Article Text

Statistics from Altmetric.com
Learning objectives
To recognise spontaneous coronary artery dissection (SCAD) as a cause of myocardial infarction in low-risk, predominantly female, patients and to understand that although SCAD is an important cause of peripartum myocardial infarction, ~90% of incident cases are not pregnant.
To be aware that a visible dissection flap at angiography is absent in the majority of cases.
To understand the rationale for an ‘as conservative as possible’ approach to revascularisation and key challenges in medical treatment.
Introduction
Spontaneous coronary artery dissection (SCAD) is an increasingly recognised cause of non-atherosclerotic acute coronary syndromes leading to myocardial infarction. It is characterised by the presence of blood entering and separating the layers of the coronary arterial wall to form a false lumen. This leads to external compression of the true coronary lumen restricting coronary blood flow and leading to coronary insufficiency (figure 1). SCAD should be distinguished from atherosclerotic dissections arising from plaque rupture events or erosions allowing blood to enter the intimal space and from iatrogenic dissections arising during coronary procedures.

Pathophysiology of SCAD. A spontaneous haematoma forms in the outer media of a coronary artery forming an FL. This then compresses the artery from the outside restricting blood flow in the TL with typical histological and angiographic appearances. FL, false lumen; SCAD, spontaneous coronary artery dissection; TL, true lumen.
Epidemiology
The true incidence of SCAD is unknown, largely because most patients fall into the lowest risk categories for conventional atherosclerotic disease leading to underdiagnosis and probably lower rates of presentation by patients.1 Historically thought to be very rare, increasing use of high-sensitivity troponin with early angiography for the assessment of acute chest pain presentations has led to a greater recognition of SCAD. However, accurate angiographic diagnosis can be challenging and reported rates of SCAD diagnosis from angiographic registries (0.2%–0.7% of angiograms; 2.0% of ACS angiograms)2 3 probably significantly under-represent true SCAD incidence. There are currently no blood biomarkers which distinguish SCAD from other causes of ACS.
SCAD overwhelmingly affects young to middle-aged women with men accounting for less than 10% of cases in most large contemporary series.4–8 Indeed around a quarter of ACS presentations in women under the age of 50 are reportedly due to SCAD.8 9 The mean age of affected patients ranges from 42 to 53 years, but the condition has been reported in patients aged 18–84 years.4 5
Pregnancy
Although historically described primarily in the context of peripartum myocardial infarction, SCAD associated with pregnancy is now recognised to account for a small proportion of the overall disease burden (5%–18%).4 8 SCAD may, however, cause a significant proportion of peripartum myocardial infarctions, predominantly occurring late in gestation or early, late or sometimes very late in the postpartum period.10–12 Some evidence suggests that multiparity might be a risk for pregnancy associated SCAD.7 13
Mechanical stressors
SCAD may be precipitated by Valsalva-type manoeuvres such as coughing,14 vomiting,15 heavy lifting16 or by extreme or isometric exercise.17–19 It is hypothesised that this results from transient increases in coronary wall shear stress. In some cases however, there seems to be a significant lag time between the last exercise episode and the onset of symptoms of SCAD, suggesting high exercise capacity may be part of the phenotype of a patient with SCAD rather than a direct cause of the dissection. An association with exercise is more frequent in male SCAD cases.20 Altered coronary shear stress and vasoreactivity may also explain the rare case reports associating SCAD with cocaine,21–23 amphetamine use5 24 25 and a possible association with migraine.26
Emotional stressors
Emotional stress and sometimes preceding physical illness are reportedly associated with SCAD events, with apparent emotional precipitants more common in female patients.5 8 20
Connective disorders, autoimmune and inflammatory disorders
There are several reports of SCAD in patients with known connective tissue disorders (eg, Marfan,27 Ehler-Danlos type 4,28 Loeys-Dietz syndromes29 and adult polycystic kidney disease).30–33 However, specific genetic testing in SCAD survivors has a low yield.34 Likewise, SCAD has been rarely reported in association with autoimmune/inflammatory disorders including Behcets,35 systemic lupus erythematosus,36–41 polyarteritis nodosa42 and inflammatory bowel disease,43 but again these cases represent rare associations rather than typical presentations.
Presentation
Patients with SCAD present with acute coronary syndromes, usually with chest pain associated with an elevation of cardiac enzymes.44 The proportion of patients presenting with ST-segment elevation (STEMI) versus non-ST-segment elevation (NSTEMI) varies between series with some reporting a dominance of STEMI4 6 8 and others NSTEMI.5 7 This likely reflects differences in patient selection between studies with the former series likely under-representing patients with less severe presentations. A small proportion (3%–14%) presents with resuscitated ventricular arrhythmia.4–6 Some cases present as unexplained sudden death, although, because of the challenges of accurate postmortem diagnosis, this condition is likely under-represented in postmortem series.45 46
Patients with SCAD too frequently suffer from failed or delayed diagnosis.44 This primarily results from emergency medical systems targeted to screen patients with acute chest pain presentations on the basis of traditional atherosclerotic cardiovascular risk factors. As a result, some patients with SCAD are not appropriately referred for coronary angiography or referral is delayed. A high index of clinical suspicion is required for women presenting with typical chest pain and abnormalities of either ECG or cardiac biomarkers.
Angiographic findings
While recognition of typical angiographic features and use of intracoronary imaging is improving accurate diagnosis, this condition remains under-recognised at angiography.9 47
Angiographic classification
One key area of persisting misunderstanding is an expectation that the false lumen in SCAD will usually be angiographically apparent. Saw et al 44 described an angiographic classification for SCAD which has been increasingly adopted. Type 1 angiographic SCAD (figure 2A) is characterised by an identifiable false lumen with a linear filling defect or dissection ‘flap’. There is often contrast hold-up in the false lumen after clearance from the true lumen. This appearance is familiar to interventional cardiologists from catheter or interventional procedure-induced dissections where contrast readily enters the false lumen. However, such cases make up a minority of SCAD angiograms (29%–48%). More common are type 2 lesions where contrast penetration of the false lumen is not evident. In type 2a (figure 2B) lesions, there is distal reconstitution of a normal vessel calibre (often preceded by a tapered critically narrowed segment at the distal extent of the dissection). In type 2b lesions (figure 2C), the stenosis continues to the distal extent of the affected coronary territory. Type 2 lesions account for 52% to 67% of presentations. Type 3 lesions (figure 2D) are angiographically indistinguishable from atherosclerosis without recourse to intracoronary imaging but appear rare (2%–3.9% of cases). We would also propose a type 4 variant (figure 2E) which presents with a total, usually distal, vessel occlusion where sources of coronary embolism have been excluded and there is subsequent evidence of complete vessel healing in keeping with the natural history of SCAD.

Angiographic appearances of SCAD. Adapted from the Saw classification. (A) Type 1 dissection with visible linear ‘flap’ or dual lumen in the mid-left anterior descending coronary artery. (B) Type 2a dissection with a long segment of narrowing in the right coronary artery with no visible ‘flap’ and distal reconstitution of normal vessel architecture. (C) Type 2b dissection with a long segment of narrowing in the distal third of the left anterior descending coronary artery with no visible ‘flap’ and no distal reconstitution. (D) Type 3 dissection in the mid-left anterior descending coronary artery. Angiographically difficult to distinguish from an atherosclerotic stenosis. (E) Type 4 dissection with the appearances of an abrupt vessel occlusion in the apical segment of the left anterior descending coronary artery with subsequent vessel healing and no cardiac embolic source. SCAD, spontaneous coronary artery dissection.
Additional angiographic features
While SCAD has been reported in all coronary segments, it has a frequent predilection for more distal coronary segments (in contrast to atherosclerotic disease).4–7 When it occurs, proximal disease more commonly has a type 1 appearance and may have associated thrombus within the true lumen while middle to distal SCAD is more usually a type 2 appearance. Although more discrete dissected segments do occur, long affected segments are more typical. Most4–6 8 but not all7 series report the left anterior descending to be the the most common affected vessel. Coronary tortuosity is increased with a non-significant trend towards a higher risk of recurrence in those with the greatest tortuosity.26 Simultaneous multivessel SCAD is well recognised.
Vessel healing
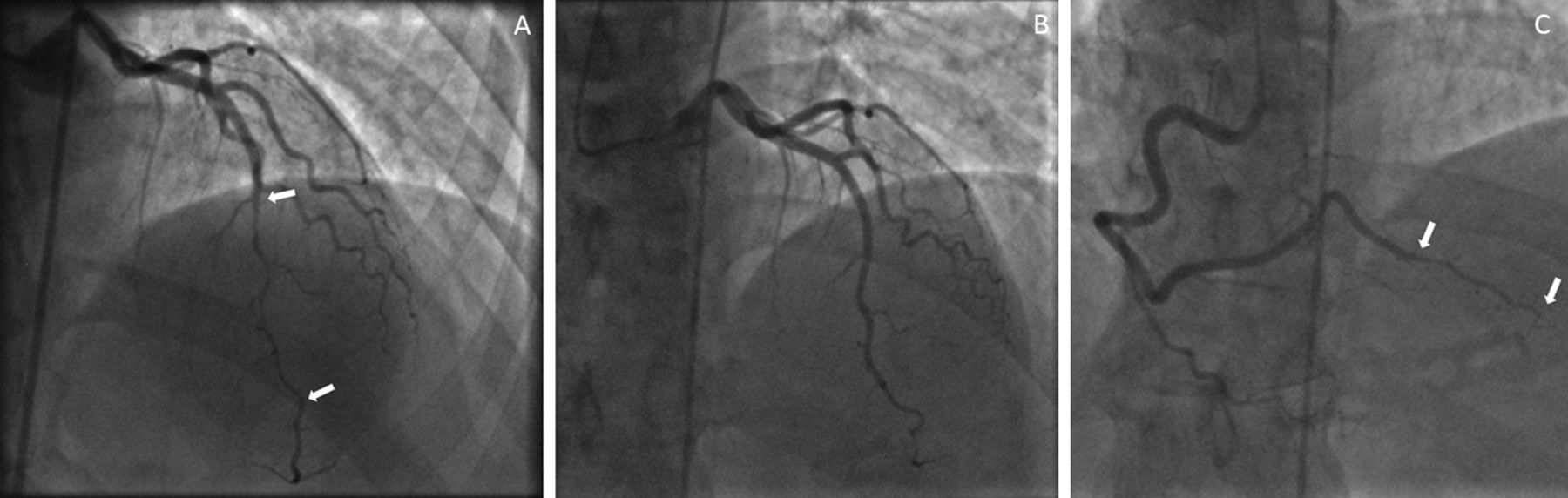
Although there are some reports of persisting dissections or coronary maladaptation following SCAD,4 47 48 complete vessel healing in conservatively managed SCAD seems to occur in the most cases which remain stable during the acute period (figure 3A,B) with normalisation reported to occur in the majority by 26 days.5 7

Conservative management of SCAD. Type 2a SCAD in the left anterior descending coronary artery (A) healed completely at repeat angiography (B) following presentation with a further acute coronary syndrome found to be due to a second type 2b SCAD in the right coronary artery (C). SCAD, spontaneous coronary artery dissection.
Intracoronary imaging
Although the angiographic findings in SCAD may be characteristic, if diagnostic uncertainty remains, intracoronary imaging by intravascular ultrasound (IVUS) or optical coherence tomography (OCT) findings are usually characteristic. OCT has the advantage of higher spatial resolution (15–20 µm) but limited depth penetration, while IVUS has greater depth penetration but limited spatial resolution (150 µm).49 50 Because some important features (true lumen boundaries, fenestrations between true and false lumens and local thrombus) require higher resolution imaging, OCT is preferred for SCAD imaging by some authors.44 A number of clinical issues should however be considered before imaging and/or deciding on the optimal imaging strategy. First, in patients with TIMI 3 flow and in whom the angiographic appearances are typical, there is an inherent risk that any coronary instrumentation of the dissected artery could exacerbate matters and potentially convert a case which could be conservatively managed into one in which intervention becomes necessary. Second, the high-pressure contrast injection required for lumenal blood clearance with OCT could extend the dissection (this is probably most relevant in proximal type I dissections). Finally, given the relatively distal locations of many SCADs especially in type 2B dissections, it may be impossible to image the entire length of the affected segment (5/11 cases in one series)51 and adequate blood clearance for OCT imaging from the true lumen may be challenging. However in expert hands, intracoronary imaging appears both safe and clinically useful.51
The classical OCT imaging findings in SCAD are described51 and shown in figure 4. The imaging catheter is cited in the true lumen with the false lumen, visible as a crescentic arc, separated by the intimal–medial membrane (figure 4A). In some cases, the true lumen may appear ‘free floating’ within the false lumen (figure 4B). Fenestrations connecting false and true lumens may be evident but are not always present (an intimal tear was identified in 7/11 cases in one series)51 (figure 4A,C). Thrombus may be present either in the true or false (figure 4B) lumens. IVUS (figure 4D) may also be used but given the lower spatial resolution, care is required to ensure the intimal–medial membrane is not missed or misinterpreted.52 53

Intracoronary imaging appearances of SCAD. Typical optical coherence tomography image of SCAD with fenestration connecting true and false lumen (arrow) (A). True lumen ‘floating’ within the false lumen with thrombus evident in the false lumen (arrow) (B). Intramural haematoma with no connection between true and false lumen limiting optical penetration but with the outer limit of the false lumen still identifiable (arrows) (C). IVUS image of healing proximal left anterior descending coronary dissection (D). IVUS, intravascular ultrasound; SCAD, spontaneous coronary artery dissection.
Management of SCAD
Revascularisation
Decision-making about revascularisation in acutely presenting SCAD is more complex than for NSTEMI or STEMI of atherosclerotic aetiology for two principal reasons. First, outcomes following revascularisation, whether surgical or by percutaneous coronary intervention (PCI), are less good54 and second, there is a high likelihood of complete healing of the dissection with conservative management. This has led to a growing consensus in favour of conservative therapy where clinically possible (ie, maintained TIMI3 flow and haemodynamic stability) and limiting intervention to what is required to minimise myocardial injury where revascularisation is essential. All series, however, report a small proportion of SCAD cases which progress with conservative management so close observation in the acute phase is necessary.
Percutaneous revascularisation in SCAD
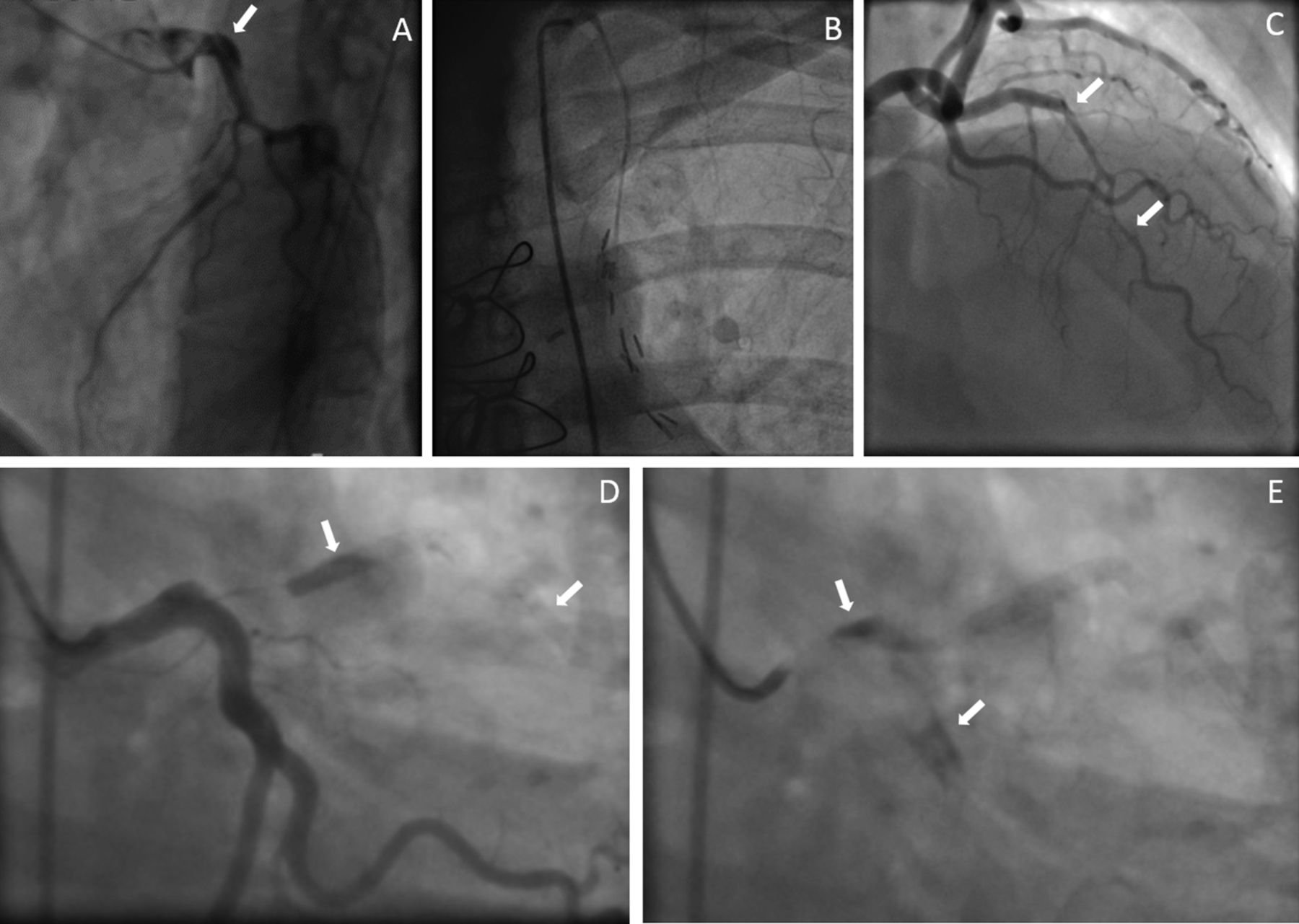
While PCI in SCAD can be very successful and is certainly sometimes essential to restore blood flow in the affected vessel, there are a number of specific technical challenges. The anatomical site and extent of the dissection can be an issue as SCAD often involves longer and relatively distal small calibre coronary segments and with type IIb dissections, there is no clear distal landing zone for a stent. Furthermore, the haematoma in the false lumen behaves very differently from fibroatheromatous plaque material following stent expansion, such that the haematoma frequently tracks proximal and/or distal to the stented segment creating new prestent and/or poststent lumenal restrictions which may require further stents (figure 5C–E).55 The overall result is that patients with SCAD undergoing PCI frequently require long stented segments to effectively restore luminal architecture. In general, where stents are deemed necessary, drug-eluting stents are preferred. Bioabsorbable scaffold use has also been reported and the long-term clinical results in this population are awaited.56 57 Other interventional strategies are also described including limited balloon angioplasty to restore TIMI 3 flow followed by a conservative approach or even use of a cutting balloon to fenestrate the dissection and relieve external compression.58 Where PCI is required, intracoronary imaging may be useful for procedure optimisation.51 There is a report demonstrating late stent strut malapposition following resorption of the false lumen haematoma,59 but there is little current evidence of an increase in stent thrombosis following PCI in SCAD.

Complications of SCAD revascularisation. Left mainstem SCAD (A) treated by CABG with left internal mammary bypass graft to the left anterior descending artery. Follow-up angiography demonstrating a healed dissection and graft failure (B). Type 2a SCAD with TIMI 3 flow in the left anterior descending coronary artery (C). Initial stenting (D—distal arrow) led to proximal migration of the haematoma. An attempt to seal the proximal extent of the dissection with a second stent (D—proximal arrow) led to further proximal extension of the dissection causing occlusion of the left anterior descending coronary artery (D) with dye hang up indicating dissection propagation into the left mainstem and circumflex (E). CABG, coronary artery bypass grafting; SCAD, spontaneous coronary artery dissection.
CABG in SCAD
Emergency CABG is sometimes used as a bail-out strategy in SCAD. Two typical scenarios are either a failure of PCI (usually due to an inability to track the guidewire into the true lumen) or left mainstem or very proximal SCAD where there is felt to be a high degree of jeopardy involved with conservative management or stenting. Although useful in the short term for SCAD limited to the proximal vessel, grafting is unsuitable for distal or extensive dissections. Furthermore in the medium term, graft failure rates are high (only 5 of 16 conduits remained patent at 3.5 years in one series54 as a result of dissection healing in the native coronary leading to competitive flow in the bypass conduit (figure 5A,B).
Medication after SCAD
There are currently no clinical trials to guide optimal medical management following SCAD. However there are a number of special considerations which distinguish the therapeutic approach in SCAD from standard treatment strategies following myocardial infarction.
Antiplatelet therapy
Dual antiplatelet therapy followed by antiplatelet monotherapy are clearly indicated in patients who have undergone PCI with stenting for SCAD in accordance with guidelines.65 However for those without stents, the indication is less clear. Furthermore, women of child-bearing age can develop significant menorrhagia with antiplatelet therapy.66 There is some pathophysiological logic in initiating antiplatelet therapy in the acute phase where intracoronary imaging is reported to show that SCAD can act as a substrate for thrombus formation within the true lumen.51 In conservatively managed SCAD, once healing has been confirmed, the logic of maintaining platelet inhibition for a condition whose primary pathophysiological event is a spontaneous intramural bleed seems less evident, although discontinuing antiplatelet therapy in SCAD remains controversial.
Anticoagulant therapies
The risk/benefit of anticoagulant therapies either acutely (prior to or during coronary angiography, PCI or cardiopulmonary bypass) or chronically is unknown. In general, concerns about dissection expansion/extension in the acute phase and the theoretical increased risk of recurrence should minimise their use. Where strong indications exist however (eg, left ventricular mural thrombus or thromboembolism), a lack of clear evidence of harm probably favours their use with careful monitoring in selected cases.
Statins
Patients with SCAD are frequently commenced on statins as part of the standard evidence and guideline-based cocktail of medications usually initiated following myocardial infarction in patients with atherosclerosis.67 68 However, the logic of prescribing cholesterol lowering agents for a condition which has no known pathophysiological link to cholesterol seems unclear and one study has suggested a link between statins and increased recurrence risk.4
Other postmyocardial infarct medications
Where patients are left with impaired left ventricular function following SCAD, evidence and guideline-based medications (eg, ACE inhibitors, ARBs (angiotensin receptor antagonists), β-blockers, mineralocorticoid receptor antagonists) are recommended.67 68 However, as the SCAD population is generally younger, female and without premorbid hypertension, low blood pressure can be limiting in many patients. In normotensive SCAD survivors with preserved left-ventricular function, a more conservative approach to these medications may be sensible.
ICD/devices/mechanical assist/transplantation
Unfortunately, some patients suffer significant myocardial injury as a result of their SCAD event(s). Extreme cases may present with cardiogenic shock requiring mechanical ventricular assist or even extracorporeal membrane oxygenation as a bridge to transplantation.69 Devices (ICD - implantable cardioverter defibrillator/CRTD - cardiac resynchronisation therapy defibrillator) should be considered in patients with severe impairment of left ventricular function in accordance with guidelines.67 68
Convalescent imaging
Coronary CT
Although CT findings in SCAD have been described,70 the relatively low spatial resolution of CT coupled wtih the distal coronary location of many SCAD sites plus variations in contrast penetration of the false lumen may limit its sensitivity for the primary diagnosis of this condition.71 Where CT may have utility is to non-invasively confirm coronary healing in conservatively managed cases,47 especially given reports of iatrogenic dissections occurring during follow-up angiography.72
Assessment of left ventricular systolic function
As with myocardial infarction of any aetiology, an assessment of left ventricular function in the recovery phase following SCAD is mandatory. Echocardiography or cardiac MRI can be used.71 This is of particular importance as there is some suggestion that recovery of left ventricular function following SCAD myocardial infarction may be better than that following conventional atherosclerotic events,73–75 and this may impact on medical treatment choices.
Peripheral arterial assessment: fibromuscular dysplasia
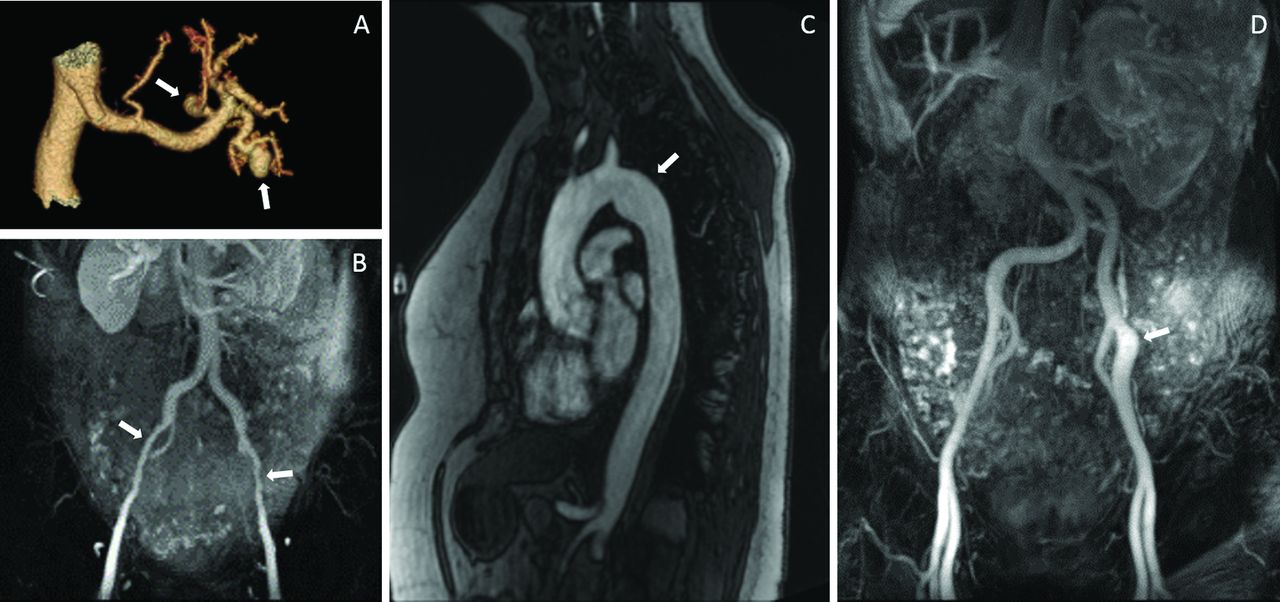
SCAD is frequently a coronary manifestation of a more widespread arteriopathy. Remote dissections and aneurysms have been described with 66% of cases having some extracoronary abnormality in one series (figure 6).76 Fibromuscular dysplasia (FMD) is the the most common remote arteriopathy found in patients with SCAD,77 78 although the reported incidence varies widely (25%–86%).76 79 80 Coronary abnormalities distinct from dissections have been reported in patients with peripheral arterial FMD (including a subgroup with previous SCAD), and it has been suggested that SCAD may be a complication of coronary FMD.81 Although the long-term clinical significance of peripheral arterial FMD in SCAD survivors remains to be determined, an assessment for renal, cervicocephalic and iliac FMD is recommended in all patients with SCAD.78 This can be by CT82 or MRA (magnetic resonance angiography).78 79 CT has the advantage of higher spatial resolution and therefore potentially better sensitivity, while MRA avoids the radiation dose inherent to CT which may be a particular concern in this younger population.78

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Extracoronary manifestations of SCAD. Renal aneurysms (A), Iliofemoral fibromuscular dysplasia (B), a thoracic saccular aneurysm (C) and an iliac saccular aneurysm and gross tortuosity (D) found on screening in SCAD survivors. SCAD, spontaneous coronary artery dissection.
Management after SCAD
Risk of recurrence
Recurrent SCAD is well recognised. Report incidences range from 5% to 19% of cases,4–8 26 although repeat events may be overestimated in registries reliant on self or even clinician referral. Prospective series are underway to assess this further. Recurrent events may occur in the same or a different (figure 3) artery.
Recurrent (including cyclical) chest pain
Many patients continue to experience episodes of significant chest pain long after healing of the primary lesion.83 In some premenopausal cases pains may be cyclical, usually occurring premenstrually. Anecdotally, these chest pains respond to conventional treatments for coronary spasm (ie, cessation of β-blockers and initiation of high-dose vasodilators such as diltiazem). Cyclical cases respond well to implantation of a Mirena (Bayer, Whippany, New Jersey, USA) coil.
Rehabilitation and exercise risk
In general and according to guidelines for patients after myocardial infarction, cardiac rehabilitation and a return to full activity is recommended and has been validated as safe for SCAD survivors.84 85 Isometric or extreme exercise is not recommended.
Contraception after SCAD
The predilection of SCAD for female patients and the association with pregnancy and the peripartum period strongly suggests a role for sex hormones in the pathogenesis. This has led to some concerns over the safety of hormonal contraceptives in women post-SCAD.1 Clearly, barrier methods are safe and an intrauterine contraceptive either hormone free or with local hormone delivery may be useful in some cases (eg, for cyclical chest pain or menorrhagia).
Pregnancy after SCAD
Data from one small series has reported nine pregnancies in SCAD survivors with one recurrence occurring in a patient whose first event was not peripartum.86 The degree of left ventricular impairment post-SCAD will also contribute independently to the risk. Pregnancies which do occur should be deemed high risk and managed by an appropriate multidisciplinary team.
Key messages
Spontaneous coronary artery dissection (SCAD) is an underdiagnosed cause of non-atherosclerotic acute coronary syndromes.
Peripartum cases account for <10% of patients with SCAD.
There is frequently not a visible dissection flap on coronary angiography.
A conservative approach to revascularisation is favoured where possible.
You can get CPD/CME credits for Education in Heart
Education in Heart articles are accredited by both the UK Royal College of Physicians (London) and the European Board for Accreditation in Cardiology—you need to answer the accompanying multiple choice questions (MCQs). To access the questions, click on BMJ Learning: Take this module on BMJ Learning from the content box at the top right and bottom left of the online article. For more information please go to: http://heart.bmj.com/misc/education.dtl
RCP credits: Log your activity in your CPD diary online (http://www.rcplondon.ac.uk/members/CPDdiary/index.asp)—pass mark is 80%.
EBAC credits: Print out and retain the BMJ Learning certificate once you have completed the MCQs—pass mark is 60%. EBAC/ EACCME Credits can now be converted to AMA PRA Category 1 CME Credits and are recognised by all National Accreditation Authorities in Europe (http://www.ebac-cme.org/newsite/?hit=men02).
Please note: The MCQs are hosted on BMJ Learning—the best available learning website for medical professionals from the BMJ Group. If prompted, subscribers must sign into Heart with their journal’s username and password. All users must also complete a one-time registration on BMJ Learning and subsequently log in (with a BMJ Learning username and password) on every visit.
Acknowledgments
The authors acknowledge the contribution of the ESC-ACCA Study Group on Spontaneous Coronary Artery Dissection: Fernando Alfonso (Spain), Angela Maas (The Netherlands), Christiaan Vrints (Belgium), Tom W Johnson and Stephen P Hoole (UK). We are grateful to Gerry McCann for the MRI images and PJ Gallagher for the histopathological image in figure 1.
References
Footnotes
Contributors All authors have contributed to the preparation, refinement and review of the article and are in agreement with its content.
Funding This work is supported by the Department of Cardiovascular Sciences at the University of Leicester, the NIHR Leicester Cardiovascular Biomedical Research Unit, the NIHR rare diseases translational research collaboration and the British Heart Foundation.
Competing interests None declared.
Provenance and peer review Commissioned; externally peer reviewed.
Collaborators The ESC-ACCA Spontaneous Coronary Artery Dissection Study Group: Fernando Alfonso, Angela Maas, Christiaan Vrints, Tom W Johnson, Stephen P Hoole, Nilesh J Samani, Gerry P McCann.