anatomical evidence of lesions. These patients provided an interesting setting for the evaluation of diagnostic accuracy of repeated echocardiographic examinations.
The mean frequency of TTE examinations in each episode ranged from 1.6 among patients with a rejected diagnosis of endocarditis to 2.8 among patients with a definite diagnosis. The mean rate of TOE examinations in each episode ranged from one among patients with rejected endocarditis to 1.4 among patients with a definite diagnosis. The gradual increase in the mean frequency of examinations for rejected, possible, and definite endocarditis shows that physicians took into consideration the pre-test probability of the disease when ordering repeated examinations. Some patients were underwent several repeated TTE (n = 65) or TOE examinations (n = 5) despite previous non-diagnostic echocardiographic findings. We hypothesised that clinical conditions that were considered to suggest the diagnosis of endocarditis in the absence of an alternative explanation contributed to repeated examinations.
Repeated TTE and TOE up to the third examination added diagnostic findings. The diagnostic contribution of repeated TTE or TOE examinations for the diagnosis of endocarditis decreased as the number of repetitions increased. The repetition of TTE added more diagnostic findings than repeated TOE. Such an observation may be biased by the higher diagnostic yield of the first TOE.2,3,5 The second TTE or TOE provided additional diagnostic information but the third one added much less additional information, mainly with the transoesophageal approach. After the third TTE or TOE, no diagnostic category was reassigned. In this scenario, the present data do not corroborate the increase in the number of echocardiographic examinations as an efficient strategy to increase the diagnostic accuracy in all but a selected subset of patients with suspected endocarditis.
The literature about the optimal time interval for repetition of the examinations is scanty. Repeated TOE examinations has been recommended as a diagnostic strategy in suspected endocarditis, with a suggested time interval of 7–10 days for repeating echocardiograms.5 In our study, the time interval between the first and second examinations was in this range—a mean (SD) of 7.4 (5.2) days for TTE and 12.4 (6.6) days for TOE. The time interval was higher as the number of repetitions increased. Probably a lower diagnostic threshold hindered repeated examinations over time.
The findings of repeated TOE examinations contributed to change in 40.2% of the diagnoses (51 of 127 episodes), even though imaging quality of the TTE was considered adequate in 80.4% of these episodes. The diagnostic yield improved in all three patients with artificial cardiac pacemakers, in almost half of the patients with prosthetic valve endocarditis, and in a third of patients with native valve endocarditis, a trend comparable with that in other published reports.25 Our data suggest that repetition of echocardiographic examinations may benefit selected patients with suspected infective endocarditis even after a non-conclusive first examination—mainly those with cardiac prostheses and pacemakers.
The diagnostic category was more often reassigned after TOE study of patients with smaller vegetations, which was due to higher TOE accuracy to detect smaller structures.19 In this series, we observed vegetations < 5 mm in 11 (8.7%) of 127 episodes with a definite diagnosis. We wonder whether in the absence of the TOE examination this information would be missed. Specifically among patients with prosthetic valve endocarditis, the diagnosis for most patients was made after the first TOE examination. This finding would recommend the transoesophageal technique as the best first approach to patients with suspected prosthetic valve endocarditis, as previously suggested.5
Study limitations
This series is one of patients referred to a tertiary hospital and may not be representative of infective endocarditis in other clinical settings. For instance, we also included a significant proportion of early postoperative patients with a cardiac valve bioprosthesis. In addition, the intervals between the first echocardiographic examination and the following studies were heterogeneous. However, such an approach may shed some light on the frequency and yield of repetitions of echocardiographic examinations on clinical practice for patients with suspected endocarditis.
Clinical implications
Repeated echocardiographic examinations were common for patients with suspected endocarditis. The diagnostic contribution of repeated TTE or TOE examinations for the diagnosis of endocarditis decreased as the number of repetitions increased, mainly for patients with the lowest diagnostic probability of the disease. In this setting, our data do not substantiate more than three TTE or TOE examinations as an efficient strategy to increase the diagnostic accuracy in all but selected patients with suspected endocarditis. Our data may contribute to planning of echocardiographic evaluation of patients with infective endocarditis.
Acknowledgments
The authors thank Dr Cícero Piva de Albuquerque for critical review of the manuscript.