Article Text

Statistics from Altmetric.com
- DSE, dobutamine stress echocardiography
- EDWT, end diastolic wall thickness
- FDG, F18-fluorodeoxyglucose
- LV, left ventricular
- LVEF, left ventricular ejection fraction
- MRI, magnetic resonance imaging
- NYHA, New York Heart Association
- PET, positron emission tomography
- SI, signal intensity
- SPECT, single photon emission computed tomography
- SWT, systolic wall thickening
Over the past decade the number of patients presenting with heart failure has increased exponentially.1 It has been estimated that 4.7 million patients in the USA have chronic heart failure, with 400 000 new cases per year, resulting in one million hospitalisations.1 The diagnostic and therapeutic costs involved with heart failure are estimated to be more than $11 billion per year.1 Gheorghiade and Bonow emphasised that the aetiology of heart failure may be coronary artery disease in > 70% of patients.2
Currently, three routine courses of action are available: medical treatment, heart transplantation, and revascularisation. Newer therapeutic modalities include laser therapy, advanced surgery, assist devices, artificial hearts,3 and transplantation of different (progenitor) cells.4 These options should currently be considered experimental but may offer alternative treatments in the future. Medical treatment has improved substantially over the past years, with the introduction of angiotensin converting enzyme (ACE) inhibitors, angiotensin II receptor blockers, and spironolactone. Four recent trials have demonstrated the value of β adrenergic blocking agents in the treatment of patients with heart failure.5 Finally, amiodarone has been demonstrated to reduce sudden death in patients with heart failure.6 Despite all of these new drugs, mortality of patients with severe heart failure remains high; Cowie and colleagues7 reported 12 month mortality to be 38% and extrapolation of these results demonstrated five year mortality to be > 70%.
The second option, heart transplantation, has fairly good long term prognosis but the limited number of donor hearts is largely exceeded by demand.8 In addition, many patients with heart failure have significant co-morbidities, excluding them as candidates for heart transplantation.
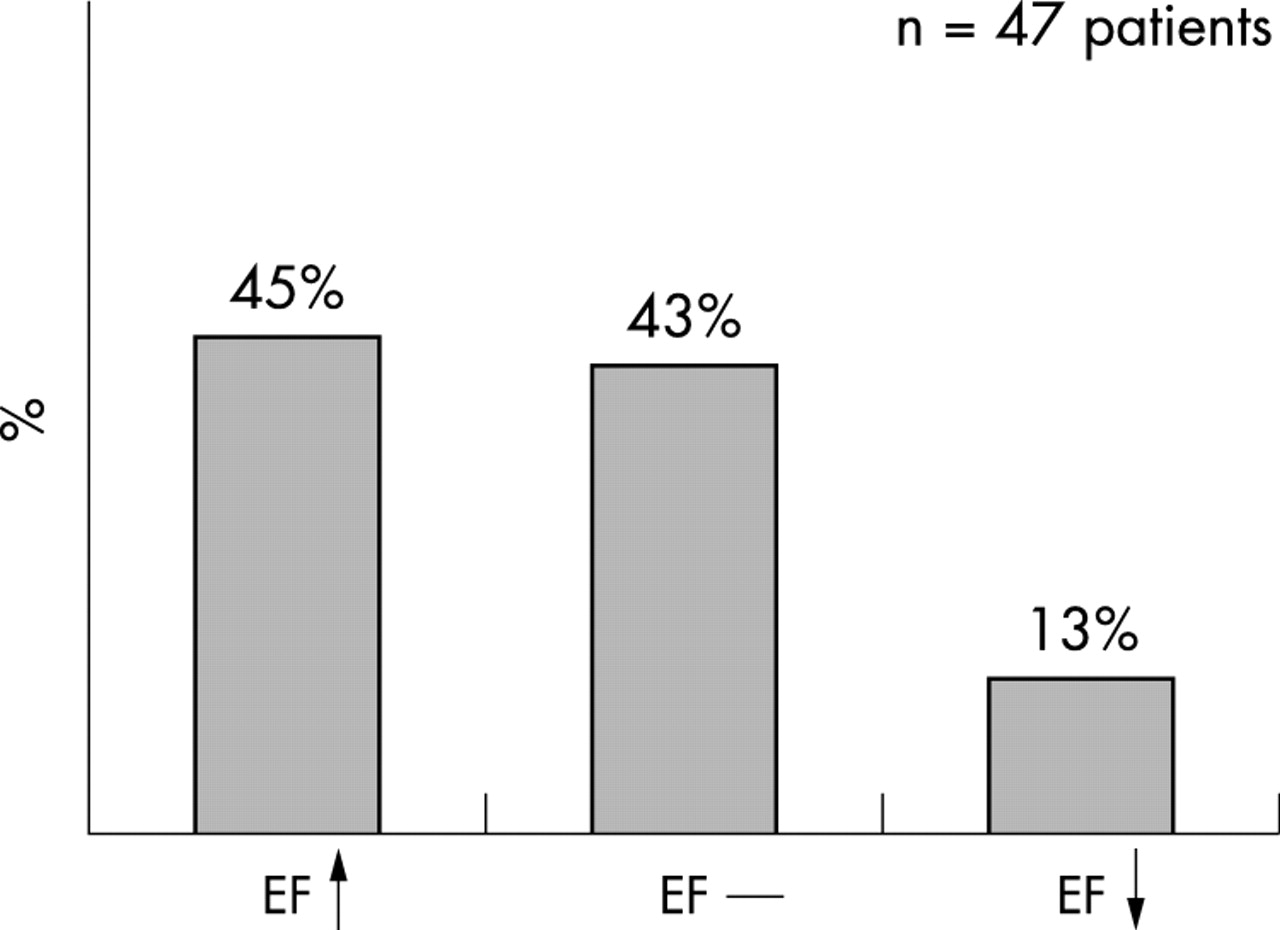
Revascularisation is the third option in patients with heart failure. The major drawback to performing revascularisation in these patients is the high periprocedural morbidity and mortality.9 However, it has been shown that there is a substantial survival benefit after surgical revascularisation compared with medical treatment.10 Also, improvement in regional contractile function and left ventricular ejection fraction (LVEF) was shown following revascularisation.11 Since LVEF is an important prognostic parameter,12 improvement in LVEF may, at least in part, contribute to improved survival. However, contractile function does not improve in all segments and not all patients improve in LVEF. In our own experience, improvement in contractile function is seen in approximately one third of segments and approximately 40% of patients have improvement in LVEF (fig 1).13 Hence, identification of patients with the potential for improvement in LVEF and survival is needed to justify the higher risk of surgery in these patients.
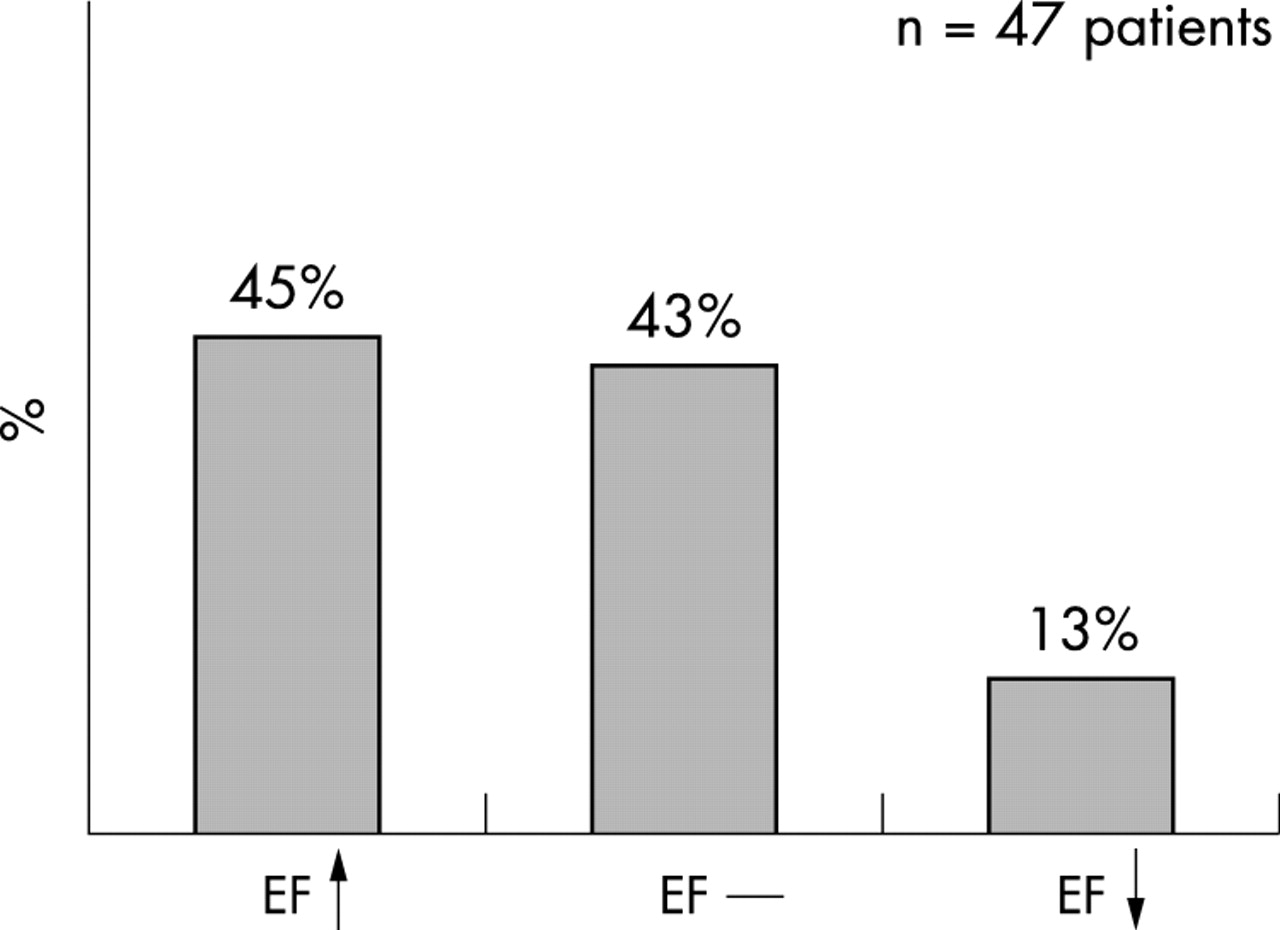
Changes in left ventricular ejection fraction (LVEF), observed in 47 patients with ischaemic cardiomyopathy undergoing revascularisation. Improvement in LVEF was defined as an increase in LVEF of ⩾ 5% after revascularisation. (Data based on Bax and colleagues.13)
DEFINITIONS OF MYOCARDIAL VIABILITY
Initially, it was thought that dysfunctional myocardium, related to coronary artery disease, was equivalent to myocardial necrosis. However, the observational studies by Rahimtoola14 indicated that many patients with left ventricular (LV) dysfunction exhibited improvement of function after revascularisation. To explain the improvement in function, the concept of viability was introduced: dysfunctional but viable myocardium has the potential to recover function after revascularisation, whereas the revascularisation of scar tissue will not result in improvement of function. Histological analysis of biopsies obtained during revascularisation confirmed that segments with recovery post-revascularisation contained viable myocytes as compared to the large extent of fibrosis detected in irreversibly damaged myocardium.15
In the literature different definitions of viable myocardium have been used. Hibernation refers to a condition of chronic sustained abnormal contraction caused by chronic underperfusion in patients with coronary artery disease in whom revascularisation causes recovery of function.14 Several studies have demonstrated a significant reduction in resting blood flow in segments that exhibited improvement of function after revascularisation. Tawakol and colleagues using N13-ammonia positron emission tomography (PET) showed that mean (SD) blood flow in normally contracting myocardium was 1.14 (0.52) ml/min/g, as compared to 0.48 (0.15) ml/min/g in dysfunctional but viable myocardium.16 Sun et al showed that blood flow was also reduced in viable myocardium, but to a lesser extent than shown by Tawakol et al.16,17 In contrast, other studies have demonstrated that resting perfusion was near normal in chronic dysfunctional myocardium.18,19 Vanoverschelde et al observed almost similar levels of perfusion in regions with normal contraction and regions with chronic dysfunction: 85 (14) ml/min/100 g v 77(25) ml/min/100 g.18 These authors showed that instead of resting flow, flow reserve was reduced in dysfunctional but viable myocardium.18 Based on their observations, Vanoverschelde and co-workers18 suggested that repeated ischaemic attacks may result in chronic dysfunction, with flow remaining normal or mildly reduced—a condition referred to as repetitive stunning.20
Observations in animal models of chronic occlusion resulting in chronic contractile dysfunction suggest that a temporal progression of initially near normal flow (with reduced flow reserve) to reduced resting flow may occur. Firoozan et al21 have developed a six week model of hibernation in dogs using ameroid constrictors on proximal left coronary arteries. Initially, flow remained near normal (consistent with stunning), but later some dysfunctional segments developed a reduction in resting flow. Fallavolita and Canty22,23 have shown that in a pig model of chronic hibernation, dysfunctional myocardium flow was normal at 1–2 months but was reduced at 3–4 months. Thus, the conflicting findings in patients may result from different durations of chronic dysfunction, and repetitive stunning and hibernation may represent different ends of the spectrum of chronic dysfunction. However, from a clinical point of view this differentiation may not be that important, since both repetitively stunned and hibernation myocardia need to be revascularised in order to improve function.
Finally, chronic dysfunction can also result from non-transmural necrosis in combination with viable (normal) myocardia. The subendocardial layer contributes significantly to contraction and subendocardial necrosis of > 20% of the myocardial wall results frequently in akinesia.24 Revascularisation of these regions will not improve contractile function, but may be of clinical relevance in terms of preventing remodelling.25
CLINICAL RELEVANCE OF MYOCARDIAL VIABILITY
Although from a theoretical point of view, the assessment of viability in patients may be of interest, the key question is how frequently is viable myocardium present in chronic dysfunctional myocardium? Various studies have reported on the incidence of viability in patients with chronic ischaemic LV dysfunction (table 1), with varying results, although studies in larger groups of patients suggest that 50% of the patients exhibit substantial viability.
Incidence of viable myocardium in patients with ischaemic left ventricular dysfunction
Improvement of function after revascularisation is still considered the gold standard for viability. Pooled data from 105 viability studies, with 3003 patients, included 15 045 dysfunctional segments, with 7941 segments (53%) improving in function after revascularisation.26 Clinically, improvement in global LV function (LVEF) may be more important than improvement in regional function. The majority of viability studies have only evaluated improvement of regional LV function but the studies that included assessment of LVEF, before and after revascularisation, consistently showed that patients with a substantial amount of viable tissue improved in LVEF after revascularisation. It is currently unclear whether an improvement in LVEF is strictly necessary to result in an improved prognosis. Samady et al27 recently evaluated 135 patients with ischaemic cardiomyopathy (LVEF ⩽ 30%) undergoing revascularisation and 68 (65%) patients showed an improvement of 5% or more in LVEF. Survival at 32 (23) months was comparable between patients with and without improvement in LVEF. However, viability testing was not part of the routine work-up of these patients and improvement in LVEF was assessed within six weeks of revascularisation, which is too short a time to exclude improvement in LVEF, since recovery of function may occur up to one year after revascularisation.28 Still, it is important to realise that besides improvement in LVEF, revascularisation of viable myocardium may have a beneficial effect on the prevention of remodelling, arrhythmias, and sudden cardiac death, which may also improve longevity.25
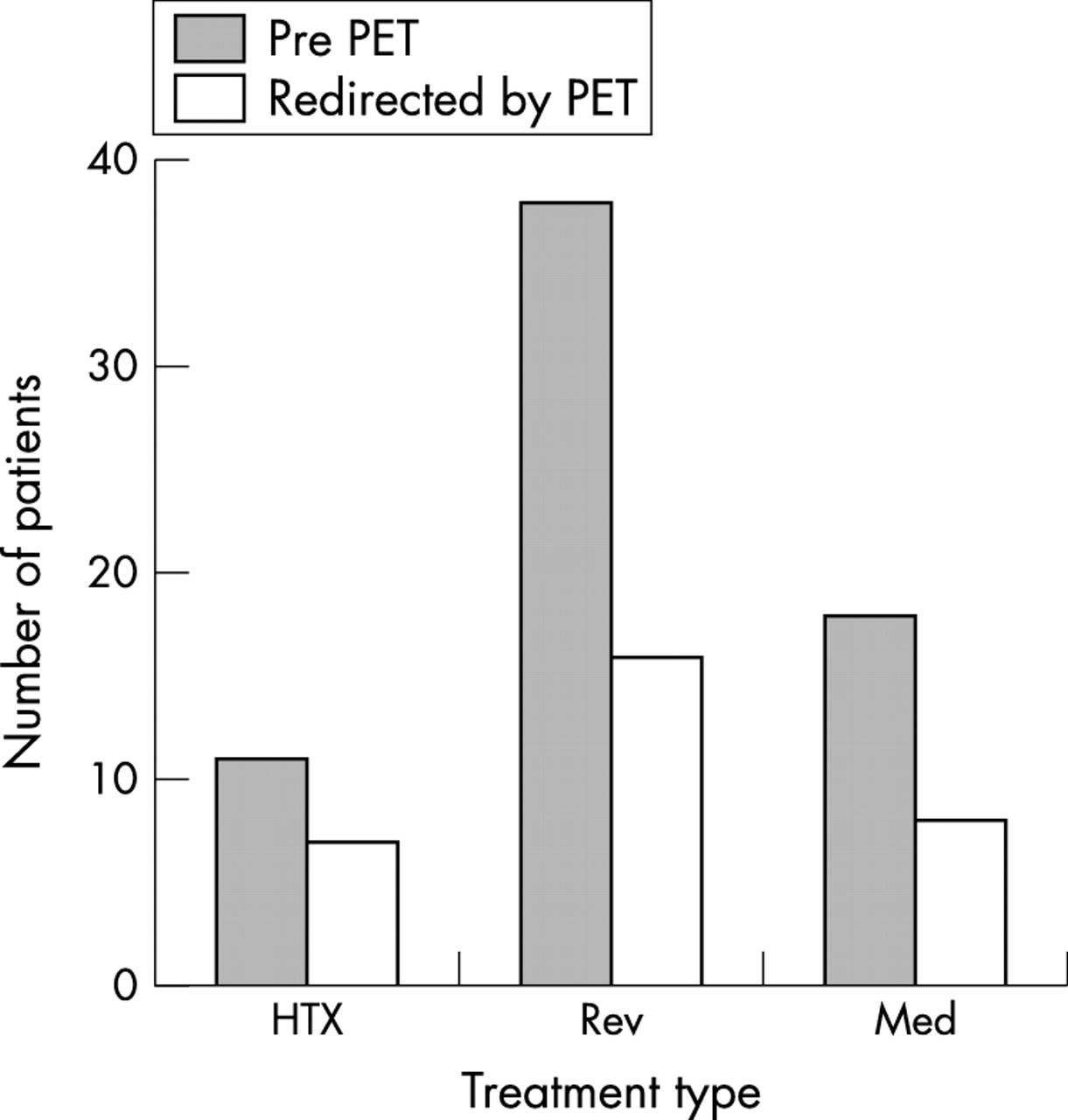
Finally, Beanlands and colleagues29 have demonstrated the impact of viability assessment on subsequent management of patients with ischaemic LV dysfunction. The authors evaluated 67 patients with F18-fluorodeoxyglucose (FDG) PET, while treatment was already established on clinical information. Thus, 11 patients were scheduled for heart transplantation, 38 for revascularisation, and 18 for medical treatment. Based on the presence/absence of viability, treatment was changed in 31 (46%) patients (fig 2). In addition, the same group demonstrated that once viability has been detected, revascularisation should follow as soon as possible.30 The authors evaluated 35 patients with FDG PET; 18 patients underwent early revascularisation (12 (9) days after FDG PET) and 17 underwent late revascularisation (145 (97) days after FDG PET). In the early revascularisation group, the preoperative mortality was lower, more patients improved in LVEF postoperatively, and the event-free survival was higher. All these findings support the necessity and clinical relevance of viability assessment in patients with ischaemic cardiomyopathy.

Bar graph illustrating the influence of FDG PET imaging on subsequent patient management. The grey bars indicate the number of patients and their planned treatment before FDG PET was performed; the white bars demonstrate the number of patients in whom treatment was changed according to the FDG PET results. HTX, heart transplantation; Med, medical treatment; Rev, revascularisation. (Reprinted from Bax and colleagues,44 with permission).
CHARACTERISTICS OF VIABLE MYOCARDIUM
Dysfunctional but viable myocardium has different characteristics and these form the basis for the different imaging modalities that are most frequently used for the assessment of myocardial viability (table 2). These characteristics include intact perfusion, cell membrane integrity, intact mitochondria, preserved glucose and (possibly) fatty acid metabolism, and contractile reserve.31 All these characteristics can be evaluated by scintigraphic techniques using PET or single photon emission computed tomography (SPECT) (table 2). Perfusion can be evaluated by thallium-201 or technetium-99m labelled tracers, cell membrane integrity can be evaluated by thallium-201, intact mitochondria can be probed by technetium-99m labelled tracers, and preserved glucose and free fatty acid metabolism can be assessed by FDG and radiolabelled fatty acids (123I-β methyliodophenyl pentadecanoic acid (BMIPP) is most frequently used). Contractile reserve is evaluated most frequently by echocardiography, or more recently by magnetic resonance imaging (MRI), using dobutamine stress. However, various studies have recently demonstrated the feasibility of evaluating contractile reserve by gated SPECT (using technetium-99m labelled agents) during the infusion of dobutamine.32
Characteristics of dysfunctional but viable myocardium
Not all viable myocytes exhibit all characteristics. Sloof and co-workers33 have recently studied 14 patients with chronic ischaemic LV dysfunction and evaluated perfusion by early resting thallium-201 SPECT, fatty acid utilisation by BMIPP SPECT, glucose utilisation by FDG SPECT, and contractile reserve by dobutamine stress echocardiography (DSE). Intact perfusion was found in 52% of dysfunctional segments, fatty acid utilisation was maintained in 59% of segments, glucose utilisation was preserved in 59% segments, whereas contractile reserve was present in significantly fewer segments (33%, p < 0.01 v perfusion, glucose and fatty acid utilisation) (fig 3). Other recent studies have demonstrated that segments with preserved thallium-201 uptake, but without contractile reserve, have significantly more fibrosis.34,35 Thus, the presence or absence of the different characteristics may be related to the severity of ultrastructural damage at the myocyte level.35

Bar graphs indicating the discrepancy between contractile reserve (assessed by DSE) and different nuclear imaging techniques. CR+, contractile reserve present; CR−, contractile reserve absent; DSE, dobutamine stress echocardiography; FDG, F18-fluorodeoxyglucose; FFA, free fatty acids. (Based on Sloof and colleagues.33)
IMAGING TECHNIQUES
Thallium-201 SPECT
The initial uptake of thallium-201 after injection is mainly determined by regional perfusion, whereas sustained uptake (usually imaged at 3–4 hours after injection) is dependent on cell membrane integrity which reflects viability.36 Although many thallium-201 imaging protocols have been described, only two protocols are used frequently in the clinical setting: rest-redistribution and stress-redistribution-reinjection imaging.36
Rest-redistribution provides information on viability only, whereas the reinjection protocol provides information on both viability and stress induced ischaemia. With rest-redistribution imaging, two sets of images are acquired: the first set of images, which are obtained directly following tracer injection, represent perfusion; and the second set of images, obtained 3–4 hours after tracer injection, represent viability. With the stress-redistribution-reinjection protocol, the initial images are obtained after stress, the second set of images are obtained 3–4 hours thereafter (redistribution images); a second dose of thallium-201 chloride is injected and one hour after this reinjection more images are acquired. The stress and redistribution images represent ischaemia and the reinjection images provide information on viability.
Markers of viability on thallium-201 studies are: (1) normal thallium-201 uptake (normal perfusion) at stress; (2) stress defects with redistribution (reversible defects) on the 3–4 hour delayed images; (3) redistribution in fixed defects at redistribution following reinjection or delayed rest images (frequently a threshold of 10% increase in tracer uptake is used); (4) tracer uptake of > 50% at the redistribution-reinjection images or the delayed rest images.36 The first three markers appear to reflect adequately jeopardised but viable myocardium, whereas the fourth marker is more complex. Frequently, segments with > 50% tracer uptake do not improve in function; the reason for this observation is the presence of non-transmural infarction, rather than jeopardised, viable myocardium. These segments are not capable of improving function post-revascularisation, resulting in a lower specificity to predict improvement of function after revascularisation. Still, the higher the level of thallium-201 uptake, the higher the likelihood of recovery of function post-revascularisation, indicating that the amount of viable tissue also determines potential functional recovery.37
The uptake and retention of these tracers is dependent on perfusion, cell membrane integrity, and mitochondrial function (membrane potential).38 Most studies for assessment of viability with have been performed with technetium-99m sestamibi, but recent studies with technetium-99m tetrofosmin have shown a comparable value of this tracer for the assessment of viability.39,40
Most frequently, technetium-99m labelled tracers are injected under resting conditions.38 In these studies, dysfunctional segments with tracer uptake > 50–60% are considered viable.38 Since attenuation may result in lower activities, in particular in the inferior and septal wall, Schneider and colleagues41 have suggested to use a cut-off value of 35% tracer uptake in these regions. Sciagra and co-workers42 have popularised the use of technetium-99m sestamibi imaging after administration of nitrates, either orally or intravenously. It is thought that nitrates enhance blood flow and tracer uptake to myocardial regions that are subtended by severely stenosed arteries. In most of these studies, two sets of images are obtained, a resting image and a nitrate-enhanced image, and these results are compared.
Finally, ECG gating of images provides additional information on function and may potentially enhance accuracy to detect viable myocardium.43
FDG is a glucose analogue (one hydroxyl group replaced by an F18 atom) and initial trans-sarcolemmal uptake is identical to that of glucose. After phosphorylation, FDG-6-PO4 remains trapped in the myocyte (physical half-life 110 minutes) and provides a strong signal for imaging.44 With FDG imaging, the metabolic circumstances determine tracer uptake 45; optimal studies are performed during hyperinsulinaemic euglycaemia, but for clinical routine oral glucose loading is frequently used.45 For optimal identification of viable tissue, FDG imaging should be combined with perfusion imaging. Dysfunctional segments with preserved perfusion and FDG uptake are thought to represent repetitively stunned myocardium and segments with reduced perfusion, but preserved FDG uptake (perfusion-FDG mismatch) are considered hibernating myocardium.44 In contrast, segments with reduced perfusion and concordantly reduced FDG uptake are considered scar tissue.
Since FDG is a positron emitter, FDG imaging is performed with PET; PET has limited availability for clinical routine, however. Driven by the increasing demand for viability studies, much effort has been invested in the development of 511 keV collimators to permit FDG imaging with SPECT.44 Direct comparisons between FDG PET and SPECT have demonstrated excellent agreement.44,46 More recently, gamma cameras with the option of coincidence imaging have been developed; this approach enhances resolution of the system, but necessitates the use of attenuation correction.44
The observation that infusion of dobutamine (5–10 μg/kg/min) can increase contractility in dysfunctional myocardium serves as the hallmark for viable myocardium and has been referred to as contractile reserve. More recent studies have extended the dobutamine infusion to a maximum of 40 μg/kg/min, with the potential addition of atropine.47 This protocol allows assessment of viability at low dose dobutamine infusion with assessment of ischaemia at infusion of higher doses. Four patterns in regions with contractile dysfunction can be observed: (1) biphasic response—initial improvement followed by worsening of wall motion; (2) worsening—direct deterioration of wall motion without initial improvement; (3) sustained improvement—improvement of wall motion without subsequent deterioration; (4) no change—no change in wall motion during the entire study. All patterns except no change, which represents scar tissue, are related to the presence of viable myocardium. Sustained improvement is most likely related to subendocardial necrosis.48
The first MRI studies for the detection of viable tissue focused on the end diastolic wall thickness (EDWT), systolic wall thickening (SWT), and signal intensity (SI) without contrast enhancement.49 Early observations revealed severely reduced EDWT, reduced/absent SWT, and decreased SI in patients with previous infarction.49 In a direct comparison between FDG PET and resting MRI, Baer and colleagues50 showed that segments without SWT and EDWT of < 5.5 mm were non-viable. In a subsequent study, the authors showed that segments with an EDWT of < 5.5 mm never showed recovery of function post-revascularisation.51
The alternative was not true—segments with an EDWT of ⩾ 5.5 mm did not always improve in function post-revascularisation;51 this is not surprising, since many segments with EDWT of ⩾ 5.5 mm contain some extent of subendocardial scar. However, segments that displayed contractile reserve during dobutamine infusion had a high likelihood of recovery.51
The most recent studies have used contrast agents; Kim and colleagues52 have demonstrated the use of contrast enhanced MRI for the detection of viability and subsequent prediction of improvement of function. This technique is primarily based on the detection of scar tissue and the resolution of MRI allows assessment of the extent of transmurality. Kim and co-workers52 demonstrated that myocardium with large areas of hyperenhancement, indicating transmural necrosis, virtually never improved in function after revascularisation, whereas segments without hyperenhancement had a high likelihood of recovery. Problems again arise in the segments with intermediate extents of hyperenhancement, which have a 50% likelihood of recovery. In these segments, an additional test—for example, the assessment of contractile reserve with a dobutamine challenge—is needed to predict recovery after revascularisation.
PREDICTION OF IMPROVEMENT OF FUNCTION AFTER REVASCULARISATION
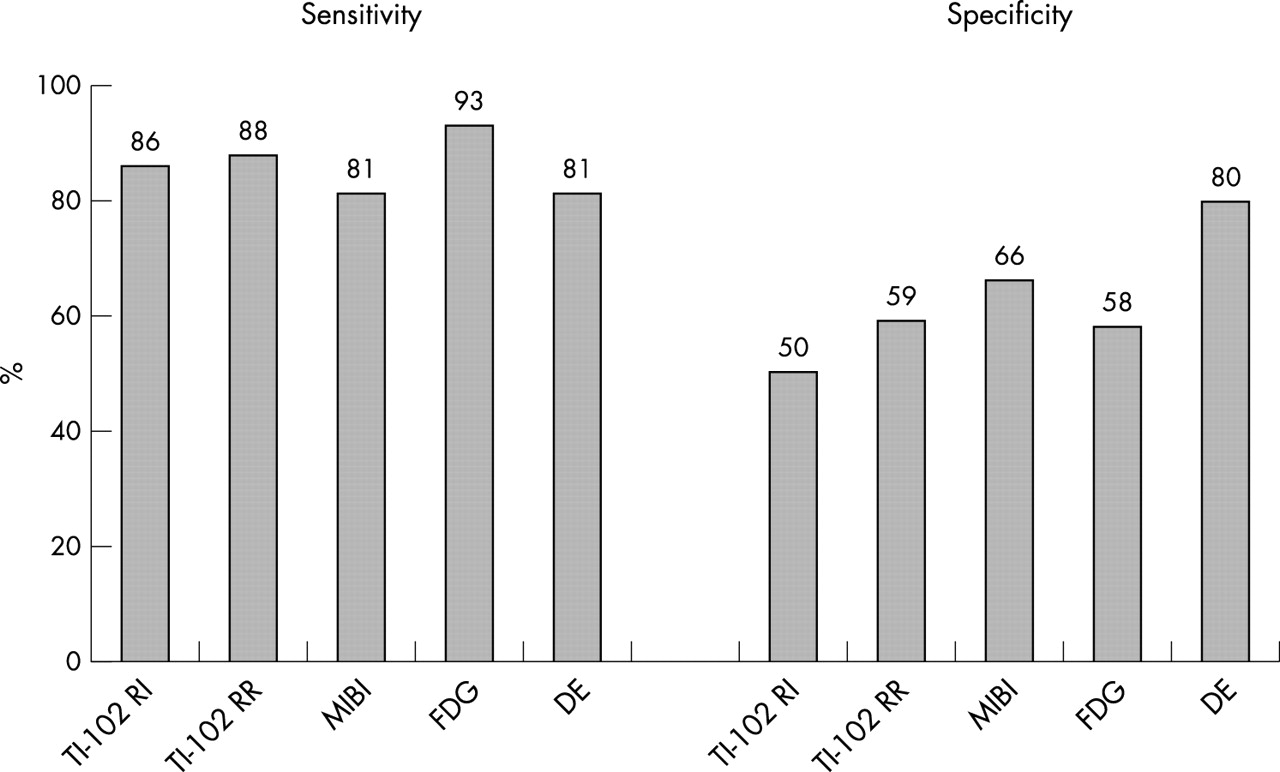
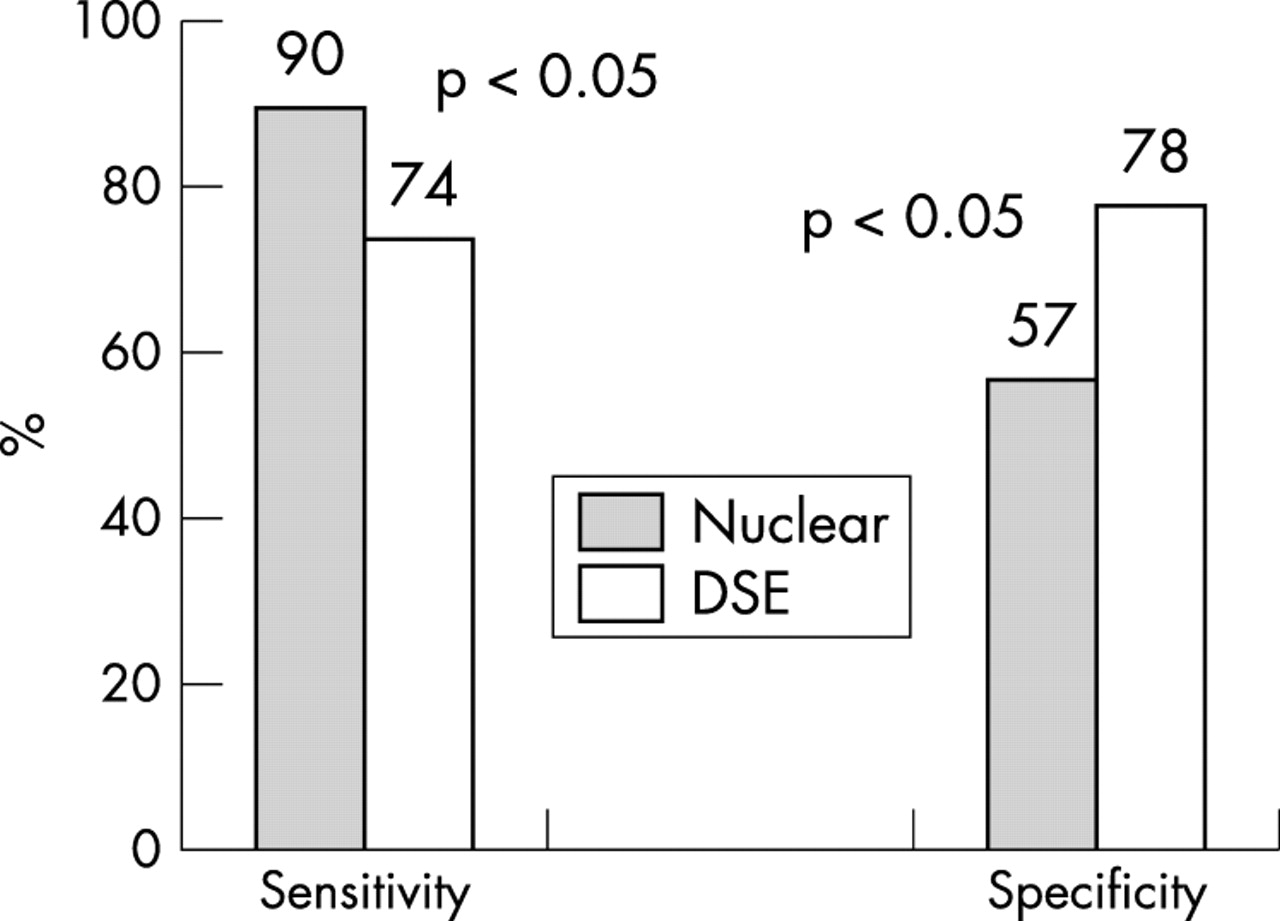
Most of the viability studies have focused on the prediction of improvement of regional function after revascularisation.26 Pooling of all available data (n = 105 studies, n = 3034 patients), resulted in a sensitivity of 84% and a specificity of 69%.26 The relative merits of the techniques for prediction of functional recovery are summarised in fig 4. The nuclear imaging tests tended to have a somewhat higher sensitivity for the prediction of recovery post-revascularisation, whereas DSE had a higher specificity. This discrepancy was even more obvious when the analysis was restricted to 11 studies which compared these two modalities directly (fig 5). The lower specificity of nuclear imaging is caused by dysfunctional segments, which are classified as viable using nuclear imaging, not improving in function. Most of the studies, however, have a limited follow up with a maximum of 3–6 months post-revascularisation.26 Recent data have demonstrated that improvement of function may occur up to one year post-revascularisation.28 Furthermore, these data suggested that more severely damaged myocardium may need longer time to recover function as compared to mildly damaged myocardium. It is conceivable that more severely damaged myocardium may no longer exhibit contractile reserve, but may still have preserved perfusion, cell membrane integrity or glucose utilisation, all characteristics identified by nuclear imaging.53 More studies are needed to confirm these findings.

Sensitivity and specificity of the various viability techniques to predict improvement of regional left ventricular function after revascularisation. DSE, dobutamine stress echocardiography; FDG, F18-fluorodeoxyglucose; MIBI, sestamibi; Tl-201 RI, thallium-201 reinjection; Tl-201 RR, thallium-201 rest-redistribution. (Data based on Bax and colleagues.26)

Sensitivity and specificity of dobutamine stress echocardiography (DSE) and nuclear imaging (Nuclear) techniques (based on pooled data from 11 studies (n = 325 patients) that performed a direct comparison between DSE and nuclear imaging to predict improvement in regional LV function after revascularisation). The sensitivity of the nuclear techniques was significantly higher as compared to DSE, whereas the specificity of DSE was significantly higher. (Data based on Bax and colleagues.26)
From a clinical point of view, improvement of global function is more important than improvement of regional function. A total of 29 studies, with 758 patients evaluated LVEF before and after revascularisation, in relation to presence/absence of viability. The results of these studies are summarised in table 3; the studies consistently showed improvement in LVEF in viable patients. An open question is the exact amount of viable myocardium that is needed to result in an improvement of LVEF post-revascularisation. Various studies have demonstrated that 25–30% of the dysfunctional myocardium needs to be viable to result in improvement of LVEF.54,55
Pooled data from viability studies predicting improvement of LVEF after revascularisation
IMPROVEMENT IN SYMPTOMS, EXERCISE CAPACITY, AND PREVENTION OF REMODELING
Additional end points besides improvement in function have been considered. Few studies have evaluated the relation between preoperative viability and postoperative improvement in symptoms and exercise capacity. Thus far, several viability studies (evaluating New York Heart Association (NYHA) functional class before and after revascularisation) have shown that mean NYHA class improved significantly in patients with viable myocardium.13,44 Individual data, however, varied significantly and the accurate prediction of improvement of symptoms in an individual patient remains difficult.56 Few studies have demonstrated that exercise capacity improved in patients with viable myocardium.57–59 Marwick and colleagues57 evaluated 23 patients with FDG PET before revascularisation and demonstrated that patients with extensive viability improved significantly in exercise capacity post-revascularisation (from 5.6 (2.7) METS to 7.5 (1.7) METS). Similar results were reported by DiCarli et al58 and Gunning et al.59
In addition, the relation between preoperative assessment of viability and prevention of remodelling has been studied recently. Mule and co-workers60 evaluated 50 patients with ischaemic cardiomyopathy with thallium-201 stress-redistribution-reinjection SPECT before revascularisation. Patients with residual viability/ischaemia (involving > 20% of the LV) improved in LVEF (from 35 (6%) to 43 (6%), p < 0.001) and actually demonstrated reversed remodelling after revascularisation, LV end systolic volume index decreased from 68 (16) ml/m2 to 52 (14) ml/m2 (p < 0.001), and the LV end diastolic volume index decreased from 103 (21) ml/m2 to 91 (18) ml/m2 (p < 0.001). These patients also improved in NYHA class and exhibited excellent long term survival (100%). In contrast, patients with predominantly scar tissue failed to improve in LVEF (34 (4%) v 33 (7%), not significant), and exhibited ongoing remodelling (LV end systolic volume index increased from 70 (14) ml/m2 to 78 (23) ml/m2, p < 0.001, and LV end diastolic volume index increased from 106 (19) ml/m2 to 116 (25) ml/m2, p < 0.001), without improvement in NYHA class and worse long term prognosis (29% event rate).
PREDICTION OF LONG TERM PROGNOSIS
The most important clinical issue is the prediction of long term survival. Various studies have evaluated long term prognosis in relation to treatment and viability; in these studies, the patients were grouped according to the presence/absence of viable tissue and treatment (medical versus revascularisation). Currently, 17 prognostic studies are available (seven employing FDG PET, four employing thallium-201 imaging, and six employing DSE).47,48,61–75 The results of these studies are summarised in fig 6.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
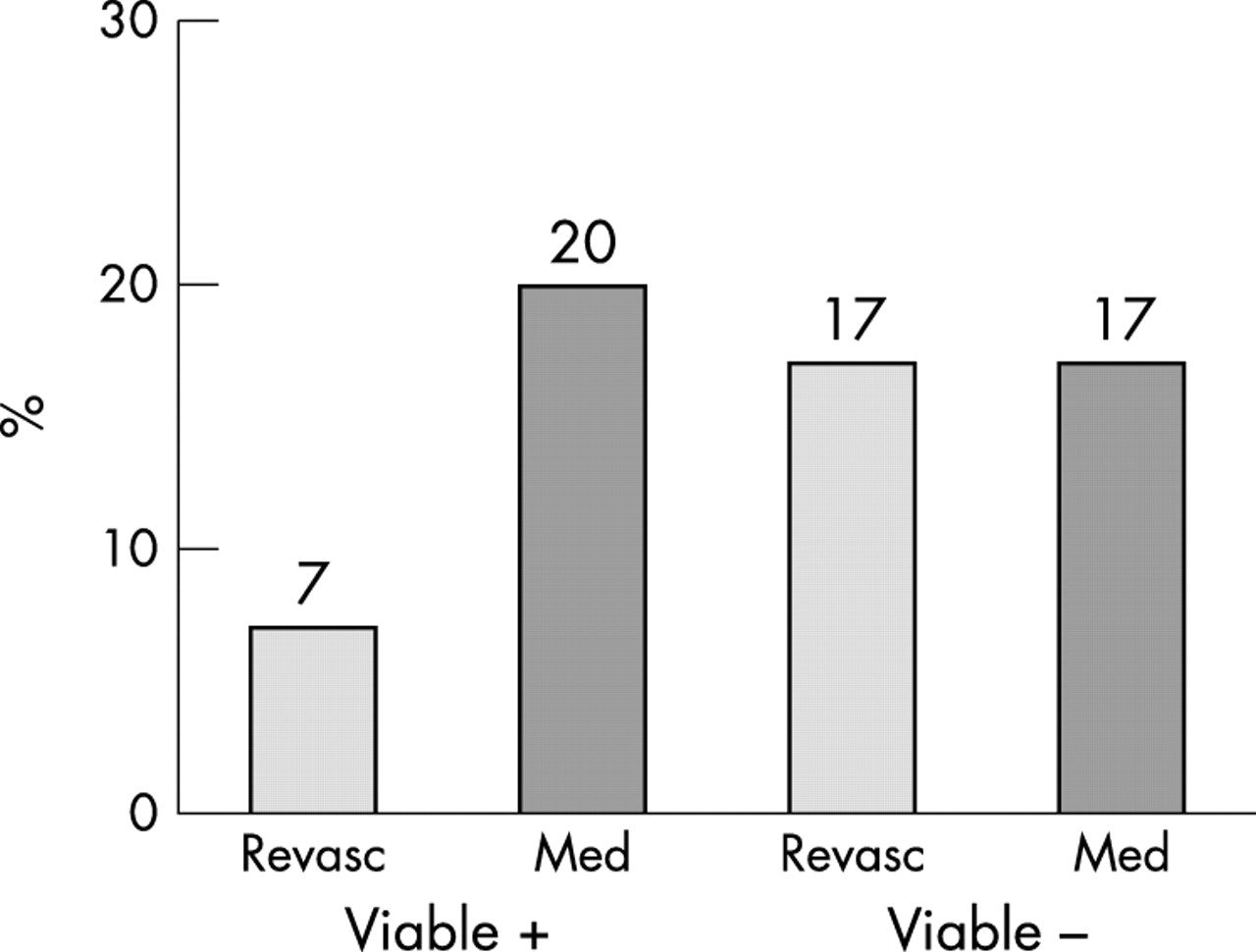
Prognostic value of the viability studies: event rate is plotted versus presence/absence of viability and treatment (medical/revascularisation). The highest mortality is observed in the patients with viable myocardium who were treated medically. Med: medical treatment; Revasc: revascularisation. (Based on pooled data from references 47, 48, 61–75.)
A high mortality rate was observed in all groups, except in the group of patients with viable myocardium who underwent revascularisation. Thus, the combination of viability and revascularisation appears to favourably influence long term survival. However, all of these studies were non-randomised, retrospective analyses and the findings need to be confirmed in a randomised, prospective trial. This trial is now underway: the surgical therapy for ischemic congestive heart failure (STICH) trial is a randomised, prospective trial evaluating the role of viability (versus therapy) for predicting long term outcome.76 Another comparable trial is currently being conducted in the UK (Heart-UK study).
CONCLUSIONS
Heart failure secondary to chronic coronary artery disease is a major problem in clinical cardiology. In patients with viable myocardium, revascularisation is likely to result in improvement of regional and global LV function, heart failure symptoms, and long term prognosis. Alternatively, current evidence suggests that patients with viable myocardium who are treated medically have a high event rate. Thus, assessment of viability in patients with ischaemic cardiomyopathy may help to guide optimal treatment. Accordingly, patients with severely depressed LVEF (< 35%), secondary to chronic coronary artery disease without a recent (< 1 month) myocardial infarction, and presenting with heart failure are the candidates that should undergo additional viability testing. Patients with accompanying angina or who have a preserved LVEF should not be referred routinely for viability testing. In addition, the precise role of viability assessment in patients with an acute myocardial infarction is currently unknown.
Several viability tests are available: SPECT imaging with thallium-201 or a technetium-99m labelled agent may be the first step; these techniques are very sensitive for detecting viable myocardium, and relatively widely available. DSE may also be a good initial test, although one should keep in mind the somewhat lower sensitivity of this technique.
Contrast enhanced MRI is a promising technique, but larger studies are needed to determine the precise value of the technique. In patients with the most severely depressed LVEF, FDG imaging may be the technique of choice, since this technique has the highest sensitivity, allows attenuation correction, and has superior resolution to SPECT.
Although a lot of information on assessing viability in chronic ischaemic heart disease has been obtained over the past decade, prospective, randomised trials, comparing medical treatment versus revascularisation, and focusing on prognosis are still missing. Therefore, the results of the STICH trial and the Heart-UK study are needed.