Article Text

Statistics from Altmetric.com
Intravascular ultrasound shows that many coronary artery atherosclerotic plaques do not encroach on the lumen and therefore are angiographically invisible.1 ,2 The reason for this phenomenon was first firmly established in human coronary arteries by Glagov and colleagues.3 As a plaque develops the overall cross sectional area of the coronary artery increases to accommodate the plaque without any reduction in the cross sectional area of the lumen. The process was termed compensatory enlargement. The increase in total cross sectional area of the artery is achieved by two mechanisms. One has been recognised by pathologists for many years4and involves the media behind the plaque undergoing atrophy with fracture of the internal elastic lamina. The plaque is extruded outward through the disrupted media leaving the lumen normal in shape and size but giving the artery an external asymmetric bulge. The second mechanism is more common and involves a rearrangement of smooth muscle cells in the media for which the term remodelling can be used. The arterial wall is now recognised as a dynamic structure capable of altering in size. Glagov and colleagues’ work carried out on postmortem samples has been amply confirmed by epicardial echocardiography and intravascular ultrasound.5 ,6
Postmortem specimens of human coronary arteries that have been perfused at systemic pressure during fixation provide excellent illustrations of the process of compensatory enlargement (remodelling). In such preparations the lumen is round and the internal elastic lamina is expanded to its full capacity indicating an arterial state equivalent to maximal vasodilatation. Multiple cross sections of the artery can be made at 2 mm intervals and the area of the lumen and the vessel within the external elastic lamina measured. When these measurements are plotted against distance from the origin of the artery the two lines run parallel with distal tapering in a normal artery (fig 1). The distance between the two curves is a measure of the media plus intimal area. Plots of a diseased artery in which there are plaques interspaced with histologically normal segments of artery allow remodelling to be appreciated.

Diseased right coronary artery (proximal segment on left). Open circles, total vessel cross sectional area; closed circles, lumen cross sectional area.
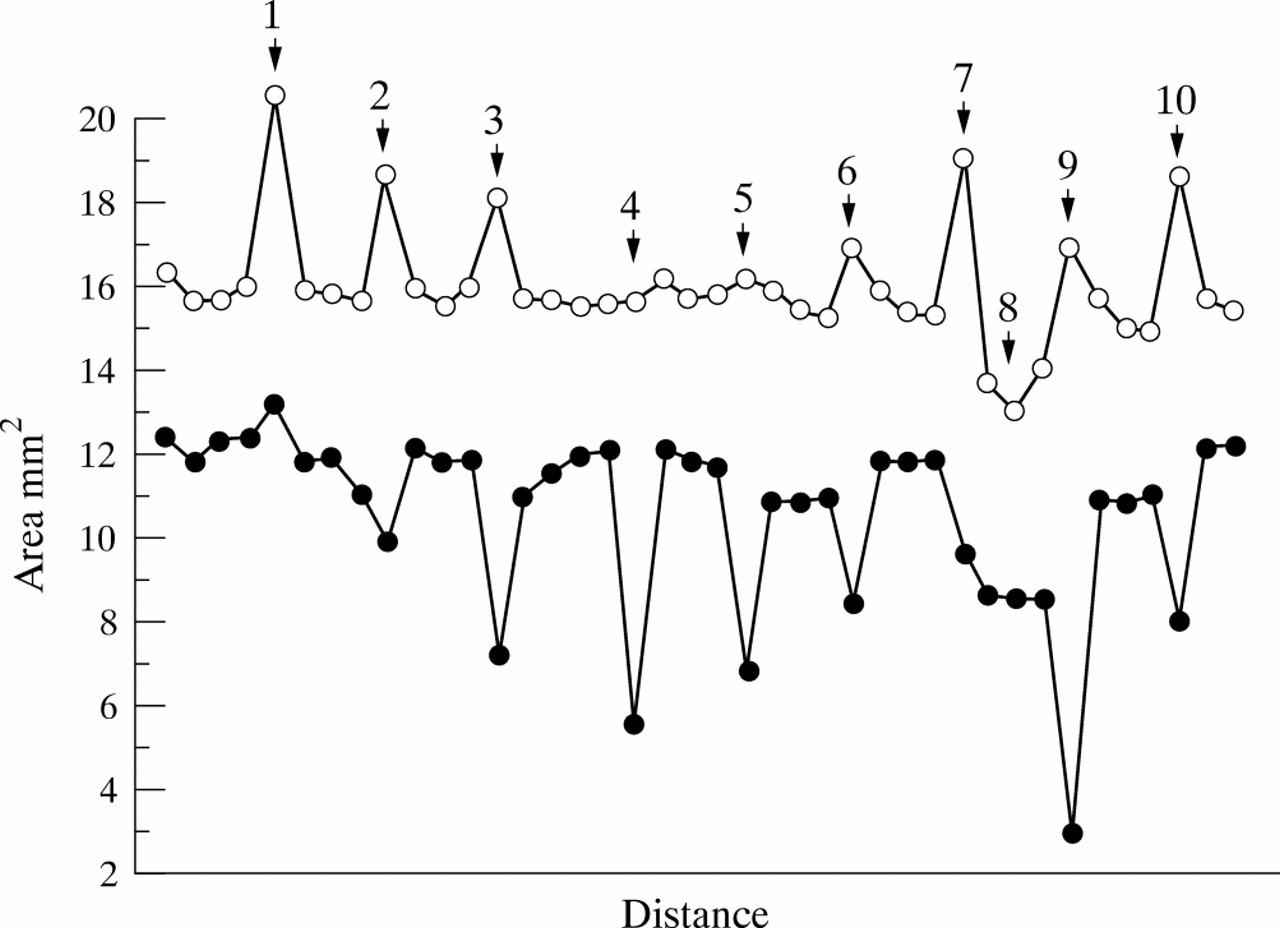
Figure 2 shows an artery with 10 plaques. Plaque 1 shows no luminal stenosis with an increase of the cross sectional area of the artery by 28.7%. This increase has compensated entirely for the plaque mass. In contrast plaque 9 is associated with a 47.2% diameter luminal stenosis and the cross sectional area of the vessel has increased by only 8.4%. This failure of remodelling is often known as inadequate compensation. Had the artery undergone the maximal achievable compensatory dilatation the degree of stenosis would have been far less.
{kind=link}
{kind=link}
Diseased right coronary artery (proximal segment on left). Open circles, total vessel cross sectional area; closed circles, lumen cross sectional area; arrows, plaques.
Many intravascular ultrasound studies show that compensatory enlargement (positive remodelling) is a common phenomenon and that inadequate degrees of compensation play a major role in stenosis generation. Such in vivo studies confirm what is illustrated in fig 2and table 1 that within a single artery different plaques show different degrees of compensatory enlargement, leading to the view that the process is plaque specific.
Diameter stenosis and remodelling of right coronary artery seen in fig 1
More recently intravascular ultrasound has suggested that some segments of arteries respond to the growth of a plaque by a reduction in the normal overall cross sectional area of the vessel. Vessel shrinkage is regarded as a significant contributor to luminal stenosis in “negative remodelling”.7 ,8 The concept of negative remodelling is more firmly established in postintervention restenosis. In 209 postintervention patients studied by intravascular ultrasound 73% of the mean overall loss in lumen at follow up was due to a decrease in vessel cross sectional area and only 23% due to an increase in plaque size. There was, however, sometimes an increase in total vessel area (22% of lesions) that was responsible for about 50% of the late lumen gain. It is not possible to predict whether a vessel will show positive or negative remodelling after angioplasty.
This issue of Heart reports work of two groups who have studied vascular remodelling in native atherosclerosis using IVUS in a preintervention patient population. Smits et al 9 found an equal proportion of lesions displaying compensatory enlargement (positive remodelling) and vessel shrinkage (negative remodelling). The results also demonstrated that vessel shrinkage (negative remodelling) was associated with a higher degree of luminal stenosis suggesting that this is the dominant form of remodelling in severe stenosis. Von Birgelen et al 10 found that inadequate remodelling was found in lesions with a smaller plaque area. They also found evidence of inadequate remodelling associated with lesions that had a concentric plaque distribution. Are we to assume therefore that inadequate positive remodelling occurs in approximately 40% of all atherosclerotic lesions?
Before we accept these figures the importance of defining the reference sites used in IVUS studies must be emphasised. Some studies have used the site (proximal or distal to the target lesion) with the maximum lumen but in which there may still be plaque. By doing this reference points can have larger plaque areas than the target lesion. In the early stages of compensatory enlargement some vessels may actually overcompensate and thus achieve an increase in luminal area despite the presence of plaque. The arterial segment in question is developing mild ectasia. If this reference point is used the number of lesions with vessel shrinkage will be overestimated. A more accurate approach would be to choose reference sites without any plaque. This may prove easier by histological assessment in pathology specimens than by IVUS.
It is also important to understand the significance of the target site. If the target site is taken as any point in which atherosclerosis is seen, then a range of plaque sizes and luminal stenoses will be observed. However, if the target sites used are confined to areas with maximal luminal stenosis on a preintervention study, then only lesions with advanced disease that have become both clinically and angiographically apparent, will be assessed. This is important when considering that Glagov et al’s3 results showed that only when the plaque occupies 40% or more of the cross sectional area of the artery did the luminal area decrease. In addition Wong et al 11 have shown that angiographically silent lesions were associated with compensatory enlargement while lesions of clinical and angiographic significance exhibited inadequate or negative remodelling. This suggests that by studying only high grade lesions in a preintervention population the results will be skewed towards lesions that have progressed beyond the limits for which vessel enlargement can compensate or include a greater proportion of lesions with vessel shrinkage. Such studies will provide data on the remodelling processes of severely stenosed lesions, but omit any information on the processes involved in early atherosclerotic disease. These studies therefore fail to answer the question of whether vessel enlargement and shrinkage are merely different phases of the same pathological process, or whether the lesion is committed to one form of remodelling from the initiation of plaque formation.
At present little is known about the factors that direct vessel wall remodelling. Von Birgelen et al’s10study suggests that eccentric plaques are more prone to compensatory enlargement. Thus the local increases in wall shear stress may stimulate the production of endothelium dependent vasodilatation in the disease free wall, which may in turn lead to structural changes in the media. Conversely concentric plaques without a disease free wall may not undergo these vasodilatory changes and instead undergo vessel shrinkage as a result of fibrous changes in the vessel wall. Other lesion specific factors such as plaque calcification, local inflammatory response in the adventitia, and plaque composition need to be assessed. The presence of all degrees of positive and negative remodelling within the same artery suggests that these local factors are more important than patient specific factors such as sex, racial origin or smoking. However, it is possible that the relation between total plaque area and vessel cross sectional area may differ between individuals.10 In 20 femoral arteries studied by IVUS, six subjects showed a good correlation implying that as plaques developed the artery enlarged. In 14 however there was no significant correlation implying that the increase in plaque area at least in some of the diseased segments was not matched by an increase in vessel cross sectional area. This work suggests that some individuals are better than others at arterial remodelling. The concept of remodelling thus challenges the conventional way of thinking about the generation of coronary artery stenosis. Until recently the dogma held was that coronary stenosis was dependent on plaque growth. We now know that it is more complex and dependent on the balance between plaque growth and the process of remodelling. The question is therefore not how large is the plaque, but will the vessel remodel. One determinant may well be how fast the plaque grows.