Article Text

Statistics from Altmetric.com
Stents have been shown to reduce the incidence of restenosis; however, they are not a cure. In two trials the angiographic restenosis rate was reported to be between 20% and 30% (in the Benestent II trial the unpublished quoted restenosis rate was 15%). These trials were based on stenting short, de novo lesions, in native coronary arteries. Whether such results are applicable to the widespread stenting that is currently being practised is not clear. It has been shown that the incidence of in-stent restenosis may vary according to the conditions of stenting and the vessel being stented. The number of stents deployed, whether there has been previous intervention, the size of vessel stented, the location of the lesion, whether the vessel is a native coronary artery or vein graft, co-morbid conditions such as diabetes, and stent design may all affect the incidence of in-stent restenosis. Rates of up to 40% have been reported when lesions other than de novo Benestent-type are treated. How factors such as multiple stenting promote restenosis is not always clear.
The next goal in stent development therefore should be to reduce further the need for repeat intervention for any stent deployed under any circumstance.
Biological consequences of stenting
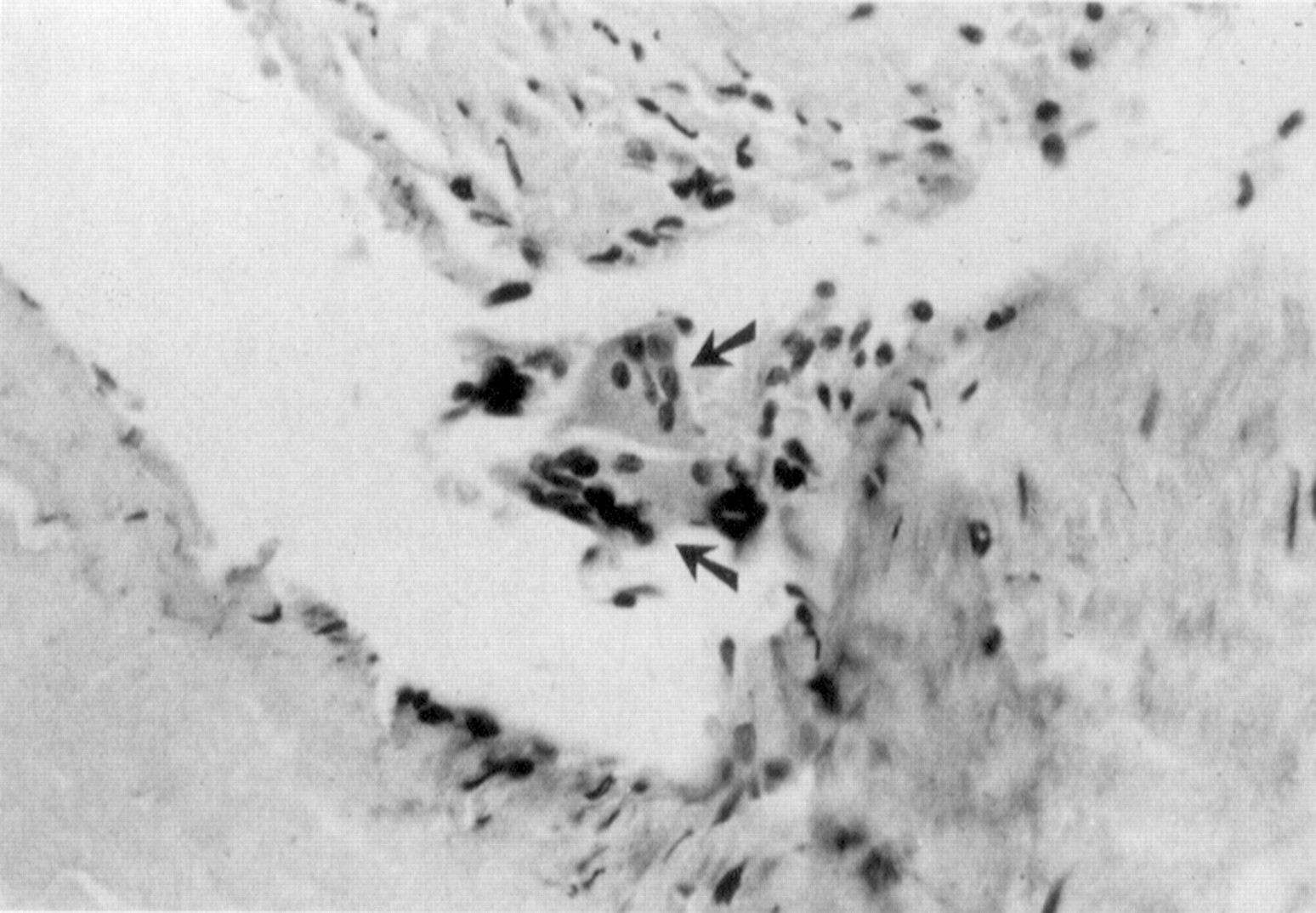
Stents prevent negative remodelling and recoil. The need for repeat intervention is predominantly because of tissue ingrowth. Extensive animal data and information from some human postmortem samples have identified the nature of in-stent restenosis. The process appears to be initiated by a giant cell based inflammatory reaction centred on the stent struts (fig 1).1 Thereafter the responses to the stent are similar to many of the changes demonstrated previously for balloon angioplasty. Smooth muscle cells migrate through the internal elastic lamina and proliferate in the newly formed intimal layer (fig 2).2 Angiographic studies and intravascular ultrasound suggest stents invoke a greater intimal proliferative response than balloon angioplasty.3 The factors that influence whether the tissue ingrowth is focal or diffuse are not understood. All stents have been shown to induce the tissue changes described.

Changes after stent implantation showing multinucleate giant cells (arrows). This figure (from von Beusekom1) demonstrates the inflammatory nature of stent implantation, a process that occurs much less after balloon angioplasty. Reprinted from J Am Coll Cardiol 1993;21:45–54 with permission from the American College of Cardiology.
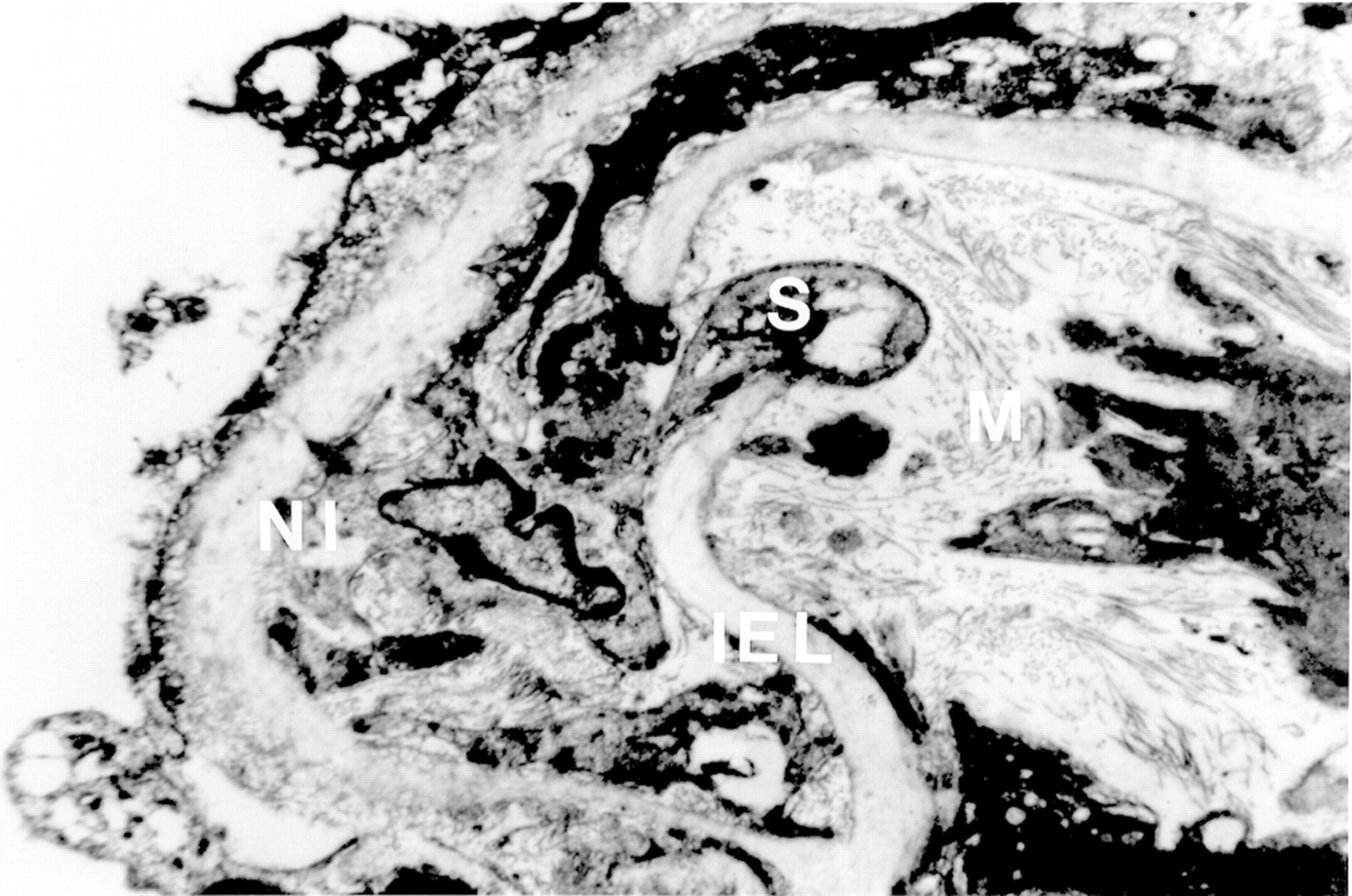
Progress of smooth muscle cell (S) from media (M) to new intima (NI) through the damaged internal elastic lamina (IEL) in a balloon injured artery. Once in the new intima the smooth muscle cell proliferates leading to restenosis.
The time course of in-stent restenosis appears similar to that seen after routine angioplasty, occurring within three months of the procedure. It would therefore be reasonable to suppose that to influence the process the same principle of inhibiting the initial phases of the process during the first week or so will apply. The effect of early inhibition leading to late reduction has been used to explain the longer term benefits of reduced clinical events with 7E3 (abciximab; ReoPro, Eli Lilly) in the EPIC trial.4
Of the three major components of in-stent restenosis (inflammatory process, smooth muscle cell proliferation, and production of the extracellular matrix) current approaches have been directed towards either removing the formed tissue or preventing the initial smooth muscle cell response.
Management of in-stent restenosis
BALLOON ANGIOPLASTY
The best way to treat in-stent restenosis is not clear. Most patients presenting with clinical recurrence undergo repeat balloon angioplasty using either the same size or a larger balloon. This has been shown to be safe and to increase the lumen size, although intravascular ultrasound has shown that catheter based strategies fail to recover the lumen size achieved during initial stent implantation. In one study it was shown that despite achieving an increase in minimal lumen area from a mean (SD) of 2.1 (1.4) to 6.2 (1.7) mm2 and a decrease in intimal area from 5.5 (2.4) to 2.9 (1.6) mm2, the final lumen area was 1.3 (1.9) mm2 less than the preintervention stent area (p < 0.0001).5 Some have suggested that the predominant effect of balloon angioplasty on in-stent restenosis is overexpansion of the stent rather than any significant effect on intimal tissue within the stent. It is probably a combination of both but a return to the immediate post-stent dimensions does not appear achievable. Part of the reason for this may by the constraints imposed by the stent itself—there appears nowhere for the tissue to go. As the principle of “the bigger the better” is well established it is perhaps not surprising that re-restenosis occurs after balloon treatment.
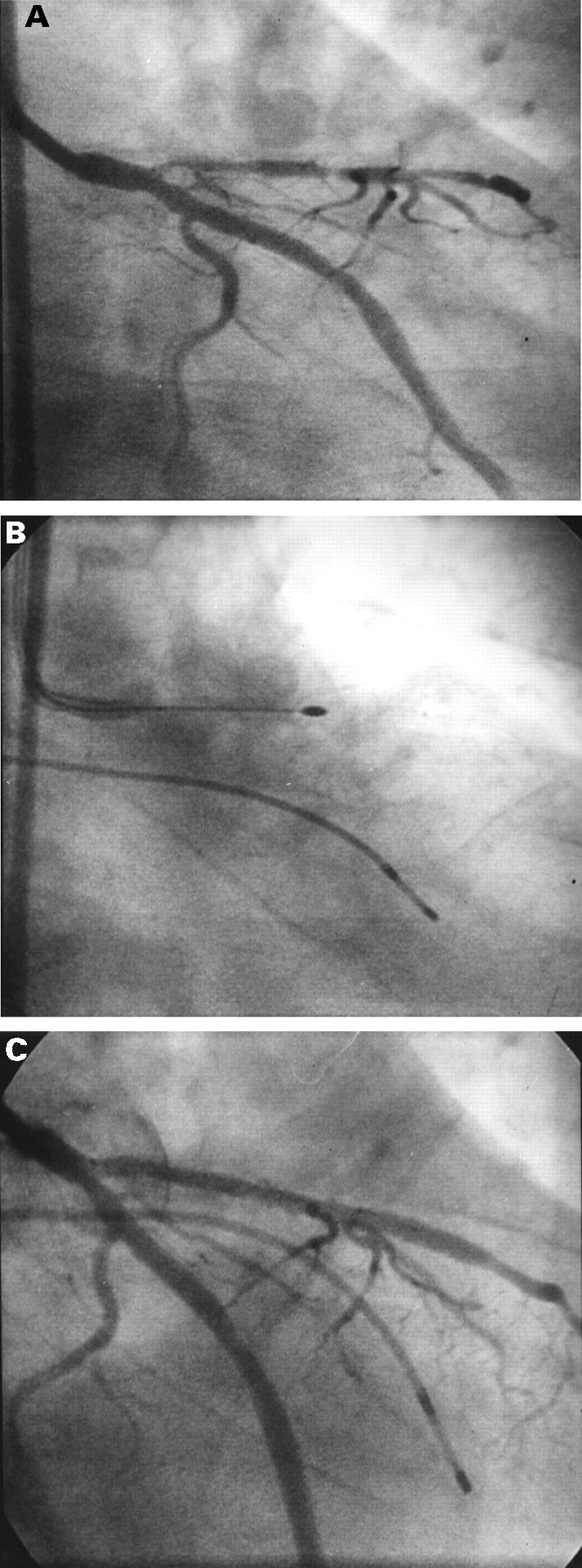
The outcome of balloon redilatation on re-restenosis appears to depend on the nature of the in-stent restenosis. Diffuse disease (fig 3) has been reported to have a high re-restenosis rate with figures of up to 80% quoted.6 Baim et al reported the US experience of treating in-stent restenosis with catheter based techniques. In patients treated with balloon angioplasty the re-restenosis rate was 54% (with a mean absolute lumen stenosis of 84%).7 Such high rates appear to translate into a high incidence of clinical restenosis. Tan et al reported that 22 of 47 patients with in-stent restenosis treated with angioplasty developed subsequent clinical events.8 Many of the published data apply to the Palmaz-Schatz stent, and whether balloon intervention for in-stent restenosis will be different for other stents is unclear.
{kind=link}
{kind=link}
{kind=link}
(A) Diffuse in-stent restenosis in a Cook GR II stent placed in the left anterior descending artery; (B) rotational atherectomy treatment; (C) final result after rotational atherectomy and ballooning. Regaining the original in-stent luminal diameter can be difficult.
The original value of stenting was based on the bigger the better principle. Thus it would appear to be a disadvantage if as large a lumen as possible cannot be achieved once restenosis has occurred. As restenosis has been considered a predictor for further restenosis then this makes treatment even more difficult.
ATHERECTOMY
One way of achieving a larger lumen following restenosis is to remove tissue (fig 3). Rotational atherectomy, which has become a niche intervention for treating calcified lesions, is being tested as a treatment for in-stent restenosis.9 Trials such as the ARTIST study have started recruitment. Abstracts and meeting presentations of available data from other sources have suggested some benefit. It appears that a larger lumen can be achieved using atherectomy. In one study the changes in lumen dimeter were increased from 0.7 (0.4) to 2.0 (0.5) mm after atherectomy and then to 2.4 (0.7) mm following adjunctive ballooning.10 It is unclear whether this absolute increase in lumen diameter, achieved through tissue removal, translates into any clinical advantage.
The BARRASTER registry involving 14 institutions has just finished the enrollment of 145 patients. Results presented to date show that the mean (SD) burr size used was 1.9 (0.7) mm, the final burr size 2.1 (0.3) mm, with atherectomy only being used in 26% of cases. The clinical success rate was 90% and the complication rate 4% including four dissections. There were, perhaps surprisingly, three deaths reported. The minimal luminal diameter before treatment was 0.6 (0.4) mm, after rotational atherectomy it was 1.7 (0.4) mm, and after atherectomy plus ballooning it was 2.1 (0.6) mm, compared with a reference minimal luminal diameter of 2.8 (0.5) mm. The mean clinical event rate at follow up in the 87 patients so far presented is reported to be 38%, but it is higher in those who had rotational atherectomy alone compared with those who also had ballooning.
It is unclear how much tissue needs to be removed and whether the principle of following the atherectomy with low pressure ballooning as is used in non-stented arteries (to prevent further injury) applies equally to post-stent atherectomy. Cost-benefit analyses need to be done and may help decide—for example, whether the use of multiple burrs is justified.
Although in-stent tissue can be safely removed with atherectomy, and while such treatments may reduce the re-restenosis within the stent from between 50–80% after ballooning to 30–40%, this cannot be regarded as satisfactory from either the clinical standpoint or the cost-benefit perspective. Prevention may be a better option.
Prevention of in-stent restenosis
The aim of prevention is to produce a stent that either fails to initiate the tissue response or one that is pretreated so that the subsequent tissue response is suppressed. Any such pretreated stents need to be safe, user friendly, and not to add significantly to the cost or time required for the procedure.
NON-REACTIVE STENTS
Metal has well described effects on flowing blood. Platelets are activated and may initiate smooth muscle cell proliferation through the release of growth factors. Platelet involvement leads to complex thrombus formation containing fibrin, thrombin, and other formed blood elements. The generated thrombin stimulates smooth muscle hyperplasia. Platelets are attracted to metal through the presence of a negative charge and have been shown to cover the struts within the first few minutes after stent placement. The stent itself initiates a well recognised inflammatory reaction within the vessel wall and exerts damage on smooth muscle cells, which in turn produce their own growth factors. There is greater intimal hyperplasia at the points where the stent struts impact on the medial layer. Stents that exert continued outward pressure on the vessel wall may result in an even greater increase in in-stent restenosis. To overcome the effects of the stent on blood and tissue, attempts have been made to produce non-reactive stents.
Polymer and polymer covered stents have been investigated extensively in animal models and it has been shown that the polymer itself may produce an excess tissue response.11 The degree of response varies with the type and amount of polymer—for example, it occurs with poly-L-lactide but not with others. Van der Giessenet al evaluated the biocompatibility of five different polymers and found extensive inflammatory responses with both biodegradable and non-biodegradable forms.12 This, together with the difficulty in developing a non-metal stent with sufficient radial strength, has led to a waning of interest in the pure polymer stent. Polymers are available that do not induce an inflammatory response and these have been used to coat stents.
RADIATION EMITTING STENTS
External radiation is a well established treatment for benign and malignant proliferative conditions. Such treatment has been shown to benefit keloid formation. The potential for local radiation to inhibit the arterial response to injury is currently the focus of major research programmes. King13 has recently highlighted the potential of radiation to deal with in-stent restenosis. Both γ radiation in the form of 192Iridium given via an external source placed within the stented artery and β radiation, delivered either locally by the positioning of intrastent Strontium/Yittium coils (90Sr) or by making the stent itself the radiation source, are being evaluated. The stent is made radioactive by placing it in a nuclear reactor so that it delivers sufficient amounts of32P to the artery. The advantage of using β emitters is their short penetration and because only 1/10 000th of the dose is present at five months. Initial studies have demonstrated an inhibitory effect on smooth muscle cells growing in culture. A dose of32P as small as 0.006 μCi/cm of wire significantly inhibited smooth muscle cell growth.14 A single dose of external radiation has been shown in an animal model to reduce intimal hyperplasia following balloon angioplasty by up to 37%.15In variations on a porcine model a number of investigators have delivered endovascular radiation in the form of 192Iridium and showed a dose-response relation with the greatest benefit at doses of 3.5–25 Gy. Again there appeared to be about a 40% reduction in intimal hyperplasia. β Emitting stents in a porcine model have also resulted in the development of less intimal area reduction compared with controls (2.4 (0.8) v 1.6 (0.7) mm2) with the degree of reduction being dose dependent.16 These radiation effects are not species specific.
There seems little doubt that radiation given as either as a γ emitter delivered endoluminally after stent deployment or as a β emitter given endoluminally after stenting or incorporated into the stent itself significantly inhibits the smooth muscle cell response. Such findings have led to a number of clinical trials. Initial studies in the peripheral circulation have shown a variable effect with90Yittium delivered locally. Early reports of a clinical evaluation in the coronary artery by Popowski et al have been disappointing,17 and dose adjustments are planned. The effect of 192Iridium on re-restenosis rates in patients randomised to stent plus radiation treatment or stent plus placebo has recently been published.18 The SCRIPPS trial enrolled patients presenting with restenosis after angioplasty, a potentially high risk group for re-restenosis that probably accounts for the high incidence of further restenosis in the control group. Patients were randomised to either stent plus radiation or stent plus placebo. The 55 randomised patients were re-evaluated at six and 12 months. The late loss in the treated group at six months was 0.38 (1.06) compared with 1.03 (0.97) mm in the control group (p = 0.03). The categoric restenosis rate was reduced dramatically to 17% in the treated group compared with 54% in control patients (p = 0.01).18
Despite the positive nature of this exciting study it is clear that the global application of such treatments will have a major impact on how interventionists work. Anxiety about the potential adverse effects of radiation both locally and generally still exists in some quarters and it has been suggested that much longer follow up to determine safety is required. Radiation protection for the interventionist may become an issue. The local effects of radiation on the vessel wall have been shown to lead to adverse changes such as stromal fibrin exudate, thinning of the media, and adventitial fibrosis,19 and these may explain the occurrence of one false coronary aneurysm and two occlusions in 21 patients in a clinical trial of 192Irdium. The results of the IRIS study evaluating 32P emitting stents in man are awaited. Storage problems and decay in radiation activity may be major drawbacks of β emitting stents.
DRUG ELUTING STENTS
Delivering drugs that prevent restenosis on to the stent itself has a number of advantages. The dose of drug required is less than would be needed systemically reducing the incidence of systemic side effects. The drug can be tailored to the pathological process and can be retained for the duration of the process. Achieving the correct balance between rate of elution and degree of retention is clearly important. Efficient ways of attaching the chosen agent to the stent are required. Ideally the agent should elute off the stent to influence the interstitial spaces, something that is less likely to happen if the agent is covalently bonded to the metal as with the Carmeda AB. This process was used to bind heparin to the Palmaz-Schatz stent in the Benestent II trial.20
An alternative way to deliver drugs with the stent is to incorporate them passively into a polymer coating already attached to the stent. The advantages are a lack of affect of the binding process on the biological activity of the agent, although the absolute quantity of the drug loaded by this method is less than if it were covalently bound.
Polymer coatings have been the subject of much discussion as they can be responsible for local inflammation and neointimal proliferation. The choice of the coating is therefore as important as that of the agent adsorbed to it. Studies in our laboratory using cellulose polymer coated stents in injured internal iliac arteries showed no increase in neointimal hyperplasia with a cellulose polymer compared with plain wire stents.21
Drug choice
The innovative study in stent delivery of a drug was the Benestent II trial. Although there seemed to be clear benefits in terms of stent thrombosis, no evidence has been presented that the changes in lumen dimensions seen in Benestent II, compared to Benestent I, related to the heparin: the reference vessel size, and the acute gain were significantly greater in Benestent II than Benestent I but no control group with non-heparin coated stents was included. Further, the late lumen loss for Benestent II was the same as for Benestent I (0.66 (0.58) v 0.68 (0.50 mm)) suggesting that the heparin itself had no affect on tissue responses.
There are many drugs that potentially could be passively or actively adsorbed onto stents including antithrombins and inhibitors of growth factors. One alternative to heparin is the glycoprotein Iib/IIIa antibody abciximab. It is currently used clinically to deal with arterial thrombus, given either prophylactically or after thrombus formation as with stent thrombosis. Abciximab affects integrins on platelets and smooth muscle cells. The integrin family of molecules comprise a series of α and β subunits. When combined, these form receptors that mediate a wide variety of cell functions via specific ligands. One of the main integrins responsible for mediating smooth muscle cell migration is the αvβ3 integrin. This shares a β3 subunit with the glycoprotein IIb/IIIa integrin present on platelets. It has been shown that abciximab, which inhibits αIIb/β3 on platelets, cross reacts with the smooth muscle cell integrin through the shared β3. If drugs such as abciximab can block platelet glycoprotein IIb/IIIa receptors they may influence the β3receptor on smooth muscle cells and influence restenosis beneficially. Other inhibitors of platelet receptors have been shown to affect smooth muscle cell growth.22
AZ1 is an inhibitor of platelet glycoprotein IIb/IIIa receptors.19 AZ1 loaded stents beneficially alter the interaction between the stent and the damaged vessel wall. The antibody was passively adsorbed on to cellulose polymer coated stents that were implanted in balloon damaged, flow reduced arteries. Control stents (either base polymer alone or an irrelevant antibody adsorbed in a similar manner) were implanted in the opposite side. There was a significant improvement in patency rate at two hours and 28 days when the AZ1 adsorbed stents were used (100% v 40%, p = 0.015). The AZ1 was adsorbed passively by a simple dipping technique and its elution, an important prerequisite for influencing the stent interstitial spaces, has been shown in vitro to follow a reproducible gradual bi-exponential pattern. The adsorption and elution of abciximab from polymer coated stents is currently being evaluated to determine whether abciximab loaded stents influence the activity of the vitronectin receptor and to reduce intimal hyperplasia. Adsorption and elution have followed a similar pattern, with 52% of the original amount adsorbed still being present after 12 days’ continual elution.23 Studies of the effects of the monoclonal antibody on human vascular smooth cell function in vitro have shown similar inhibition of cell adhesion to that seen with other anti-αvβ3 antibodies.24 If such techniques can be reproduced in vivo, a truly non-thrombogenic, non-restenosing stent may be possible. Altering the drug, its concentration, and the stent is relatively easy and inexpensive. The user friendliness of currently available stents should be unaffected. Further studies of loading stents with potent antithrombins and growth factors such as VEGF are ongoing by a number of laboratories.
Conclusions
In-stent restenosis occurs in at least 15% of patients and, depending on lesion and patient factors, this figure may be much higher. If it occurs in its diffuse form the use of balloon redilatation may result in re-restenosis rates of 80%. Techniques such as rotational atherectomy increase lumen diameter and appear to be safe. Currently available registry data suggest that such techniques improve the rate of re-restenosis to about 40%. This is still an important rate that has significant cost implications. Attention has turned towards preventing in-stent restenosis. Radiation delivered either endovascularly or on the stent itself appears a promising way forward. Alternatively, drugs that inhibit the biological reaction of the smooth muscle cells to balloon damage and stent deployment may be incorporated onto the stent itself. Clinical trials are awaited.
The need to improve clinical outcome and therefore to have cost-effective stenting suggests that the development of the truly non-reactive stent is a high priority.