Recent Advances: Cardiology - I: Treatment of myocardial infarction, unstable angina, and angina pectoris
BMJ 1994; 309 doi: https://doi.org/10.1136/bmj.309.6965.1343 (Published 19 November 1994) Cite this as: BMJ 1994;309:1343
- J McMurray,
- A Rankin
- Department of Cardiology, Western General Hospital, Edinburgh EH4 2XU University Department of Medical Cardiology, Royal Infirmary, Glasgow G31 2ER
- Correspondence to: Dr McMurray.
In the past 12 months there have been many advances in our understanding of how to treat heart disease. In the first part of this two part review we summarise the most important of these advances in the treatment of myocardial infarction, unstable angina, and angina pectoris. A glossary of study abbreviations is given in the appendix.
Myocardial infarction and thrombolysis Early thrombolysis
Two recent large trials, EMIP and the MITI project, have compared thrombolysis started before admission to hospital with that started in hospital, which adds to the findings of GREAT (table I).*RF 1-3* The results of EMIP and the MITI project were much less encouraging than those of GREAT, showing only a marginal benefit during short term follow up for prehospital treatment over hospital treatment (table I). This difference between GREAT and the two recent trials probably reflects the much shorter delay in starting thrombolysis in hospital in EMIP and the MITI project. This, in part, reflected the effect of the trials on “usual practice.” In EMIP the median time from arrival in hospital to injection was only 15 minutes compared with over 80 minutes in recent British and American surveys.4 In support of this, patients in the MITI project who were treated within 70 minutes of the onset of symptoms had a mortality in hospital of only 1.2% compared with 8.7% in those who were not treated within 70 minutes (P=0.04). The clear message of these studies is the earlier treatment is given the better: when matters more than where.
Trials of prehospital thrombolysis
Initiating thrombolysis just 30-60 minutes earlier, the sort of time saving that can be achieved by regular audit and the introduction of fast track systems, will typically save about 15 extra lives for each 1000 patients treated (see discussion of GUSTO study below).4 An even greater benefit may be obtained if treatment is given within the first hour after the onset of symptoms (fig 1).5
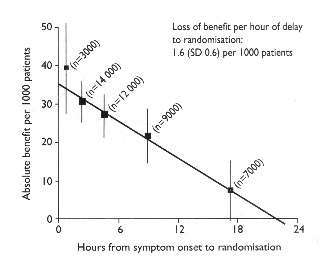
Time dependent benefits of thrombolysis. Graph shows absolute reduction in mortality at 35 days v delay from onset of symptoms to randomisation among 45 000 patients with ST elevation or bundle branch block. Vertical lines show standard deviation5
A British Heart Foundation working group has recommended that the time between calling the emergency services and receiving thrombolysis should ideally be less than 60 minutes and certainly no more than 90 minutes.4 Initiating thrombolysis before arrival in hospital may need to be considered if it is the only way to achieve the 90 minute target - for example, in rural areas.
Late thrombolysis
Two large trials have investigated whether thrombolysis is beneficial to patients presenting late after the onset of symptoms of myocardial infarction.6,7 This question has also been addressed by the Fibrinolytic Therapy Trialists' Collaborative Group.5
In the LATE study 5711 patients with electrocardiographic evidence of myocardial infarction who presented more than six hours after the onset of symptoms were randomly assigned to placebo or alteplase.6 By intention to treat analysis, thrombolysis up to 12 hours after the onset of symptoms was worth while (table II). A similar trend was seen in EMERAS, which randomly assigned patients who presented late to placebo or streptokinase (table II).7
Mortality (%) 35 days after infarction in patients receiving late thrombolysis for acute myocardial infarction
By intention to treat analysis, neither the LATE study nor EMERAS showed any benefit in patients treated more than 12 hours after the onset of symptoms. A further analysis of the LATE study, however, suggested that these patients might represent two distinct subgroups - that is, those presenting late with typical symptoms and electrocardiographic changes and those treated late because of initial diagnostic uncertainty due to atypical features. The first group seemed to get benefit from thrombolysis given 12-24 hours from the onset of symptoms.
The overview by the Fibrinolytic Therapy Trialists' Collaborative Group also supports treatment between 6 and 12 hours (table II).5 The number of patients treated beyond 12 hours in existing trials was considered to be too small to permit any conclusion about the value of thrombolysis between 13 and 24 hours.
Thrombolytic regimens
In the multinational GUSTO trial 41 021 patients with acute myocardial infarction who presented within six hours of the onset of chest pain were randomly assigned to one of four thrombolytic regimens (table III).8 In contrast to the protocol of two other international studies (ISIS 3 and the GISSI 2 study), tissue plasminogen activator (alteplase) was given rapidly (“accelerated” or “front loaded”) and with intravenous heparin.*RF 9-11* Two groups received streptokinase at conventional doses, one with subcutaneous and the other with intravenous heparin. The fourth group received alteplase, streptokinase, and intravenous heparin.
Fewer deaths but more strokes occurred in the group given alteplase rapidly than in the three groups given streptokinase (table III).8 Intravenous heparin did not increase the efficacy of streptokinase and seemed to increase the risk of bleeding and stroke.
Results of GUSTO trial of different thrombolytic regimens8
Compared with streptokinase and subcutaneous heparin there were nine fewer deaths but three extra strokes (one fatal, one non-fatal but disabling, and one non-fatal and not disabling) with alteplase (table III). The absolute benefit (reduction in mortality minus increase in stroke) was less in those over 75 years because of the increased rate of stroke in this group (net benefit 4.2 per 1000 patients treated). The beneficial effect on mortality was greater in anterior myocardial infarctions (19 deaths prevented per 1000 patients treated compared with 6 per 1000 for other infarctions).
The benefit of the combined thrombolytic regimen was less than that of alteplase alone and no better than that of streptokinase.
The significance of these findings is controversial, and the conduct and analysis of this study have been the subject of greater scrutiny and debate than those of any previous clinical trial in cardiology. It has been argued that the conduct of the trial, data analysis, and presentation of the results favours altepalse over streptokinase. Many patients (especially in the United States) in the group given streptokinase and subcutaneous heparin also received intravenous heparin, which could have reduced the difference in stroke rate between the groups given alteplase and streptokinase and subcutaneous heparin. More patients given alteplase underwent coronary artery bypass grafting, which possibly contributed to the lower mortality in these patients. Alteplase had a more beneficial effect on mortality in the United States than in other countries, possibly because American physicians are less familiar with streptokinase and may have discontinued treatment with this agent during the trial when patients became hypotensive. All of these potential biases are considered to be worrying because the GUSTO trial was unblinded. Concern has also been expressed at how the results were presented: overall mortality and stroke rate will be increased with streptokinase if the streptokinase groups are combined, thus favouring alteplase. Alteplase was, of course, given rapidly whereas streptokinase was given conventionally. How alteplase given conventionally might compare with streptokinase given conventionally or streptokinase given rapidly compare with alteplase given rapidly is not known. Clearly, a great deal of this controversy is generated by the huge price differential between the two thrombolytic agents. Because of the cost implications of switching from streptokinase to alteplase, it is important to be sure how real and how large the differences in outcome are. Not only must the cost of the thrombolytic agents be considered but also the cost of intravenous heparin and its monitoring. The substantial cost of treating stroke must also be taken into account. Essentially the argument boils down to what is a worthwhile benefit? How does one assess a relatively small benefit obtained at great monetary cost?
One important and non-controversial conclusion can be drawn from the GUSTO trial taken in conjunction with the trials of prehospital thrombolysis and the overview of the Fibrinolytic Therapy Trialists' Collaborative Group.*RF 1-3,5* The choice of thrombolytic strategy is much less important than the delay to the onset of treatment. Initiating treatment 30-60 minutes earlier can save as many or more lives as substituting accelerated alteplase for conventional streptokinase (fig 1).
Benefit of aspirin or warfarin afterwards
In the APRICOT study 300 patients were randomly allocated to placebo, aspirin, or warfarin (Coumadin) after they had been given angiographically successful thrombolysis with streptokinase or anistreplase.12 Angiography was repeated at three months. Aspirin was superior to placebo and warfarin in preventing clinical events and preserving ventricular function (table IV). There was no significant benefit of aspirin in preventing coronary reocclusion, the rate being high in all three groups.
Results of APRICOT study after 3 months12
Previous studies such as WARIS and the ASPECT study have shown a benefit of warfarin after myocardial infarction, but few trials have compared warfarin with aspirin.13 The APRICOT study suggests aspirin is to be preferred, though the results of further comparative studies - for example, CHAMP - and, particularly, combination trials - for example, CARS, CHAMP - are eagerly awaited.
Acute myocardial infarction and coronary angioplasty
The role of percutaneous transluminal coronary angioplasty in acute myocardial infarction continues to be defined (fig 2). Immediate routine angioplasty and deferred routine angioplasty after thrombolysis are not of benefit.

Strategies for percutaneous transluminal coronary angioplasty in acute myocardial infraction in randomised trials
Four recent studies have compared so called primary angioplasty with thrombolysis (table V).14 15 16 17 Experienced operators in tertiary centres with rapid access to cardiac catheterisation laboratories obtain very good results in selected patients with acute myocardial infarction. Collectively, these studies suggest that in such circumstances primary percutaneous transluminal coronary angioplasty may be better than thrombolysis. Even if this benefit is confirmed by further studies, the widespread adoption of primary angioplasty as a routine treatment for acute myocardial infarction is impractical. Patients who cannot receive thrombolytic treatment - for example, because they have active peptic ulceration - might be considered for primary angioplasty if they have been admitted under the care of a cardiologist experienced in the procedure who can gain rapid access to a cardiac catheterisation laboratory.
Results of trials comparing outcome of thrombolysis with that of angioplasty
Rescue or salvage angioplasty for patients who have not shown coronary reperfusion with thrombolysis is a new strategy (fig 2), which is under evaluation in the RESCUE trial.
Myocardial infarction and angiotensin converting enzyme inhibitors
Five large randomised trials of the use of angiotensin converting enzyme inhibitors after myocardial infarction have been published or presented (fig 3).18 One of these is the AIRE study, which is one of the most important clinical trials in cardiovascular medicine to be published for many years.19 In the AIRE study 2006 patients with acute myocardial infarction complicated by signs of left ventricular failure, even if only transient, were randomly allocated to placebo or ramipril which was given in addition to full conventional treatment (fig 4). Treatment was started in stable patients between day 3 and day 10 (mean 5.4 days) after admission. Mean follow up was 15 months.

Randomisation times in trials of angiotensin converting enzyme inhibitors in myocardial infarction

{kind=link}
{kind=link}
{kind=link}
{kind=link}
The principal outcome measure was mortality. Ramipril 5 mg twice daily reduced absolute mortality by 6% (relative reduction 26%), preventing 45 premature deaths per 1000 patient years of treatment. This benefit is at least as large as that obtained with many standard treatments and is in addition to those of conventional treatment (table VI). There is no doubt that patients with clinical or radiological left ventricular failure (the AIRE study) or asymptomatic left ventricular dysfunction (the SAVE study) should routinely receive an angiotensin converting enzyme inhibitor after myocardial infarction.
Relative benefits of treatments for myocardial infarction
The GISSI 3 study was published most recently.20 It and the unpublished ISIS 4 differed greatly from previous trials in that oral treatment was initiated early (within 24 hours) in largely unselected, normotensive patients and was continued for six weeks (four weeks in ISIS 4) (fig 3). The GISSI 3 study and ISIS 4 can be regarded as having recruited a large number of low risk patients in addition to the higher risk patients recruited in the AIRE and SAVE studies (fig 5). Many very high risk patients - that is, those who would have died before they became eligible for the later entry trials - were, however, also included in the GISSI 3 study and ISIS 4. In the GISSI 3 study lisinopril prevented eight premature deaths per 1000 patients treated (captopril prevented five per 1000 in ISIS 4). The results of these trials add to the debate about who to treat, when to treat, and how long to treat with an angiotensin converting enzyme inhibitor after myocardial infarction.

Degree of risk of patients recruited in trials of angiotensin converting enzyme inhibitors after myocardial infarction with premature deaths prevented
{kind=link}
The benefits seen in the AIRE and SAVE studies were substantial, and most cardiologists would now routinely use angiotensin converting enzyme inhibitors in the types of patients recruited into these trials. The size of the benefit in the GISSI 3 study and ISIS 4 is much smaller and is similar to that obtained with intravenous ß blockers. Its clinical significance has been vigorously debated. Some argue that a valuable incremental benefit has been shown and that it justifies treatment according to the protocols of the two studies. Others argue that this benefit is too small to justify widespread treatment of patients who have had a myocardial infarction with yet another drug. This debate centres around the question of what is a worthwhile benefit and, as with the GUSTO study,8 reflects the difficulty in further reducing mortality in patients receiving thrombolysis for myocardial infarction.
Subgroup analysis of the GISSI 3 study and ISIS 4 may help in this debate. Greater absolute benefit (perhaps 10-20 premature deaths prevented per 1000 patients treated) can be obtained if only higher risk patients - for example, those with acute heart failure, previous myocardial infarction, and anterior myocardial infarction - are treated (fig 6). The AIRE and SAVE studies suggest that there is continuing benefit from long term treatment in high risk patients. The alternative strategy is to treat all patients initially and stop treatment after 4-6 weeks in patients with normal ventricular function.

Flow chart showing how to maximise benefits of treatment with angiotensin converting enzyme inhibitors after myocardial infarction
{kind=link}
An equally difficult question is when to start treatment. The GISSI 3 study shows at that treatment started within the first 24 hours causes few significant adverse effects and has a net clinical benefit. The most common adverse effect of lisinopril was persistent hypotension, which was seen in 9.0% of treated patients compared with 3.7% of control patients. Hypotension after myocardial infarction is, however, associated with a higher mortality, and the possibility exists that hypotension induced by angiotensin converting enzyme inhibitors has an adverse prognostic effect - that is, it reduces the potential net benefit of this form of treatment. It has been suggested that hypotension might be more common if an angiotensin converting enzyme inhibitor is given within the first 24 hours after infarction, though the different patient populations and definitions of hypotension used in the studies make it impossible to be certain about this. Until this issue is resolved, it is probably best to reserve angiotensin converting enzyme inhibitors for patients who are clinically stable with a blood pressure above 100 mm Hg within the first 24 hours after infarction.
Myocardial infarction and calcium channel blockers
SPRINT 2 randomly allocated patients to placebo or nifedipine 60 mg/day within 48 hours of admission with acute myocardial infarction. The study was terminated early by its review committee after 1358 patients had been recruited. The trial was halted because of a trend towards a worse outcome in the group given nifedipine. Mortality at six months in the nifedipine group was 15.4% compared with 13.3% in the placebo group.
SPRINT 2 adds to a long list of trials showing a neutral effect on mortality of calcium blockers in acute myocardial infarction or unstable angina. Further analysis of these trials even suggests that dihydropyridine calcium channel blockers may have an adverse effect on death and reinfarction. Rate limiting calcium channel blockers such as verapamil and diltiazem may be of benefit in preventing reinfarction, although diltiazem may increase the risk of developing heart failure.
The routine use of calcium channel blockers should be avoided after myocardial infarction.
Myocardial infarction and smoking
Smoking plays an important part in the development of coronary artery disease. Smoking cessation therefore has an important role in the primary and secondary prevention of myocardial infarction. Survival five years after a myocardial infarction is about 17% in those who stop smoking and 30% in those who do not. Thus, stopping smoking can prevent as many as 27 deaths per 1000 patients years of treatment.
Nicotine replacement helps people stop smoking and may be safely used in patients with coronary artery disease.23 Three large meta-analyses of nicotine replacement have been published recently.*RF 24-26* Nicotine patches seem to be better than gum, and efficacy seems to be independent o type, dose of patch, counselling, duration of treatment (there was no value in extending treatment beyond eight weeks), or weaning. Meta- analysis of 17 studies of 5098 patients showed a cessation rate at six months of 9% in subjects who wore placebo patches compared with 22% in those who wore nicotine patches. In another analysis abstinence in the first two weeks of treatment seemed to be the strongest predictor of not smoking in the long term.27 The role of nicotine replacement in helping people to stop smoking after a myocardial infarction should be explored further.
Unstable angina and aspirin or heparin, or both
Both aspirin and heparin have been shown to reduce the risk of myocardial infarction and death in patients with unstable angina. Which is more effective and whether there is any advantage in combining the two treatments was not known until recently.
Theroux et al have extended their previous observations to report a six day comparison of heparin (5000 unit intravenous bolus and infusion to keep the partial thromboplastin time 1.5-2.5 times control values) with aspirin (650 mg oral loading dose and 325 mg twice daily maintenance dose) in 484 patients with unstable angina.28 Two (0.8%) patients taking heparin and nine (3.7%) taking aspirin developed myocardial infarction (P=0.035). The only death occurred in the aspirin group. Thus, treating 100 patients with heparin rather than aspirin will prevent three more patients developing myocardial infarction.
What about heparin and aspirin? The ATACS trial compared aspirin (162.5 mg/day) with aspirin plus anticoagulant with heparin followed by warfarin in 214 patients with unstable angina or non-Q wave myocardial infarction. The primary outcome measure was the combined end point of recurrent angina, myocardial infarction, or death. By 14 days one or more of these events occurred in 27% of the group taking aspirin and in 10.5% of the group taking aspirin plus an anticoagulant (P=0.004). By three months there was no significant difference in outcome between the two groups, though there was still a trend in favour of the combined treatment.
These new studies, taken together with previous studies (table VII), show that heparin is more effective than aspirin but that combined treatment with aspirin and heparin is even better. Aspirin has also been shown to prevent reactivation of unstable angina after stopping heparin. The ATACS trial does not clearly show that the addition of warfarin to aspirin leads to any further benefit during this phase, though the power of the trial definitively to exclude a benefit is limited.
Risk of death/myocardial infarction with aspirin and/aspirin plus heparin in unstable angina*
Heparin should be given routinely in the acute phase of unstable angina together with aspirin.
Unstable angina and thrombolysis
In the TIMI IIIB trial 1473 patients with unstable angina or non-Q wave myocardial infarction were randomly allocated to alteplase or placebo.30 The primary end point was an “unfavourable outcome,” defined as death, myocardial infarction, or failure of initial treatment - that is, the occurrence of spontaneous or evoked ischaemia - by the time of a follow up exercise test and clinical review at six weeks.
In the whole group (unstable angina and non-Q wave myocardial infarction) an unfavourable outcome occurred in 54.2% of the patients given alteplase and 55.5% of those given placebo (NS). Death or myocardial infarction occurred in 9.1% of patients with unstable angina given alteplase and in 5.0% of those given placebo (P=0.01). In the group as a whole there was a strong trend of an excess of intracranial haemorrhage in patients receiving alteplase.
Thrombolysis should not be used in patients with unstable angina.
Unstable angina and early angioplasty or surgery
The TIMI IIIB trial also compared two investigative strategies in patients with unstable angina.30 The first was an early invasive strategy of routine cardiac catheterisation within one or two days of admission, followed, if possible, by “revascularisation” by percutaneous transluminal coronary angioplasty or, in patients with left main coronary disease andmultivessel disease with impaired left ventricular function, coronary artery bypass grafting.
The second was an early conservative strategy that reserved catheterisation for patients having spontaneous or evoked ischaemia - that is, on stress testing. In the six weeks of follow up 98% of patients in the early invasive group underwent catheterisation and 61% had a revascularisation procedure. In the early conservative group the respective rates at six weeks were 64% and 49%. The principal composite end point was death, myocardial infarction, or a failed symptom limited exercise test by the time of the follow up visit at six weeks. This end point was reached in 16.2% of the early invasive group and 18.1% of the early conservative group (NS). In older patients (>=65 years) the respective rates were 7.9% and 14.8% (P=0.02). The average length of stay in hospital (10.9 v 10.2 days, P<0.01), rate of readmission (14.1 v 7.8 days, P<0.001), and number of antianginal doses taken (P=0.02) were higher in the conservative group.
The authors concluded that neither strategy had a major advantage over the other. Patients treated conservatively required more antianginal drugs and were readmitted to hospital more often, but they did not seem to experience an increased risk of myocardial infarction or death. On the other hand, more cardiac catheterisations and revascularisation procedures were required in the early invasive group. Both strategies are endorsed by new American guidelines on the management of unstable angina.31
Angina pectoris and interventional cardiology
Important new guidelines on the management of angina pectoris have been produced by the British Cardiac Society and the Royal College of Physicians of London.32
Angioplasty v bypass surgery
At the time of writing, three randomised trials comparing percutaneous transluminal coronary angioplasty and coronary artery bypass grafting have been published in full (table VIII).*RF 33-35*
The Lausanne study compared percutaneous transluminal coronary angioplasty with left internal mammary artery grafting in patients with an isolated proximal stenosis of the anterior descending branch of the left coronary artery and normal left ventricular function.35 After two years the composite end point of death, myocardial infarction, and further revascularisation (percutaneous transluminal coronary angioplasty or coronary artery bypass grafting) was less frequently reached in the group given left internal mammary artery grafting (table VIII). There was also a trend (P=0.07) for more patients in this group to be symptom free, and they required less antianginal treatment.
Trials comparing percutaneous transluminal coronary angioplasty with coronary artery bypass grafting in patients with angina
The RITA trial was a large multicentre study in the United Kingdom which compared outcome after equivalent revascularisation by coronary artery bypass grafting or percutaneous transluminal coronary angioplasty in patients with severe angina and disease in one, two, or three coronary arteries (table VIII).33 After 2.5 years of follow up the composite end point of death, myocardial infarction, and further revascularisation was less frequent in the group given coronary artery bypass grafting (table VIII). At six months 11% of patients who received coronary artery bypass grafting and 32% of those who received angiography reported having angina (P<0.001). At two years the rates were 22% and 31% (P=0.007). At six months 75% of patients who had percutaneous transluminal coronary angioplasty and 28% of those who had coronary artery bypass grafting were taking at least one antianginal drug. By two years these rates were 61% and 34% (all differences significant).
ERACI was a smaller study than the RITA trial but had the same aim, though more patients with unstable angina and multivessel disease were enrolled (table VIII). Only follow up after one year has been published. The clinical outcomes in this trial were broadly similar to those of the Lausanne study and the RITA trial. In terms of cost, coronary artery bypass grafting was initially more expensive ($12 812 v $4286 (pounds sterling8541 v pounds sterling 2857)), but by the end of the year follow up this difference had decreased ($12 937 v $6952 (pounds sterling 8625 v pounds sterling 4635)).
There is no doubt that both percutaneous transluminal coronary angioplasty and coronary artery bypass grafting are effective treatments for angina. These three trials and a the similar but published EAST, GBI and CABRI studies show that, in the medium term - that is one to two years - coronary artery bypass grafting does not carry any greater initial risk and is more effective at relieving angina in patients with one, two, and three vessel disease. This advantage, however, is obtained at the cost of the inconvenience and discomfort of surgery, a longer recovery time, and a greater initial expenditure.
Whether the advantage of coronary artery bypass grafting over percutaneous transluminal coronary angioplasty is sustained in the longer term will await further follow up of these trials. Restenosis in patients receiving percutaneous transluminal coronary angioplasty is likely to be more of a problem in the early follow up period whereas graft failure after coronary artery bypass grafting will be a problem in the longer term.
There is also the further clinical question of whether the two treatments should be regarded as alternative or complementary treatments. If they are complementary angioplasty might be performed initially, reserving bypass grafting for later in the natural history of what tends to be a progressive disease. In the United Kingdom, where waiting lists for bypass grafting are long, this is a particularly relevant question. BARI is testing the hypothesis that an initial treatment strategy of percutaneous transluminal coronary angioplasty rather than coronary artery bypass grafting does not compromise survival, which will help to answer this question.
Coronary atherectomy v balloon angioplasty
Two randomised trials comparing directional coronary atherectomy and conventional balloon angioplasty have been published (fig 7, table IX).36,37 A higher initial success rate and reduced risk of restenosis were hoped for, leading to improved clinical outcome. Despite better initial angiographic appearances, both studies failed to show any clinical advantage of directional coronary atherotomy over balloon angioplasty.

Interventions to open atheromatous coronary arteries (a): percutaneous transluminal coronary angioplasty (b); insertion of intravascular stent (c); and directional atherectomy, in which the plaque shaved off by cutter is trapped in cutting chamber and removed through catheter (d)
{kind=link}
Comparison of directional coronary atherectomy and coronary balloon angioplasty in patients with angina and coronary artery disease
Enthusiasts for directional coronary atherotomy believe that certain types of lesions - for example, in vein grafts, ostial stenoses - may still be better treated by atherectomy, though this remains to be proved.
Adjuncts to angioplasty Platelet monoclonal antibodies
The EPIC investigators have reported the short and long term effects of the platelet glycoprotein IIb/IIIa receptor monoclonal antibody fragment c7E3 Fab in high risk patients undergoing percutaneous transluminal coronary angioplasty - that is, those with evolving myocardial infarction, unstable angina, angina after myocardial infarction, and high risk lesions.38,39
A total of 2099 patients received either a placebo bolus and 12 hour placebo infusion, a c7E3 Fab bolus and placebo infusion, or a bolus and infusion of c7E3 Fab. These study treatments were given in addition to aspirin and intravenous heparin. The 30 days primary study end point was death, myocardial infarction, unplanned revascularisation, unplanned coronary stent implantation, or insertion of an intra-aortic balloon pump for refractory ischaemia. This combined end point occurred in 12.8% of patients given dual placebo, 11.5% of patients given the c7E3 Fab bolus, and 8.3% of patients given the bolus and infusion of c7E3 Fab (dual placebo v dual c7E3 Fab P=0.008). Bleeding complications were increased in the groups given c7E3 Fab.
The outcome at six months has also been reported. A major ischaemic event or elective revascularisation occurred in 35.1% of patients given placebo and 27.0% patients given a bolus or infusion of c7E3 Fab (P=0.001). This favourable outcome was due to less need for coronary artery bypass grafting and repeat target vessel percutaneous transluminal coronary angioplasty (22.3% v 16.5%, P=0.007).
This finding is of great interest as it may be the first evidence of a pharmacological agent reducing the clinical restenosis rate after percutaneous transluminal coronary angioplasty.
Intracoronary stents
There are two major current limitations to percutaneous transluminal coronary angioplasty. Firstly, dissection of the arterial wall may be caused by barotrauma and can lead to acute coronary occlusion during 2-10% of procedures. The second limitation is coronary restenosis. Clinical restenosis occurs in about a third of patients within six months. Intracoronary stent placement may prevent acute occlusion and reduce chronic restenosis (fig 7).40
Emergency stent placement - Most occlusive coronary dissections in large vessels can be repaired by placement of one or more stents, and in many patients emergency coronary artery bypass grafting can be avoided. Full immediate (heparin) and long term (warfarin) anticoagulant treatment is required, which can lead to initial bleeding problems especially at the site of arterial puncture. A prolonged stay in hospital may be required to ensure adequate and stable anticoagulation. Stent thrombosis can clearly have fatal consequences.
Elective stent placement to reduce restenosis - The BENESTENT study and STRESS have evaluated elective Palmaz-Schatz stent placement as a means of preventing coronary restenosis after percutaneous transluminal coronary angioplasty. The preliminary results of these trials have recently been presented.40 In the BENESTENT study (520 patients) elective repeat revascularisation was required in 22.1% of control patients and 13.5% of patients with stents. Survival free of events at six months was 67% in the control patients and 79% in the stent group (P<0.03). In STRESS (410 patients) repeat target lesion revascularisation was required in 16% of the control group and 9.7% of the stent group. Survival free of events at six months was 73% in the control group and 80% in the stent group (P=0.084). The thrombosis rate was 3.5% in both studies, and bleeding and local vascular complications were more frequent in the groups with stents. A full report of both studies, to allow detailed evaluation of the risk benefit ratio, is awaited with interest. Careful economic evaluation of these trials is also merited in the light of the cost of stents (around pounds sterling 900 each) and the cost of anticoagulant treatment and longer stays in hospital.
Further trials are awaited - for example, concerning saphenous vein grafts. New strategies that allow preanticoagulation and a reduced length of stay in hospital - for example, using a brachial or radial arterial approach - are under evaluation.
Recent advances in cardiology
Myocardial infarction
Timing of thrombolysis
Coronary angioplasty
Treatment with angiotensin converting enzyme inhibitors
Nicotine replacement therapy
Unstable angina
Combined treatment with heparin and aspirin
Early angioplasty and surgery
Angina pectoris
Percutaneous transluminal coronary angioplasty
Coronary artery bypass grafting
Directional coronary atherectomy
Use of platelet monoclonal antibodies and intracoronary stents as adjuncts to angiography
Appendix
Study abbreviations
AIRE, acute infarction ramipril efficacy
APRICOT, aspirin versus Coumadin [warfarin sodium] in the prevention of reocclusion
ASPECT, anticoagulants in the secondary prevention of events in coronary thrombosis
ATACS, antithrombotic therapy in acute coronary syndromes
BARI, bypass angioplasty revascularisation investigation
BENESTENT, Belgium and Netherlands stent
CABRI, coronary artery bypass revascularisation investigation
CARS, Coumadin aspirin reinfarction study trials
CHAMP, combination haemotherapy and mortality prevention
CONSENSUS II, cooperative new Scandinavian enalapril survival study II
EAST, Emory angioplasty versus surgery trial
EMERAS, estudio multi centrico estreptoquinasa republicas de America
del sur ECSG, European cooperative study group EMIP, European myocardial infarction project
EPIC, evaluation of 7E3 for the prevention of ischaemic complications
ERACI, Argentine randomised trial of PTCA versus coronary artery bypass surgery in multivessel disease
GABI, German angioplasty bypass investigation
GISSI, Gruppo Italiano per lo studio della Sopravvivenza nell'Infarto
Miocardico
GREAT, Grampian region early anistreplase trial
GUSTO, global utilisation of streptokinase and tissue plasminogen activator for occluded coronary arteries
ISIS, international study of infarct survival
LATE, late assessment of thrombolytic efficacy
MITI, myocardial infarction triage and intervention
PAMI, primary angioplasty in myocardial infarction study group
RESCUE, randomised evaluation of salvage angioplasty with combined utilisation of endpoints
RISC, research group on instability in coronary artery disease in south east Sweden
RITA, randomised intervention treatment of angina
SAVE, survival and ventricular enlargement
SPRINT, secondary prevention reinfarction Israel nifedipine trial
STRESS, stent restenosis trial
SWIFT, should we intervene after thrombolysis
TIMI, thrombolysis in myocardial infarction I, IIA, IIB, IIIB
WARIS, warfarin reinfarction study