Article Text

Abstract
AIMS of AMIS Plus To learn from each other, to understand the transfer, use and practicability of knowledge gained from randomised trials and to generate input for subsequent prospective and randomised studies. Furthermore, to determine how adherence to guideline-based treatments in the ‘real world’ works.
Funding AMIS Plus is an industry-sponsored project but the supporting institutions do not play any part in the design of the registry, data collection, analysis or interpretation.
Quality-of-care interventions AMIS Plus data enable doctors to identify deficits in medical care, implement the necessary changes in diagnostics and therapeutic procedures and document their impact on clinical outcome in patients with acute coronary syndrome (ACS).
Setting From 106 hospitals treating ACS in Switzerland, 76 hospitals temporarily or continuously enrolled patients in AMIS Plus. Years: 1997–
Population Patients are included on the basis of their final diagnosis. Current number of cases: 33 040.
Start points ST elevation myocardial infarction, non-ST elevation myocardial infarction and since 2000, unstable angina.
Baseline data 230 variables are collected including demographics, medical history, cardiovascular risk factors, acute symptoms, time of symptom onset, first medical contact, time of admission and start of thrombolysis or balloon, out of hospital management, clinical presentation, early in-hospital management, reperfusion treatment, hospital course, diagnostic tests used or planned, hospital length of stay, discharge medication, destination and at 1 year, outcome, rehospitalisation, intervention, working time and quality of daily life.
Data capture Data are provided through an internet- or paper-based questionnaire completed by the treating doctor or a trained study nurse.
Data quality The data are centralised at the AMIS Plus Data Center, checked for plausibility and consistency and crosschecked when queries arise. Incomplete questionnaires are returned to the enrolment centres for completion. One-third of the variables are obligatory.
End point and linkages to other data In-hospital outcome, 3-months and 1-year follow-up outcome. No linkages exist at present.
Access to data Available for research with the approval of the AMIS Plus Steering Committee. Participating hospitals use the data for benchmarking and their own quality control.
- Acute coronary syndrome
- registry
- outcome
Statistics from Altmetric.com
Introduction
AMIS Plus is a large, prospective national registry that has been collecting data continuously for 13 years on the whole spectrum of patients with acute coronary syndrome (ACS) in Switzerland to assess the real world of care. The registry is endorsed by the Swiss Societies of Cardiology, Internal Medicine and Intensive Care and includes data from voluntarily participating hospitals of different sizes. The goals are to learn from each other and to understand the transfer, use and practicability of knowledge gained from randomised trials and to generate input for subsequent prospective and randomised studies. The registry documents presently 230 variables from over 33 000 patients which provide information on clinical characteristics as well as diagnostic and therapeutic procedures. Longitudinal AMIS Plus data enable doctors to identify deficits in medical care, implement the necessary changes in diagnostics and therapeutic procedures and to document their impact on clinical outcome in patients with ACS. The AMIS Plus registry allows a ‘real-world’ view of ACS management in Switzerland.
Background: reason for existence of database, when it began
In 1996, a group of doctors endorsed by the Swiss Societies of Cardiology, Internal Medicine and Intensive Care decided to collect data on patients with acute myocardial infarction (AMI) admitted to voluntarily participating Swiss hospitals. The AMIS (Acute Myocardial Infarction in Switzerland) registry started in January 1997 with the aims of describing the epidemiology of this clinical entity and potential changes, the quality of care with regard to diagnostic and therapeutic procedures, major adverse effects and in-hospital outcome. In 2000, unstable angina was included to further understanding of the care of these patients. The registry was thus renamed AMIS Plus. The year 2005 heralded the introduction of patient follow-ups 3 and 12 months after discharge as well as the documentation of coronary pathology in patients undergoing primary coronary reperfusion. Furthermore, it was decided to document overall mortality in subsequent years. The registry was approved by the Over-Regional Ethics Committee for Clinical Studies, the Swiss Board for Data Security and all cantonal Ethic Commissions.
Organisation
The registry is led by a steering committee (SC), which includes members of the three founding national societies. The SC directs the progress of the registry, regularly revises the questionnaire, decides what data are collected and sets the priorities for data analysis. It is responsible for the medical and financial aspects of the project, data use and announcing results.
The AMIS Plus project is an open-end national registry and comprises a national network between participating acute hospitals and the AMIS Plus Data Center housed by the Institute of Social and Preventive Medicine of the University of Zürich under the supervision of the SC.
The data are owned by the investigators of the AMIS Plus registry. AMIS Plus is an industry-sponsored project but the supporting institutions do not play any part in the design of the registry, data collection, analysis or interpretation. Besides the current seven main sponsors, 14 further companies have contributed annual donations (see ‘Acknowledgements’).
Data description
All patients with suspected ACS should be considered for inclusion but their eligibility is based on the final diagnosis: AMI, defined by characteristic symptoms and/or ECG changes and raised biomarker levels (troponin according to hospital-specific assay cut-off point or total creatine kinase or creatine kinase-MB fraction at least twice the upper limit or normal), ACS with minimal necrosis (symptoms or ECG changes compatible with ACS and cardiac biomarker levels below the cut-off point for MI) and unstable angina (symptoms or ECG changes compatible with ACS without raised levels of cardiac biomarkers). Patients were also categorised as having ST elevation acute coronary syndrome (STE-ACS) or non-STE-ACS (NSTE-ACS) based on initial ECG findings. Classification of STE-ACS included evidence of ACS as described above and ST-segment elevation and/or presumed new left bundle branch block on the initial ECG. NSTE-ACS included patients with ischaemic symptoms, ST-segment depression or T-wave abnormalities in the absence of ST elevation on the initial ECG.
Participating centres are strongly encouraged to enrol all patients fulfilling the inclusion criteria to avoid selection bias. However, the AMIS project began 1997 solely as a register of AMI and in 2000 it was expanded to include unstable angina (UA), thus in the registry NSTEMI/UA is under-reported.
Data collection and evaluation are carried out using the most up-to-date information technology. Participating hospitals ranging from regional to large tertiary centres provide data on patients with ACS to the AMIS Plus Data Center through an internet- or paper-based questionnaire (available at http://www.amis-plus.ch under Documents) completed by the treating doctor or a trained study nurse. From 106 hospitals treating ACS in Switzerland, 76 hospitals temporarily or continuously enrolled patients in AMIS Plus. According to the Swiss Federal Statistic Office, participating and non-participating hospitals did not differ significantly in size, available skills or quality grading.
Data of 230 variables are collected on medical history, known cardiovascular risk factors, acute symptoms, time of symptom onset, first medical contact, time of admission and start of thrombolysis or balloon, out of hospital management, clinical presentation, early in-hospital management, reperfusion treatment, hospital course, diagnostic tests used or planned, hospital length of stay, discharge medication and destination.
Since 2005, a subset of 53 hospitals has collected follow-up information after discharge for around 50% of the available patients. All patients who provided written informed consent are followed-up 3 months and 12 months after the initial hospitalisation. The follow-up includes a personal telephone interview carried out by the AMIS Plus Data Center team. Up to the present more than 5000 patients have been interviewed. The follow-up questionnaire includes data on survival, rehospitalisation for cardiovascular disease, reinfarction, permanent pacemaker or defibrillator implantation, working time and quality of daily life. Out-of-hospital mortality is ascertained by a follow-up call. Furthermore, AMIS Plus intends to link the data with the official all-cause death records of the national mortality statistics provided by the Swiss Federal Statistic Office.
Data collection, over a long time period if possible, is of critical importance. In order to keep up with the constant advancements in diagnostic tools and therapeutic modalities and at the same time not lose participating centres by suddenly increasing the data collection burden, important steps and revisions are initially introduced voluntarily until a large majority are willing to provide these data. Once these changes have been accepted by the majority of hospitals, additional questions and data then become mandatory. Thus, it was an important step in 2000 to include patients with UA and also details of the anatomy of coronary arteries in patients who underwent primary coronary reperfusion and the use of drug-eluting stents on a voluntary basis. The current questionnaire was recently revised to include the precise dosage of a particular drug and not only the class of drugs.
Data quality (accuracy, validation, completeness)
The data are centralised at the AMIS Plus Data Center, checked for plausibility and consistency and crosschecked if queries arise. Incomplete questionnaires are returned to the enrolment centres for completion.
In 2003, 19% of questionnaires were returned to the enrolment centres for completion, in most cases owing to one implausible or incomplete variable. In December 2004, an independent doctor reviewed hospital case records on a random sample of 20 patients for internal validation, which demonstrated good agreement with the data obtained from questionnaires (κ scores >0.8 for baseline data and therapeutic interventions). Error rate was 0% for therapeutic interventions, 0–0.9% for baseline characteristics and 1.2% for time variables (eg, time of symptom onset, time of percutaneous coronary intervention).
Example of data
More than 33 000 patients with acute myocardial infarction and unstable angina enrolled from a total of 76 Swiss hospitals (listed in ‘Acknowledgements’) are now included in the AMIS Plus database.
Mortality
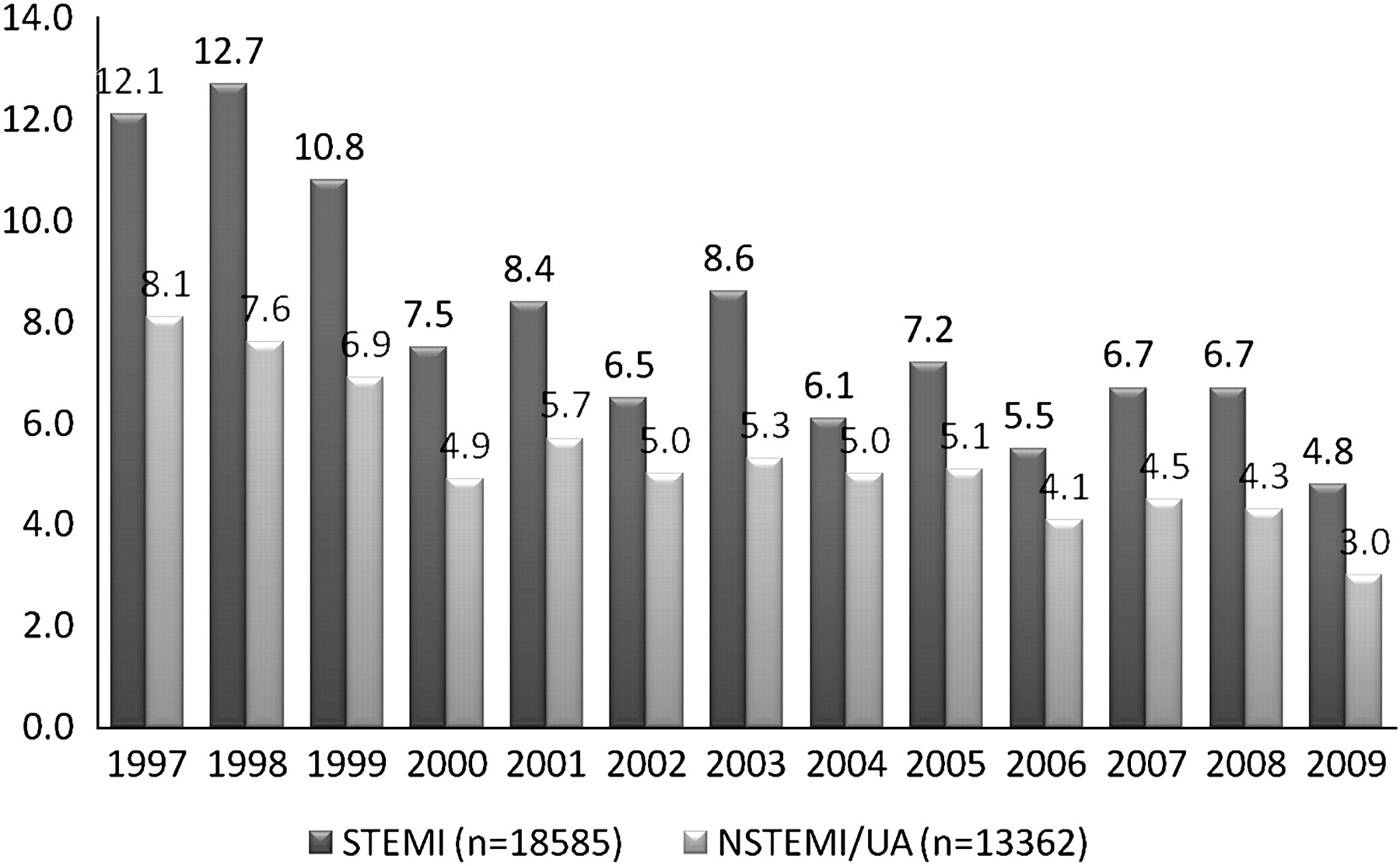
Crude in-hospital mortality decreased in patients with STEMI and in those with NSTEMI/AU (figure 1).

In-hospital mortality of patients with acute coronary syndrome. NSTEMI, non-ST-segment elevation myocardial infarction; STEMI, ST-segment elevation myocardial infarction; UA, unstable angina.
Reperfusion
Besides outcome assessment, the AMIS Plus registry also provides a real-world picture of ACS management in Switzerland and the opportunity to assess daily practice in a large population of ischaemic patients. In 2005, increasing trends in the use of reperfusion treatment were shown in Switzerland1 (figure 2).
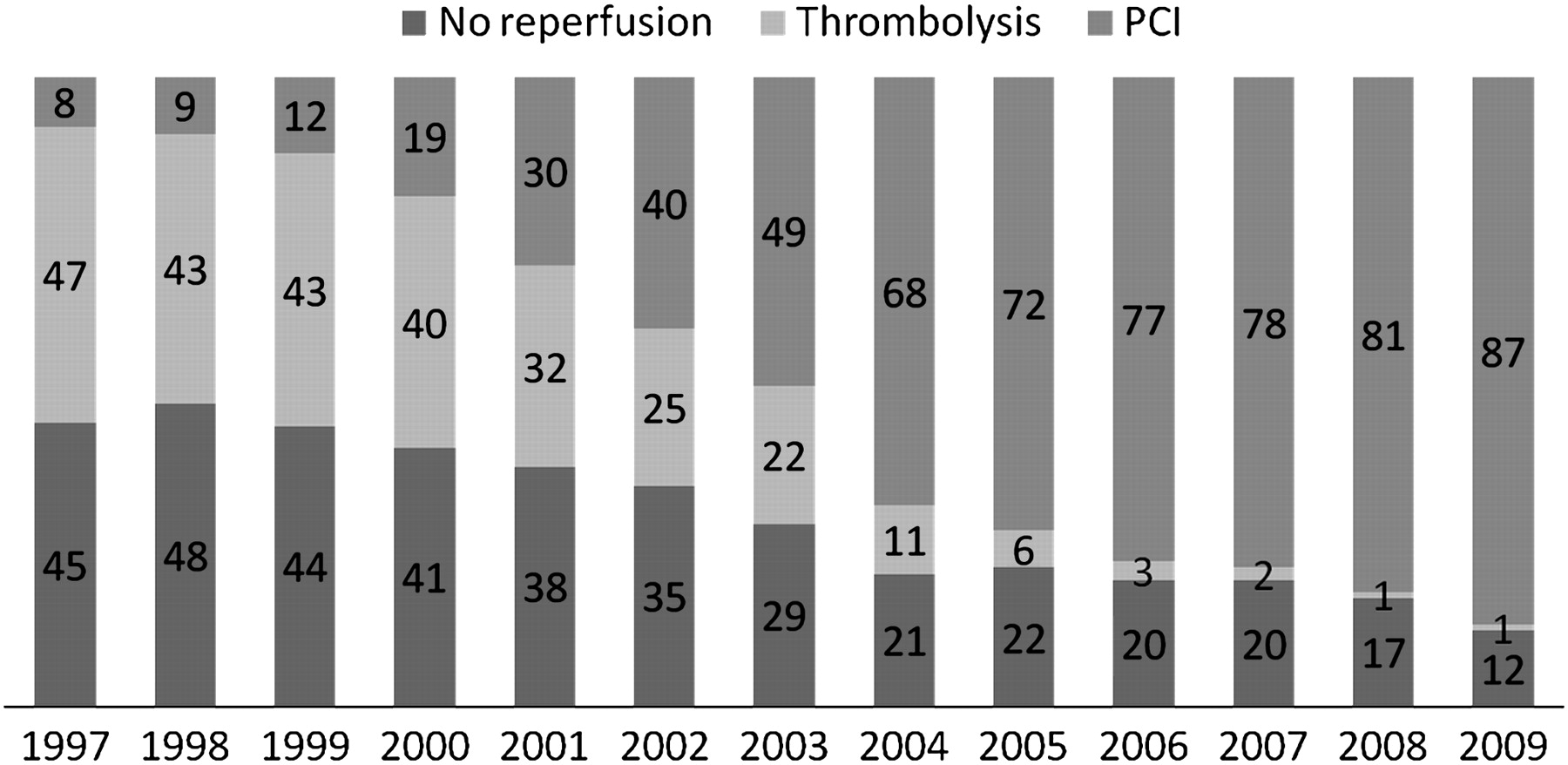
Reperfusion in patients with ST-segment elevation myocardial infarction (N=18 637).
Many studies examined the outcome of patients following coronary stenting comparing PCI with drug-eluting stents and bare-metal stents. AMIS Plus results of crude in-hospital-, 3-month and 1-year mortality according to the type of stent are depicted in table 1.
AMIS Plus results of crude in-hospital-, 3-month and 1-year mortality according to the type of stent
Although the OR adjusted for age, gender and comorbidities for 1-year mortality of patients receiving a drug-eluting stent was marginally significant (OR=0.48; 95% CI 0.23 to 0.99; p=0.049), the OR for the composite end point at 1 year including reinfarction and death was not significant (OR=0.72; 95% CI 0.38 to 1.38; p=0.324).
Delays
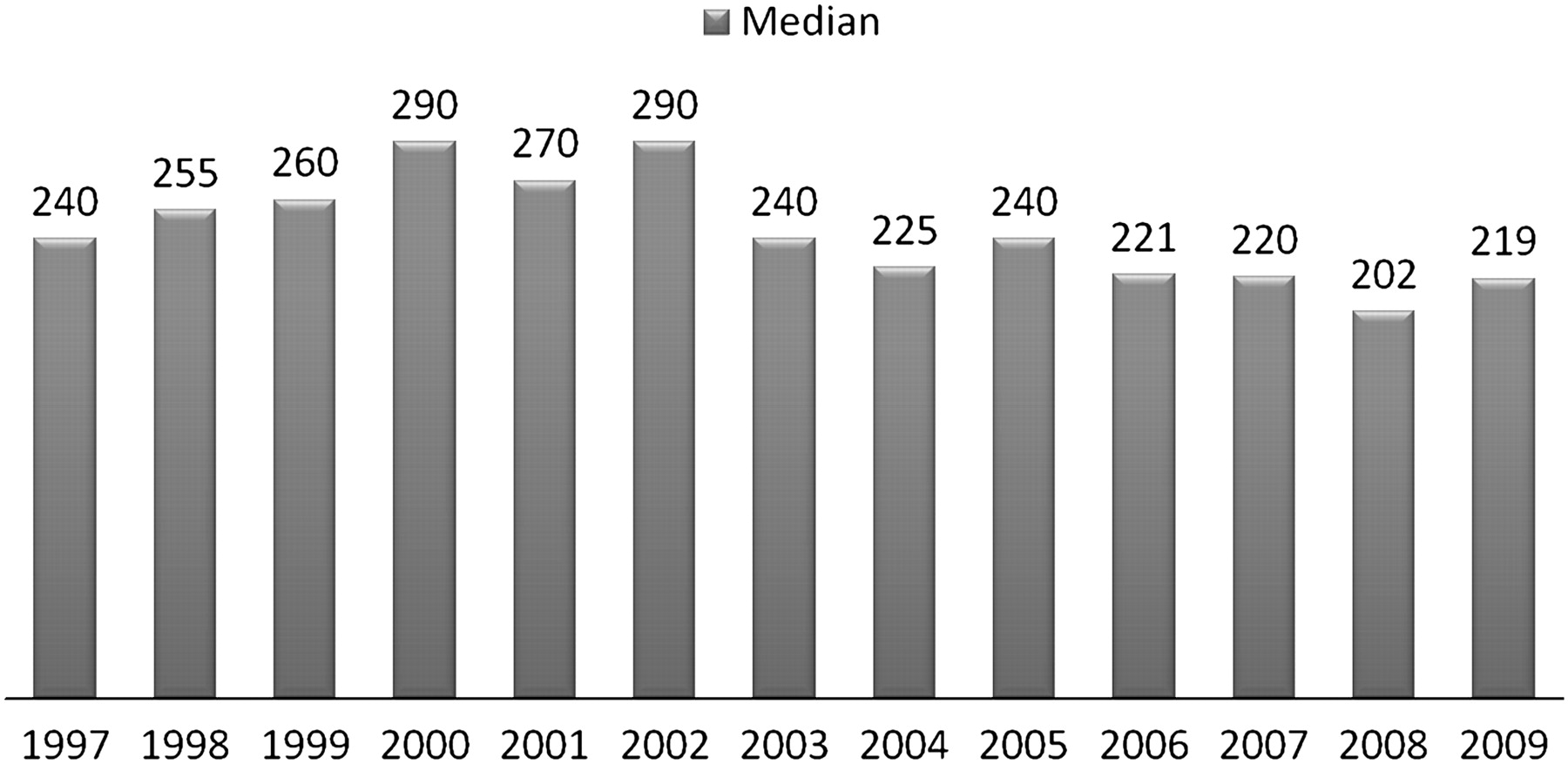
The AMIS Plus registry is not only an important instrument of cardiac care quality assessment as it can also indicate deficits. Although the in-hospital delay for PCI (door-to-balloon time) in patients with STEMI decreased in median from 118 min in 1999 to 48 min in 2009, overall pre-hospital delay (time between symptom onset and admission) of patients with ACS scarcely changed during the observed period (figure 3).

{kind=link}
{kind=link}
{kind=link}
Delay between symptom onset and admission of patients with acute coronary syndrome.
Use of the data
The data from the AMIS Plus registry enable characterisation of patients with AMI and UA, recording of examination and treatment strategies, compliance with guidelines and the optimisation of interventions, observation of changes over time as well as the economic consequences of treatment and the possible alternatives.
The implementation of the AMIS Plus project would not be possible without the highly motivated staff in charge of the patients with heart disease. Participating hospitals enter their data in the AMIS Plus registry and use these for benchmarking and their own quality control. AMIS Plus online analysis is carried out using the SPSS' real-time online statistics technology. This software allows the hospitals protected access to their current data at any time. For the purpose of benchmarking, ones own hospital patient data of 20 selected descriptive statistics can be compared with the anonymised data of all other hospitals or with the data of all other hospitals of the same size and category. The results are calculated online and are based on a weekly updated database (http://www.amis-plus.ch under Online Analysis, accessed April 2010). Online analysis is a benchmarking tool for participating hospitals enabling patient analysis to determine whether patients are treated according to evidence-based medicine and if the results of randomised prospective trials hold true in the world of clinical medicine.
Overview of the AMIS Plus publications
In the past decade clinical outcome of patients with AMI in Switzerland has improved and mortality decreased.2 Results of in-hospital outcomes of patients admitted with STEMI during working hours (from 07:00 to 19:00 on weekdays) compared with those admitted during out-of-hours (19:00 to 07:00 on weekdays or weekends) indicated no significant influence of time of admission on mortality and/or on the composite end point of reinfarction, stroke and death in AMIS Plus hospitals.3
It is important to assess whether all individual patients have access to the same quality of care and to evaluate if they profit to a similar extent from diagnostic and therapeutic procedures. Potential gender differences were analysed in baseline characteristics and also in management. In particular, PCI was performed less often in women than in men. Overall, in-hospital mortality was similar for women and men after adjustments but in women aged 51–60 years mortality remained slightly greater than that for men. The reasons for the significant underuse of PCI in women need to be further investigated together with the management and outcome of younger women who seem to be an unrecognised risk group.4
Furthermore, analysis showed that elderly patients across the whole spectrum of ACS were less likely to receive guideline-recommended medical and interventional treatments. An increasing underuse of acetylsalicylic acid, β blockers and percutaneous coronary interventions with increasing age was found even after allowing for contraindications and controlling for comorbidities. There may be important opportunities to improve outcomes of ACS care in the elderly; however, further research is needed to better understand this important domain of care to ascertain whether these observations were due to a larger burden of comorbidities, reduced incidence of informed consent to treatments or other factors.5
One of the AMIS Plus data analyses of 23 060 patients with ACS showed that over the past decade the rate of cardiogenic shock at admission of approximately 2% has remained more or less the same. However, cardiogenic shock developing during hospitalisation has significantly decreased among patients during this same period from 10.6% to 2.7%. Increased percutaneous coronary intervention rates were associated with decreased mortality among patients with cardiogenic shock and with decreased development of cardiogenic shock during hospitalisation.6
The AMIS Plus registry continuously provides important information on the use of medical treatments in adults with ACS in Switzerland. The majority of the patients (76.6%) with ACS in Switzerland enrolled in the AMIS Plus database received β-blocker treatment (either pretreated and continued or started during hospitalisation). If started after admission in haemodynamically stable patients, β blockers have the potential to markedly reduce in-hospital mortality and rates of major adverse cardiac events in patients with ACS. AMIS Plus data suggest that patients without reperfusion treatment or those undergoing thrombolysis benefit immensely from β-blocker treatment. Contrary to what would be expected, previous β-blocker treatment does not offer additional benefits over treatment started after admission and could even be potentially harmful leading to higher rates of cardiogenic shock.7 AMIS Plus findings provide additional evidence highlighting the importance of statin treatment in the treatment of ACS. Chronic statin treatment seems to alter the initial presentation of ACS but does not have an additional effect on early outcomes compared with statin treatment introduced after admission to statin-naive patients. High-risk populations, such as the elderly, diabetic subjects or patients with renal failure benefit even more.8
Registries provide the best method of documenting and following-up long-term changes in treatments and their implication on outcome in patients with ACS and also present the possibility of establishing the impact of changes in guidelines, measurements or definition, which could be very important for all players in cardiac care. Analyses from the AMIS Plus database showed that the new broadened definitions of MI to include patients with minimal elevation of serum troponin have led to a moderate increase in the incidence of MI in Switzerland. The inclusion of patients with similar baseline characteristics but smaller, less complicated acute events was associated with a better short-term prognosis despite less aggressive treatment. Although the long-term prognosis will need to be evaluated in a larger patient cohort, it would appear that the mid-term event rates at 3 and 12 months are similar for patients with ‘new MI’ and ‘classic MI’.9
The great number of enrolled patients in the AMIS Plus registry allowed the development and validation of a novel risk prediction model for ACS. The AMIS model reproducibly provides risk prediction of sufficient quality for daily clinical practice for patients with the entire spectrum of ACS at a very early stage of patient care, enabling optimisation of triage and management decisions before admission to hospital.10
Strengths and weaknesses of data
The weaknesses of the AMIS Plus are limitations common to all registries. Participation in the AMIS Plus registry is voluntary; the number of hospitals varied and might therefore not be entirely representative of all hospitals in the country despite the fact that permanently more than 60% of all hospitals with admission of patients with ACS participated. It could not be verified whether all consecutive patients with ACS were included by participating sites, or if selection biases occurred. Accordingly, the absolute number of patients enrolled in the AMIS Plus registry does not correspond to the national incidence of ACS leading to hospitalisation. Nevertheless, the AMIS Plus database is large for a small country such as Switzerland and represents hospitals of various sizes and equipment over a substantial period of time. The possibility of inaccuracies in data entry cannot be totally ruled out and may thus create unrecognised biases; although individual on-site auditing at the participating centres was performed sporadically but not systematically, data questionnaires were continuously and carefully checked by the data management centre. The limited resources of the AMIS Plus registry do not allow for systematic site visits and audits or very large questionnaires. Furthermore, as with all non-randomised data, we cannot exclude the possibility of selection bias, confounding by indication and residual confounding. All tracings were classified based on the assessment of the local investigators. There were no assessments of clinical eligibility for each drug and thus failure in the use of certain drugs may reflect contraindication for their use.
However, the major strength of AMIS Plus lies in the continuity of data collection, where the initial dataset has always remained the same. AMIS Plus regularly adapts the questionnaire to keep abreast of changes in international and national guidelines to allow permanent accurate determination of how cardiac care developments and improvements are mirrored in the real world in Switzerland. Continuity is of primary importance and allows unique studies assessing adherence to timely changes in guideline-recommended medical or interventional treatments and their impact on early, short- and mid-term outcomes. The introduction of new diagnostic and therapeutic modalities over the years was the reason for the revisions for data collection during the past years. AMIS Plus is the largest, ongoing registry of patients with ACS in Switzerland with a great number of enrolled patients.
Conclusions
AMIS Plus is a large, prospective national registry collecting data continuously for 13 years on the whole spectrum of patients with ACS in Switzerland. It can provide information on clinical characteristics, the treatment that patients actually receive and clinical evaluation. By following-up outcome data it is possible to document the implementation of new strategies and treatments in Switzerland and compare their value with the findings from randomised trials. Longitudinal AMIS Plus data enable doctors to identify deficits in medical care, implement the necessary changes in diagnostics and therapeutic procedures and to document its impact on clinical outcome in patients with ACS.
The AMIS Plus registry allows a real-world view of ACS management in Switzerland, providing the opportunity to assess daily practice in a large population of patients with ACS.
Acknowledgments
Present Steering Committee: P Erne, president, Lucerne; O Bertel, Zurich; F Eberli, Zurich; M Essig, Zweisimmen; F Gutzwiller, Zurich; P Hunziker, Basel; P-F Keller, Geneva; M Maggiorini, Zurich; G Pedrazzini, Lugano; D Radovanovic, Zurich, H Rickli, St Gallen; J-C Stauffer, Lausanne; P Urban, Geneva; S Windecker, Bern.
AMIS Plus Participants 1997–2009: The following hospitals participated in the AMIS registry (in alphabetical order): Aarau, Kantonsspital (P Lessing); Affoltern am Albis, Bezirkspital (F Hess); Altdorf, Kantonsspital (R Simon); Altstätten, Kantonales Spital (PJ Hangartner); Baden, Kantonsspital (U Hufschmid); Basel, Kantonsspital (P Hunziker); Basel, St. Claraspital (C Grädel); Bern, Beau-Site Klinik (A Schönfelder); Bern, Inselspital (S Windecker); Biel, Spitalzentrum (H Schläpfer); Brig-Glis, Oberwalliser Kreisspital (D Evéquoz); Bülach, Spital (A Vögele); Burgdorf, Regionalspital Emmental (D Ryser); Chur, Kreuzspital (R Jecker); Chur, Rätisches Kantons- und Regionalspital (P Müller); Davos, Spital (G Niedermaier); Dornach, Spital (A Droll / T Hongler); Einsiedeln, Regionalspital (S Stäuble); Flawil, Kantonales Spital (J Haarer); Frauenfeld, Kantonsspital (HP Schmid); Fribourg, Hôpital cantonal (B Quartenoud); Frutigen, Spital (K Bietenhard); Genève, Hôpitaux universitaires (HUG) (JM Gaspoz/ PF Keller); Glarus, Kantonsspital (W Wojtyna); Grenchen, Spital (B Oertli/R Schönenberger); Grosshöchstetten, Bezirksspital (C Simonin); Heiden, Kantonales Spital (R Waldburger); Herisau, Kantonales Spital (M Schmidli); Interlaken, Spital (EM Weiss); Jegenstorf, Spital (H Marty); La Chaux-de-Fonds, Hôpital (H Zender); Lachen, Regionalsspital (C Steffen); Langnau im Emmental, Regionalspital (A Hugi); Laufenburg, Gesundheitszentrum Fricktal (E Koltai); Lugano, Cardiocentro Ticino (G Pedrazzini); Luzern, Luzerner Kantonsspital (P Erne); Männedorf, Kreisspital (T Luterbacher); Martigny, Hôpital régional (B Jordan); Mendrisio, Ospedale regionale (A Pagnamenta); Meyrin, Hôpital de la Tour (P Urban); Monthey, Hôpital du Chablais (P Feraud); Montreux, Hôpital de Zone (E Beretta); Moutier, Hôpital du Jura bernois (C Stettler); Münsingen, Regionales Spital Zentrum (F Repond); Münsterlingen, Kantonsspital (F Widmer); Muri, Kreisspital für das Freiamt (H Lusser); Nyon, Group. Hosp. Ouest lémanique (R Polikar); Olten, Kantonsspital (S Bassetti); Rheinfelden, Gesundheitszentrum Fricktal (HU Iselin); Rorschach, Kantonales Spital (M Giger); Samedan, Spital Oberengadin (P Egger); Sarnen, Kantonsspital Obwalden (T Kaeslin); Schaffhausen, Kantonsspital (R Frey); Schlieren, Spital Limmattal (T Herren); Schwyz, Spital (P Eichhorn); Scuol, Ospidal d'Engiadina Bassa (C Neumeier); Solothurn, Bürgerspital Solothurn (A Grêt/R Schöneneberger); St. Gallen, Kantonsspital (H Rickli); Sursee, Luzerner Kantonsspital (S Yoon); Thun, Spital (U Stoller); Thusis, Krankenhaus (UP Veragut); Tiefenau, Tiefenauspital (P Loretan); Uster, Spital (E Bächli); Uznach, Kantonales Spital (A Weber); Wädenswil, Schwerpunktspital Zimmerberg-Horgen (B Federspiel/M Weisskopf); Walenstadt, Kantonales Spital (D Schmidt/J Hellermann); Wetzikon, GZO Spital (M Graber); Winterthur, Kantonsspital (A Haller); Wolhlusen, Luzerner Kantonsspital (M Peter); Zofingen, Spital (S Gasser); Zollikerberg, Spital (P Siegrist / R Fatio); Zug, Kantonsspital (M Vogt/D Ramsay); Zürich, Stadtspital Triemli (F Eberli); Zürich, Stadtspital Waid (S Christen); Zürich, Klinik im Park (O Bertel); Zürich, Universitätsspital Zürich (M Maggiorini).
Footnotes
Funding Sources 2009 Main sponsors Astra-Zeneca, Bayer-Schering, Biotronik, Daiichi-Sankyo/Lilly, Invatec, A. Menarini, Medtronic, St. Jude Medical, all in Switzerland. Donators: Abbott, Biosensors, Bristol-Myers Squibb, GlaxoSmithKline, Johnson & Johnson, Merck Sharp & Dohme-Chibret, Essex, Novartis, Pfizer, Sanofi-Aventis, Servier, SPSS and Takeda, all in Switzerland.
Competing interests None.
Ethics approval This study was conducted with the approval of the Over-Regional Ethics Committee for Clinical Studies, the Swiss Board for Data Security and all cantonal Ethic Commissions.
Provenance and peer review Commissioned; externally peer reviewed.