Article Text

Abstract
Background Chronic thromboembolic pulmonary hypertension (CTEPH) is a complication of pulmonary embolism potentially curable by surgery. Perfusion scintigraphy is currently advocated as the imaging modality of choice to exclude CTEPH due to its high sensitivity. We have evaluated the diagnostic utility of lung perfusion MRI.
Methods Consecutive patients attending a pulmonary hypertension referral centre undergoing lung perfusion MRI, perfusion scintigraphy, CT pulmonary angiography (CTPA) and right heart catheterisation within 14 days were identified.
Results Of 132 patients, 78 were diagnosed as having CTEPH. Lung perfusion MRI correctly identified 76 patients as having CTEPH with an overall sensitivity of 97%, specificity 92%, positive predictive value 95% and negative predictive value 96% compared with perfusion scintigraphy (sensitivity 96%, specificity 90%) and CTPA (sensitivity 94%, specificity 98%). No cases of surgically accessible CTEPH were missed with either modality.
Conclusions Lung perfusion MRI has high sensitivity equivalent to perfusion scintigraphy in diagnosing CTEPH but does not require ionising radiation, making it an attractive initial imaging modality to assess patients with suspected CTEPH.
- Imaging/CT MRI etc
Statistics from Altmetric.com
Chronic thromboembolic pulmonary hypertension (CTEPH) occurs in up to 3.8% of patients following pulmonary thromboembolism (PTE) and is a major cause of severe pulmonary hypertension (PH). Patients usually present with breathlessness following PTE or with unexplained PH. The diagnosis may be missed on CT pulmonary angiography (CTPA) by radiologists not experienced in pulmonary vascular disease, so perfusion scintigraphy has been recommended as a screening test, given its high sensitivity. In recent years, MRI has evolved into a holistic imaging modality in PH, allowing morphological assessment of the pulmonary vasculature and structural and functional assessment of the heart.1 In addition, 3D contrast-enhanced lung perfusion MRI provides insight into regional pulmonary perfusion by tracking the dynamic passage of a contrast bolus. Previous studies have demonstrated the feasibility of this technique in acute PTE.2 However, there is limited data on the performance of 3D contrast-enhanced lung perfusion MRI in diagnosing CTEPH in a high-risk population.3 ,4
From a large PH referral centre, consecutive patients with suspected CTEPH or unexplained PH who had lung perfusion MRI, perfusion scintigraphy, CTPA and right heart catheterisation within 14 days were identified from the ASPIRE registry5 to compare the diagnostic utility of these imaging modalities. 3D MR lung perfusion images were acquired using a time resolved 3D spoiled gradient echo sequence with view sharing and were analysed by two radiologists blinded to the other imaging studies and clinical information. The final diagnosis of CTEPH was based on clinical assessment, right heart catheter and imaging, including MR angiographic studies (but not the MR perfusion images analysed in this study), CTPA and perfusion scintigraphy. The diagnosis of surgically accessible disease was confirmed at the national pulmonary endarterectomy centre at Papworth.
Of the 132 patients fulfilling the inclusion criteria, 78 had CTEPH. Forty-eight patients showed no evidence of CTEPH and included patients with a diagnosis of no PH (n=5), and all major forms of PH, including pulmonary arterial hypertension (n=18), PH associated with left heart disease (n=12), PH associated with lung disease (n=8) and PH multi-factorial (n=5). Six of the MR perfusion image data sets were of non-diagnostic quality. The MR perfusion images correctly identified 76 patients to have CTEPH giving it a sensitivity of 97% (95% CI 0.91% to 0.99%) and specificity of 92% (95% CI 0.80% to 0.97%) (table 1). The results also showed CTPA, interpreted by the expert pulmonary vascular radiologists, and perfusion scintigraphy to be effective in the diagnosis of CTEPH with a sensitivity of 94% (95% CI 0.85% to 0.98%) and 96% (95% CI 0.89% to 0.99%), respectively (figure 1). None of the imaging modalities missed any of the patients with surgically accessible disease.
Summary of diagnostic performance of perfusion scintigraphy, MR perfusion and CTPA in the diagnosis of CTEPH

{kind=link}
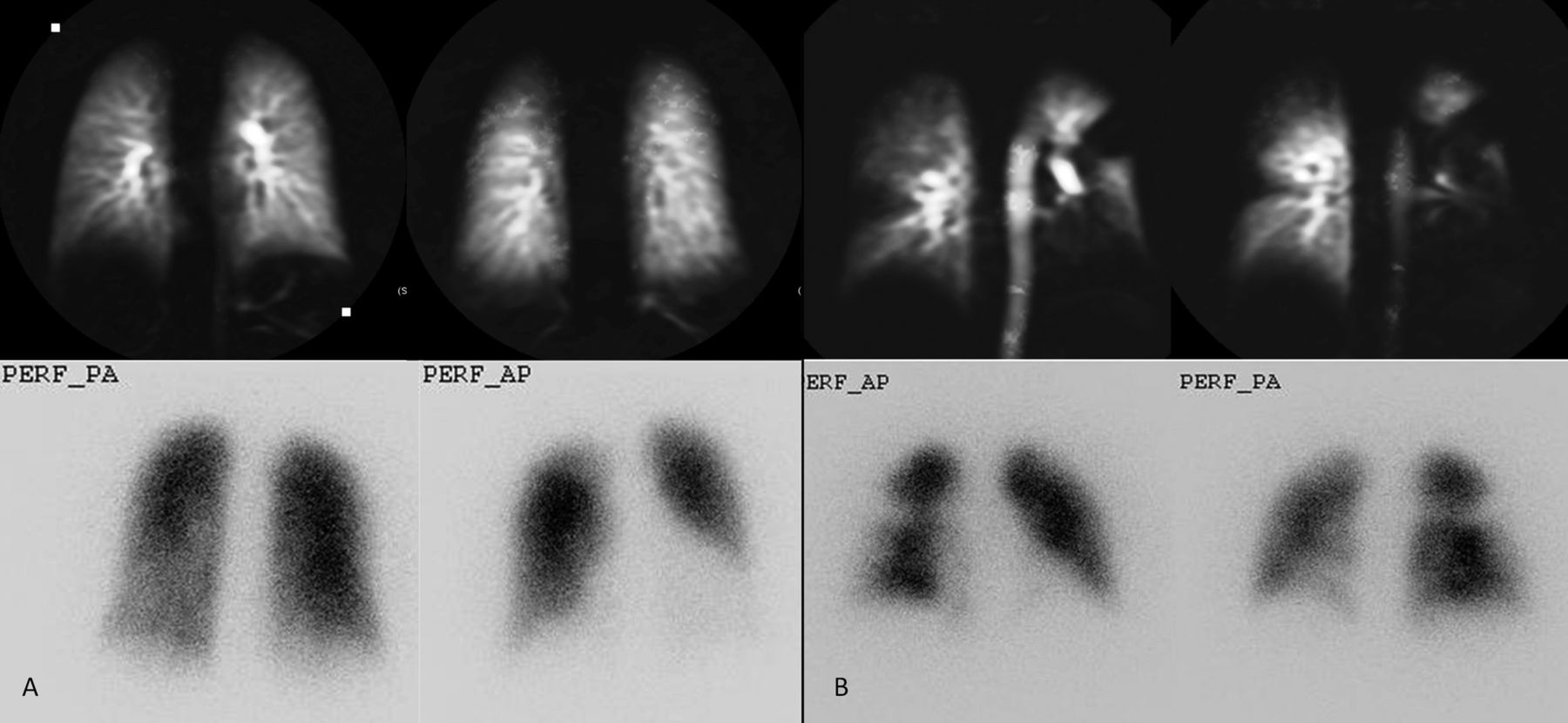
(A) Selected coronal images of MR lung perfusion (top) and anterior and posterior view of perfusion scintigraphy images (bottom) in a patient with normal lung perfusion. (B) An example of a patient with chronic thromboembolic pulmonary hypertension with bilateral segmental perfusion defects seen on MR perfusion images (top) and perfusion scintigraphy (bottom).
Accurate diagnosis of CTEPH is essential to identify a potentially treatable cause of PH. Here it is demonstrated that 3D lung perfusion MRI, as part of a pulmonary–vascular MRI protocol, has very high sensitivity for the diagnosis of CTEPH similar to that of perfusion scintigraphy and CTPA. The 3D data set allows image reconstruction in any plane, enabling better assessment of regional perfusion abnormalities and has superior temporal and spatial resolution to scintigraphy.
In conclusion, 3D lung perfusion MRI has high sensitivity for CTEPH and complements MR angiography and functional cardiac MRI in a single comprehensive radiation-free imaging modality in the evaluation of patients with suspected CTEPH.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
-
Competing interests None.
-
Ethics approval Sheffield teaching hospitals.
-
Provenance and peer review Not commissioned; internally peer reviewed.