Article Text

Abstract
Context Surgical treatment of aortic root aneurysm in Marfan syndrome (MFS) patients.
Objective To compare results of total root replacement versus valve-sparing aortic root replacement in MFS patients.
Data Sources PubMed, Embase and Cochrane library were searched from January 1966 until February 2010 looking for papers reporting on aortic root operations in MFS patients. 530 studies were retrieved.
Study Selection Finally, 11 publications were enrolled. Inclusion criteria were observational studies reporting valve-related morbidity and mortality after total root replacement (TTR) and/or valve-sparing root replacement (VSRR) in patients with MFS and study size n≥30, reflecting the centre's experience.
Data Extraction Data obtained from papers reporting both TRR and VSRR cohorts were analysed separately. In case of multiple publications, the most recent and complete report was selected. If the total number of patient-years was not provided, we calculated it by multiplying the number of hospital survivors with the mean follow-up duration of that study.
Results Overall, 1385 patients were analysed (972 patients had TTR and 413 patients had VSRR). Reintervention rate was 0.3%/year (95% CI 0.1 to 0.5) versus 1.3%/year (95% CI 0.3 to 2.2) (p=0.02) and thromboembolic events rate was 0.7%/year (95% CI 0.5 to 0.9) versus 0.3%/year (95% CI 0.1 to 0.6) (p=0.01) after TRR and VSRR, respectively. When composite valve-related events were compared, no difference existed between the two surgical strategies (p=0.41). Among patients undergoing VSRR, reimplantation was associated with a reduced rate of reintervention compared with remodelling (0.7%/year vs 2.4%/year, p=0.02).
Conclusions VSRR may represent a valuable option for patients with MFS with aortic aneurysm. However, this technique should be used with caution in patients with valve characteristics at risk for decreased durability.
- Marfan
- aneurysm
- aorta
- valves
- surgery
- meta-analysis
- surgery-valve
- aortic valve disease
Statistics from Altmetric.com
A characteristic pathological dilatation of the aortic root—namely, annuloaortic ectasia, exists in about 75–85% of patients with Marfan syndrome (MFS).1 This includes dilatation of the aortic sinuses and annulus in addition to the ascending aorta, leading to aortic valve insufficiency. If left untreated there is a high risk of death due to dissection or rupture of the aorta or heart failure resulting from severe aortic regurgitation.2
Aortic root replacement has dramatically improved the survival of these patients.3
However, there is still no agreement about the best method of dealing with malfunction of the aortic valve caused by aneurysm of the aortic root in MFS.
Total aortic root replacement (TRR) using a composite mechanical valve conduit, a method introduced by Bentall and De Bono,4 has long been considered the ‘gold-standard’ treatment in this setting, providing excellent early and late postoperative outcomes. However, a significant proportion of patients receiving mechanical valve substitutes experience complications related to long-term anticoagulation.
Recently, valve-sparing aortic root replacement (VSRR) has emerged as an alternative to composite valve-graft aortic root replacement, particularly in patients with MFS who have isolated root pathology with functionally normal valve leaflets.5 6 This technique preserves native valves, thus avoiding the disadvantages of a mechanical prosthesis and the complication of lifelong anticoagulation.
However, aortic valve leaflets carry a structural fibrillin-1 defect and this aspect has created controversy about the durability of aortic valve reconstructions in patients with MFS.7 No randomised trial has ever examined this problem and reports on outcomes after VSRR in MFS are limited by small study size and results showing variable durability. Therefore, many surgeons continue to remain sceptical about aortic valve preservation in MFS because of fear of late valve failure.
Systematic reviews allow for a more objective appraisal of evidence than traditional narrative reviews and thus may contribute to resolving uncertainty when original research, reviews and editorials disagree. To gain insights into the role of valve-sparing procedures in patients with MFS we compared outcomes after TRR with those after VSRR, conducting a systematic review and meta-analysis on observational surgical cohorts.
Material and methods
This systematic review and meta-analysis were done with the use of the Meta-analysis Of Observational Studies in Epidemiology (MOOSE) guidelines.8
Search strategy
On 20 February 2010, a PubMed and Embase search of (aortic valve sparing OR aortic valve preserving) OR (Bentall OR aortic root replacement OR composite valve graft) OR (aortic root surgery) AND (Marfan) was conducted, limited to publications from January 1966 until February 2010 in humans. In addition, the entire Cochrane library was searched for (aortic valve replacement Marfan) OR (aortic valve sparing Marfan) OR (ascending aorta replacement Marfan) in the title, abstract, or key words of publications. One reviewer (EA) screened the titles and abstracts of identified studies. Inclusion criteria were observational studies reporting valve-related morbidity and mortality after TTR and/or VSRR in patients with MFS and study size n≥30, reflecting the centre's experience. A second independent reviewer (UB) assessed whether inclusion and exclusion were performed correctly. In cases of disagreement, an agreement was negotiated. References of selected articles were cross-checked for other relevant studies.
Data extraction
Microsoft Excel and Comprehensive Meta Analysis V2.0 (2006 Biostat, Inc) were used for data extraction and statistical analysis. The study design was documented. When this could not be done the study was excluded. Data obtained from papers reporting both TRR and VSRR cohorts were analysed separately. When multiple publications on the same patient population were found, the most recent and complete report was selected. Outcome events were defined as follows: reintervention on the aortic valve, thromboembolic event, endocarditis.9 If the total number of patient-years was not provided, we calculated it by multiplying the number of hospital survivors with the mean follow-up duration of that study.
Statistical analysis
Linearised occurrence rates of valve-related complications (reintervention on aortic valve, thromboembolic event and endocarditis) were calculated ((number of events/number of patient-years)×100) for each individual study and pooled on a logarithmic scale with the use of the inverse variance method in a fixed- or random-effects model according to heterogeneity. When an included study did not specify a particular valve-related event in the ‘Methods’ section, did not mention it in the ‘Results’ section, or omitted it from both sections, then the study was excluded from analysis of that event. Funnel plots were used to study publication bias. Heterogeneity was assessed with the use of the Cochran Q statistic and the I2 test. To compare TRR and VS results, a separate analysis of heterogeneity between the two groups was performed using the Cochrane Q statistic. Patient age, urgent indication and valve-sparing technique used (reimplantation vs remodelling) were explored as potential causes for heterogeneity through subgroup analyses. Heterogeneity related to different follow-up durations among studies was assessed by a meta-regression analysis (fixed-effect model). Publication bias was detected by Egger's regression test.
Results
A total of 530 studies were identified; studies were excluded for the following reasons: other subject (n=226), review or (invited) comment (n=66), case reports (n=82), no English language articles (n=24), no patients with MFS included (n=87); data on outcomes of interest not reported (n=10), fewer than 30 patients included (n=9), overlap with other studies (n=15). Eleven publications10–20 were included in the final analysis: two reported results after both TTR and VSRR,11 16 five reported result after TTR10 12–15 and four reported results after VSRR.17–20
Overall, 1385 patients were analysed (972 patients had TTR and 413 patients had VSRR). Mean follow-up time was 8.0 years for patients with a TRR and 4.7 years for patients with a VS (p=0.003) and the total number of patient-years was 935 and 344, respectively. Table 1 provides an overview of the publications obtained by the systematic review.
Overview of publications included in the analysis
Meta-analysis
Table 2 displays pooled valve-related complications after aortic root surgery by surgical procedures (TRR vs VSRR), including heterogeneity test results.
Pooled outcome estimates*
VSRR was associated with a fourfold increased rate of reintervention on aortic valve when compared with TRR (1.3%/year vs 0.3%, p=0.02). To control for potential heterogeneity caused by surgical technique adopted in the VSRR group on reintervention rate, a subgroup analysis pooling publications in which reimplantation techniques were preferred (more than 70% of patients) was performed. Interestingly, reimplantation was associated with a reduced rate of reintervention when compared with remodelling (0.7%/year vs 2.4%/year, p=0.02), although it was still inferior to TRR (p=0.02).
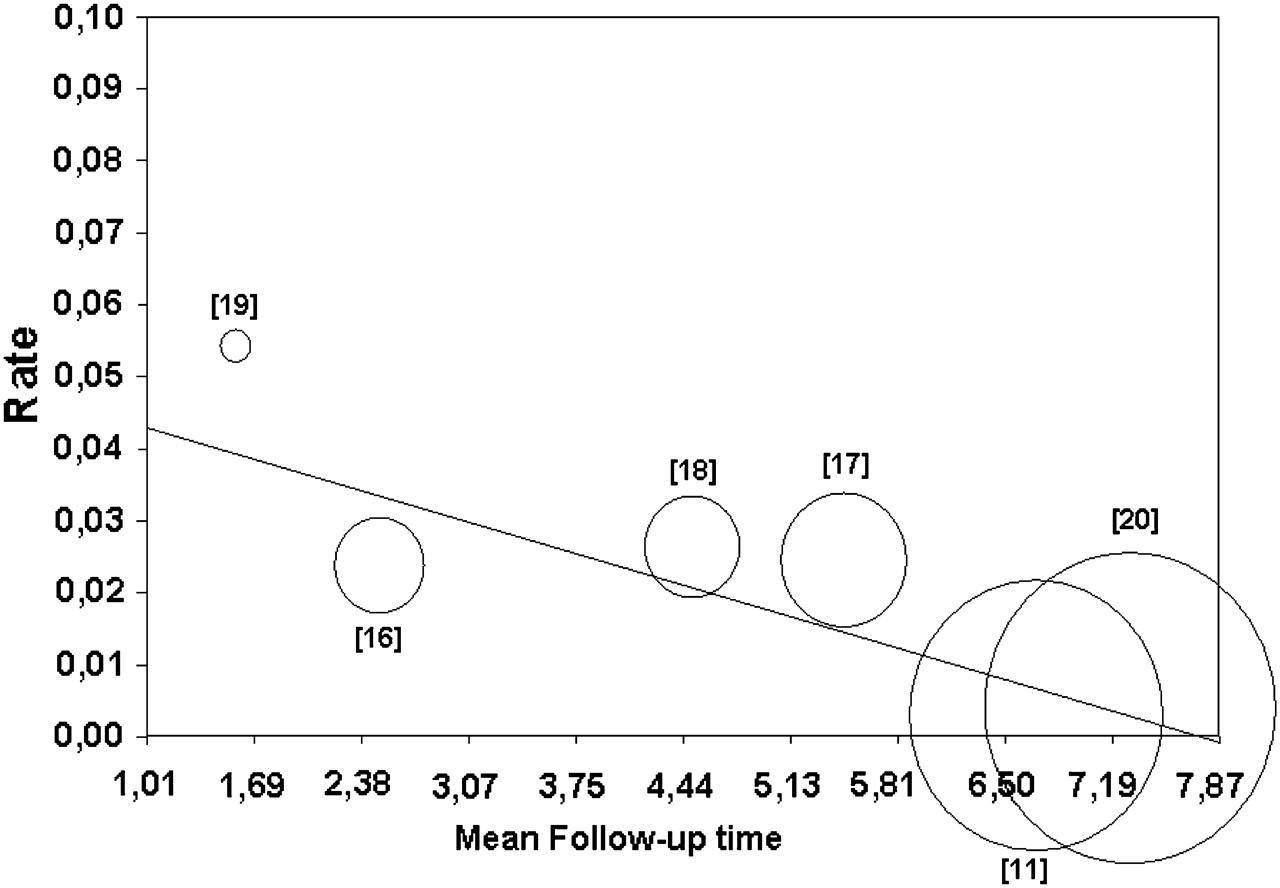
Potential heterogeneity caused by different follow-up durations among studies on reintervention rates after VSRR was investigated by a meta-regression, which showed an inverse relationship between reintervention rate and follow-up duration with the highest rates recorded in the small sample size and short follow-up studies (Q-model 11; p=0.008; figure 1).
{kind=link}
Meta-regression analysis for mean follow-up on reintervention rate (circles indicate individual trials with relative reference number. Radii are proportional to relative study weight. Q-model 11; p=0.008).
As expected, when compared with VSRR, TRR was associated with an increased rate of thromboembolic event (0.7%/year vs 0.3%/year; p=0.01) but no significant difference was observed for endocarditis rate (0.3%/year vs 0.2%/year; p=0.32). When composite valve-related event were compared, no difference existed between the two techniques (p=0.41).
Mean age at the time of operation and urgent indication did not influence valve-related complication rates.
Publication bias
Egger's test confirmed a tendency towards a higher reintervention rate in small sample size studies (p=0.001) meanwhile no publication bias was detected for thromboembolic event (p=0.19) and endocarditis (p=0.64).
Discussion
This meta-analysis, pooling a large number of patients with MFS from observational surgical cohorts, demonstrated that VSRR was associated with an increased risk of reintervention on aortic valve in comparison with TRR. However, this disadvantage become less evident when reimplantation was adopted as VSRR technique. As expected, thromboembolic events were more frequent after TRR with no significant difference in the occurrence of endocarditis. Interestingly, the overall incidence of all valve-related complications was comparable after TRR and VSRR, respectively.
Before the introduction of TRR, the prognosis of the patients with MFS was dismal.1 2 Successful employment of this technique4 is considered to have been the single most important factor responsible for the dramatic improvement in the prognosis of these patients.3
However, most patients with MFS are young at the time of operation and therefore they usually receive a mechanical prosthesis which exposes them to the risk of thromboembolic events endocarditis.11–17
VSRR has emerged as an alternative in patients who have little or no valve involvement to avoid the need for anticoagulation and late valve-related complications.5 6 The two main valve-sparing procedures proposed in MFS are reimplantation5 and remodelling.6 The principal advantage of the reimplantation technique is the stabilisation of the annulus, while remodelling is functionally superior because it preserves the function of aortic root. However, concerns exist about the late fate of preserved aortic valves in patients with MFS since they are structurally abnormal,7 and many surgeons continue to be reluctant to adopt valve-sparing techniques in this setting.15 What remains unknown is the truly long-term results in larger numbers of patients with the MFS and whether the overall incidence of all valve-related complications will be lower than that after conventional TTR with a mechanical prosthetic valve. There is an ongoing prospective, international registry study21 comparing VS with TTR but it lacks random allocation. To date it has only provided comparative data on short-term clinical outcomes.21 Therefore, until we can compare the two surgical strategies through a prospective randomised study, a meta-analysis continues to be probably one of the most reliable ways to provide objective information.
This study suggested that reimplantation should be considered a valuable surgical option for patients with MFS, being associated with an acceptable reintervention rate, although it was not comparable to that reported after TRR. Interestingly, overall occurrence of composite valve-related complications, including reintervention on aortic valve, thromboembolic event and endocarditis, was comparable after VSRR and TRR, respectively. Remodelling was associated with an unacceptable risk of reintervention, thus supporting the hypothesis that for patients with connective tissue disorders such as Marfan syndrome, it is particularly important to provide fixation of the aortic annulus, thus making it non-susceptible to future dilatation.
The findings of this meta-analysis must be interpreted with some caution. The design of the study lacks random allocation to TRR or VSRR, and no studies included in the meta-analysis reported the criteria considered by the individual surgeons to allocate patients to either group. A subtle bias towards VRSS in patients with smaller degrees of preoperative aortic regurgitation was probably active. This aspect might have underestimated the incidence of the reintervention rate after VSRR. Second, the two groups were not comparable for all the factors that can alter the outcome of interest, and the possibility of confounding factors cannot be excluded.
Mean follow-up was significantly shorter after valve sparing and it can be argued that reintervention rate might have been under-reported as a consequence. To deal with this issue we performed a meta-regression, which interestingly showed that the highest reintervention rates were recorded in the small sample size and short follow-up studies. This means that aortic valve failure occurs in an early phase after VSRR, thus suggesting an important role of technical errors or surgical complexity and reflecting the single centre and surgeon experience. In conclusion, VSRR may represent a valuable option for patients with MFS with aortic aneurysm. When valve sparing is considered, the reimplantation procedure that reliably prevents future dilatation of the aortic annulus is certainly the most prudent choice. However, this technique should be used with caution in patients with valve characteristics at risk for decreased durability. Finally, this surgery should be performed in centres with considerable experience in valve-sparing techniques because the initial learning curve can be flat.