Article Text

Statistics from Altmetric.com
Sudden cardiac death remains a worldwide health problem. More than 1000 such deaths occur daily in the United States1; most are secondary to ventricular fibrillation (VF).2Unfortunately, only about 5% of victims survive.3-5Sudden cardiac death is the most common “accidental” death in the US. A combined total of all airline, automobile, and drowning deaths would not equal the number of accidental or unexpected sudden cardiac deaths.
The key issue in successfully treating sudden cardiac death is early defibrillation. “The sooner the better” is never more true than with defibrillation of VF. In various settings, if defibrillation is applied immediately or very early, such as in the cardiac catheterisation laboratory or at cardiac rehabilitation centres, a survival rate of 90% is possible and should be expected.6-8 For every minute of delay, however, the survival rate appears to decrease by approximately 10%.9
The importance of early defibrillation for successful resuscitation has prompted important statements on both sides of the Atlantic supporting first responder defibrillator use. The American Heart Association has stated, “it is essential to integrate the concept of early defibrillation into an effective emergency cardiac care system”.10 To achieve this goal, the AHA endorses the position that “all emergency personnel should be trained and permitted to operate an appropriately maintained defibrillator, if their professional activities require that they respond to persons experiencing cardiac arrest”.10 The UK Department of Health Steering Group on ambulance performance standards has likewise proposed that:
Emergency medical system response should occur within eight minutes of cardiac arrest through the use of rapid response vehicles, including motor bikes, and through first responder automated external defibrillation schemes. The first responders are anyone who has been selected and trained by an ambulance service to provide basic support and, in the event of a cardiac arrest, to use an automatic defibrillator.11
The natural extension to these statements has been to consider expanding the boundaries of first responders to include the lay public.
Such concepts have made big headlines (fig 1), but are sometimes misunderstood. The public in public access defibrillation can be viewed on four levels.
The first tier would be first responders who provide emergency medical care as described by the American Heart Association and in the UK statements. These individuals can be easily taught to provide defibrillation with automatic external defibrillators
The second tier would be targeted responders such as police, security guards, and airline cabin crew. These individuals could be taught with relative ease the necessary skills to expand their duties to include first aid and public access defibrillation
The third tier would include family members with spouses, grandparents, or other family members at risk for sudden cardiac death. This type of programme has already been successfully implemented12
The fourth tier would be the lay public themselves. Successful programmes have taught basic cardiopulmonary resuscitation skills to members of the lay public. Such individuals could also be taught to use automatic external defibrillators.

Headlines highlighting interest in public access defibrillation.
The concept of public access defibrillation is based on deductive reasoning. Early defibrillation improves outcome from cardiac arrest due to VF.6-9 13-15 The increased availability of automatic external defibrillators should result in earlier defibrillation, leading to better outcome from cardiac arrest. The concept seems sound, but has not been proved prospectively.
Public access defibrillation is not a new idea. In 1986 the first defibrillator for public use became available (Life-Pack 100; Physio-Control, Redmond, Washington, USA). However, the concept failed to gain support for several reasons, particularly the lack of acceptance by physicians. Such devices were available through prescription, which was minimal despite family acceptance being reasonable, particularly in high risk families. Cost and reimbursement also slowed acceptance. Current enthusiasm for public access defibrillation has been spurred by recent breakthroughs in automatic external defibrillator technology. In the early 1980s advances in solid state circuitry and microcomputers occurred. Thereafter, algorithms were constructed enabling such machines to read cardiac rhythms, produce a storable shock, and then deliver such a defibrillation shock. Further recent advances include improvements in durability and low maintenance devices. These defibrillators are greatly simplified, easy to use, and highly portable, weighing less than the early models. Finally, the cost has dropped substantially in the past several years. At least five companies are producing such devices, and it is hoped that competition will drive the retail cost even lower.
Recently, the AHA sponsored a second conference on public access defibrillation. Several reports expanded current understanding of public access defibrillation and considered the potential and problems of this strategy.
An important report from Seattle, Washington, examined the “public” location in cardiac arrest (Becker LJ, et al, Second conference on public access defibrillation, Washington, DC, 1997). These investigators again confirmed that most cardiac arrests occur in the home (76%); only 16% occur in public sites. The most common public location for cardiac arrest was Seattle Tacoma Airport, with seven cardiac arrests each year. Penitentiaries were the second most common location. Shopping malls had 0.7 arrests each year, and sporting arenas during major events 0.4 each year. Other less frequent locations included hotels, government offices, schools, and churches.
White of the Mayo Clinic in Rochester, Minnesota, reported his results on police initiated defibrillation (White RD, Second conference on public access defibrillation, 1997). He has equipped the Rochester police department with automatic external defibrillators, reasoning that as the police often arrive first at an emergency, some of these could include cardiac arrest. Forty one of 108 patients having a cardiac arrest were first shocked by the police. Spontaneous circulation was restored without additional advance cardiac life support in 14 patients (34%). These patients were long term survivors. Among patients in whom spontaneous circulation could not be restored before arrival of the paramedics and who needed further advanced cardiac life support only 22% were long term survivors. The survival rate when police deliver the first shock is 49% compared with 43% when paramedics initiate early defibrillation.
Mosesso reported on a similar type of project in the suburbs of Pittsburgh, Pennsylvania. A historical control was used during which time the police were not equipped with automatic external defibrillators (Mosesso V, Second conference on public access defibrillation, 1997). The time from emergency call to delivery of the first shock was 11.8 minutes during the control period. After the police were equipped with automatic external defibrillators that time dropped to 8.7 minutes (p < 0.0001). Restoration of spontaneous circulation improved from 36% to 52% (p < 0.03), and survival more than doubled from 6% to 14% (p = 0.10).When the police arrived first during the control years only 3% of patients with cardiac arrest survived. A survival rate of 26% has been achieved since the police were issued with automatic external defibrillators (p < 0.05).
An interesting report was presented by the St John Ambulance Brigade, London, UK—a 2300 volunteer lay public first responder provider group that started training first aiders to use defibrillators in 1990 (Evans TR et al, Second conference on public access defibrillation, 1997). The St John Ambulance Brigade has major responsibilities for large public functions in the city of London, and provides first aid to attendees. In the past five years, since automatic external defibrillators were introduced, 17 patients with cardiac arrest have been defibrillated. Spontaneous circulation was restored in 14 patients. Twelve of the 17 were long term survivors. This is an astounding record of out-of-hospital success.
Quantas Airlines took a giant step forward in 1991, becoming the first major operational airline to deploy automatic external defibrillators on overseas flights. Several airlines had initially tried such strategies, but none continued. O’Rourke and Donaldson reported on five years’ experience of the automatic external defibrillator programme.16 Automatic external defibrillators were used 87 times: 47 were for monitoring, typically in patients with chest pain or palpitations, and 40 for cardiac arrests. Twenty two cardiac arrests occurred on the aircraft, while 18 occurred in the airport terminal. Six cardiac arrests on the aircraft were due to VF. Five of these six patients were successfully defibrillated with automatic external defibrillators, and two of six were long term survivors with excellent neurological function. A major problem was uncovered when these initial data were reviewed, namely that most cardiac arrests on the aircraft were discovered early in VF. Of the 22 cardiac arrests during flight, 13 were asystole and three had useless electrical activity. This finding is probably the result of undetected cardiac arrest while travellers were thought to be sleeping and late application of the automatic external defibrillator. Cardiac arrest in airport terminals (18 of 40) have a different pattern. Fifteen of 18 patients had VF: each of the 15 was successfully defibrillated with the device. Four of these 15 patients were neurologically intact, long term survivors. Quantas Airline’s experience of defibrillation (n = 21), six on the aircraft and 15 in the terminal, shows that automatic external defibrillators delivered an appropriate shock to all patients with VF. VF was terminated by defibrillator shock in 20 patients. Six of 21 patients had excellent long term outcome. The device correctly read a non-VF rhythm in each of 16 patients without VF on the aircraft and so no shock was delivered. During the last year following the lead by Quantas, several other airlines have committed to in-flight defibrillation potential by carrying automatic external defibrillators—Virgin Atlantic, American Airlines, and Cathay Pacific.
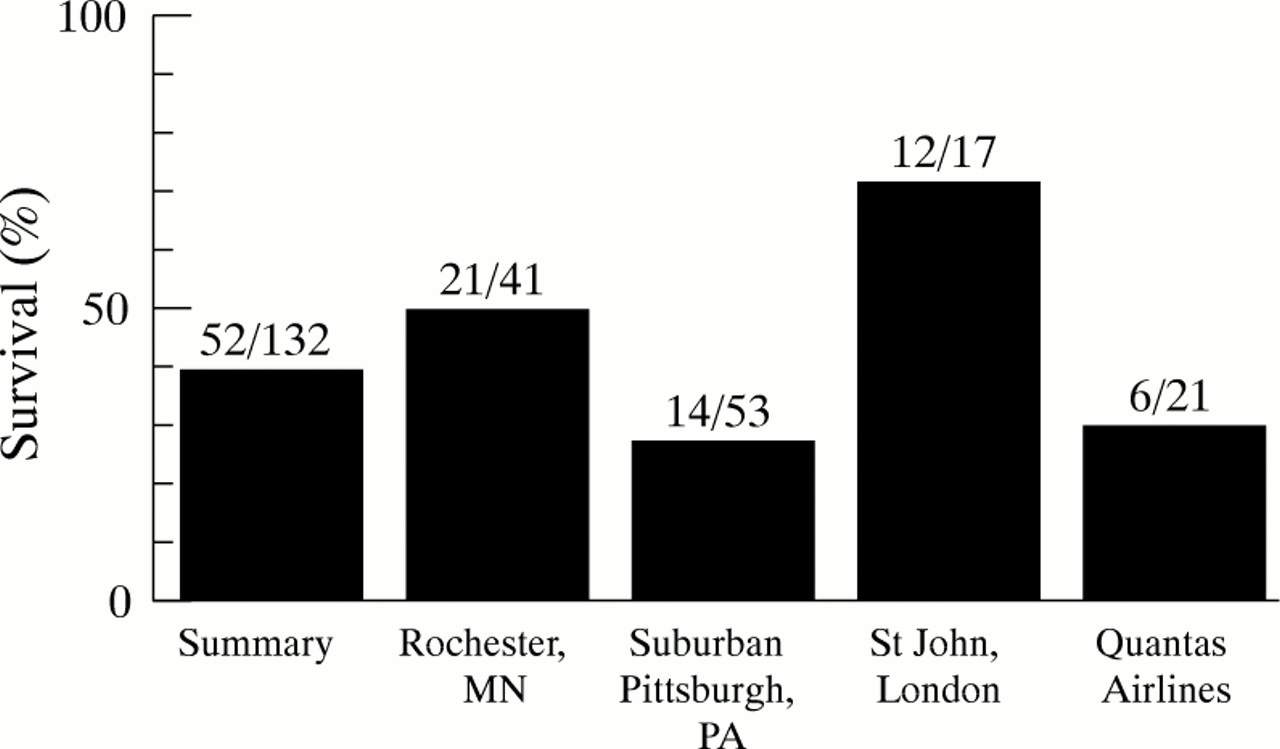
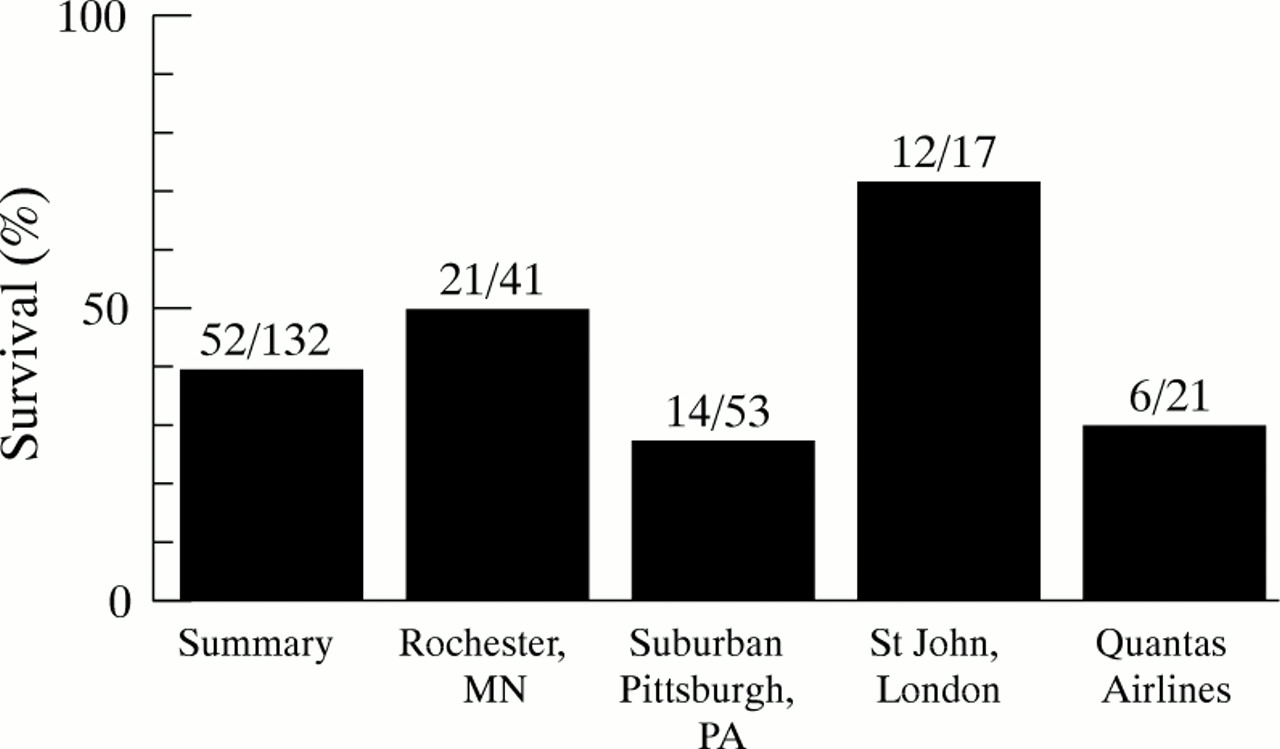
Figure 2 summarises these results for early defibrillation using automatic external defibrillators in patients with cardiac arrest due to VF.
{kind=link}
{kind=link}
Survival of patients suffering out of hospital cardiac arrest due to VF. Data from several presentations at the Second conference on public access defibrillation, 1997.
The future of public access defibrillation is an exciting one. More attention will be given to training the public in this technology to ensure safety. The devices should become less expensive with time, making them more readily available even to smaller communities. Finally, the actual optimal strategy for using such devices needs to be investigated. A randomised multicentre trial is planned to begin in the US during 1998 to examine prospectively whether trained targeted first responders equipped with automatic external defibrillators produce superior survival rates compared with those achieved by existing emergency medical systems. The primary end point will be neurologically intact long term survival, with secondary end points being time intervals, particularly time of call to shock, cost effectiveness, and resultant quality of life.
The future of treatment for cardiac arrest seems certain to include public use of automatic external defibrillators.