Article Text

Statistics from Altmetric.com
Percutaneous transluminal coronary angioplasty (PTCA) was introduced into clinical practice more than 20 years ago.1 The breathtaking growth of percutaneous coronary interventions (PCI) during the 1990s in Europe (fig 1) reflects their widespread acceptance for coronary revascularisation, challenging coronary artery bypass grafting (CABG). This review provides an overview of current coronary interventional techniques with emphasis on adjunctive pharmacologic treatments and indications of PCI in patients with chronic coronary artery disease.

Development of cardiac interventions during the 1990s in Europe. Data are obtained from the coronary circulation working group of the European Society of Cardiology and represent more than 30 European countries with a population > 500 million people. Note the steady increase in the number of PTCAs, coronary stent, and CABG procedures, in contrast to new devices.
Percutaneous coronary interventions
Balloon angioplasty
The balloon catheter is central not only to balloon angioplasty, but serves also as a complementary instrument for other intracoronary interventions such as delivery of stents or radiation sources. There are three types of ballon catheter (based on the relation between the guidewire and balloon)— fixed wire, over the wire, and Monorail balloon catheters—the latter being the most popular in Europe. There are five possible mechanism by which balloon angioplasty improves coronary haemodynamicsw1: (1) plaque compression; (2) plaque fracture; (3) stretching of the plaque free wall segment in eccentric lesions; (4) stretching of the vessel wall without plaque compression; and (5) medial dissection (fig 2). The most important mechanisms for improved blood flow appears to be the rupture and dehiscence of the atherosclerotic plaque, resulting in numerous fissures and sprouting of blood filled channels. The individual procedural outcome is a combination of different degrees of the above mechanisms, and the final luminal geometry following balloon angioplasty is determined by the ensuing remodelling of the vessel wall.w2–4

Schematic diagram of the primary mechanisms of balloon angioplasty and coronary artery stenting.
Despite this crude mechanism of arterial dilatation the initial success rate of balloon angioplasty is > 90% in single lesions.w5-7 The chief limitations to event free survival following balloon angioplasty have been abrupt vessel closure in the short term and restenosis in the long term.2 w8 Abrupt vessel closure, defined as the sudden occlusion of the target vessel during or after angioplasty, has been reported in 4–8% of cases.w9 w10 The pathophysiologic mechanisms underlying abrupt vessel closure are dissection (80% of cases), thrombus formation (20% of cases), and coronary artery spasm.w11 Abrupt vessel closure becomes apparent in 75% of cases while still in the catheterisation laboratory, the remainder occurring within 24 hours of the procedure. Abrupt vessel closure has been associated with death in 0–8% and myocardial infarction (MI) in 11–54% of cases. In the past > 20% of patients suffering abrupt vessel closure were referred for emergency CABG.w12 In the meantime coronary artery stents have become the method of choice in treating threatened or abrupt vessel closure, with success rates in excess of 90%.
Restenosis, defined as > 50% diameter stenosis at follow up angiography, has been the most important long term limitation of balloon angioplasty, with an incidence of 30–50% and need for target vessel revascularisation in 20–30% of patients.w8 Most restenosis occurs during the first four months following balloon angioplasty, and patients who are free of restenosis at six months are considered to be at minimal further risk.
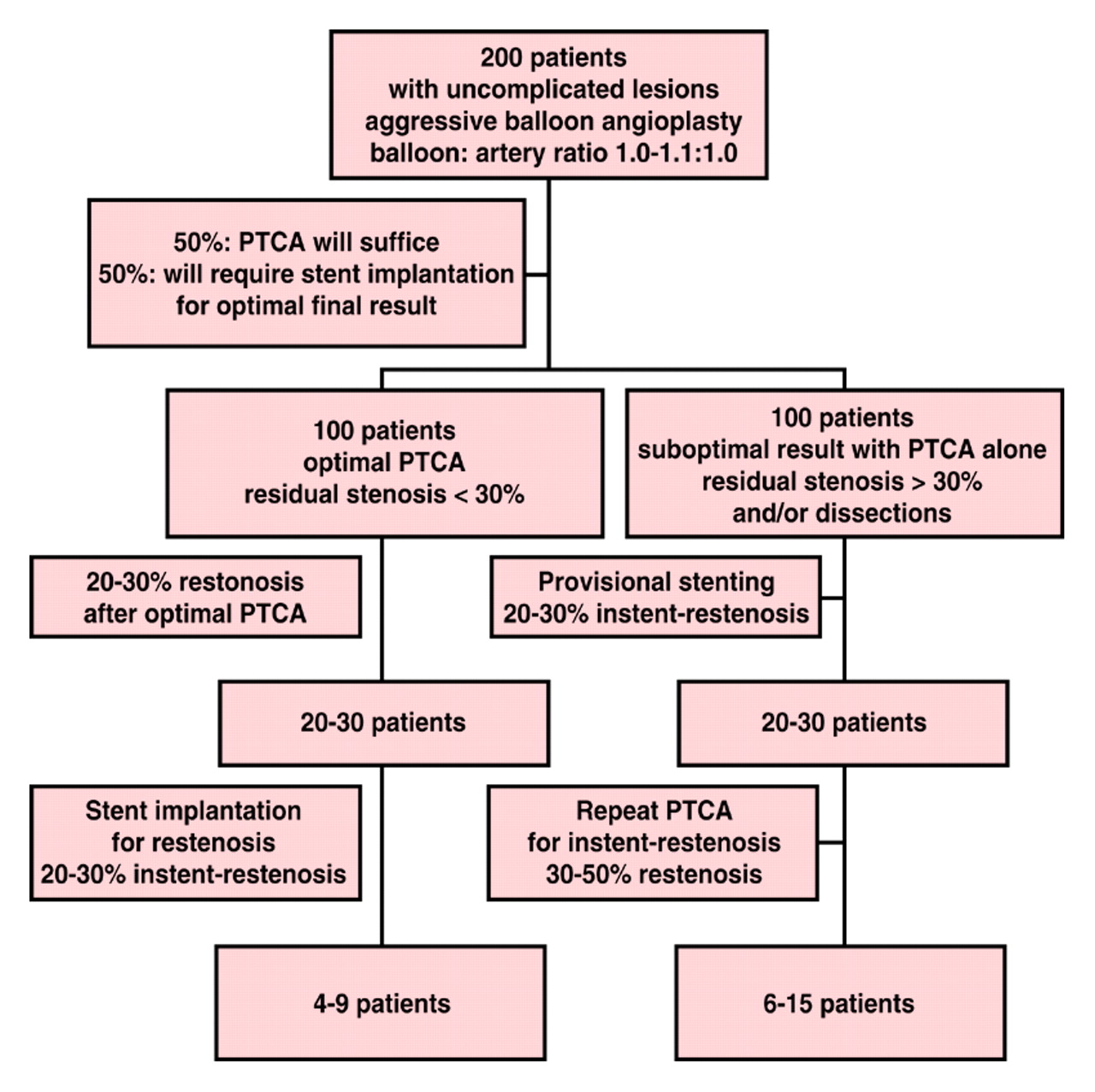
Today's paradigm of PCI is an aggressive approach to initial balloon angioplasty, so called optimal balloon angioplasty, to optimise luminal gain, with provisional stenting as a safety net for suboptimal balloon results (fig 2 and 3).3 A stent like balloon angioplasty result, arbitrarily defined in BENESTENT I as a residual stenosis < 30%, resulted in a minimal mean (SD) luminal diameter of 1.84 (0.52) mm (stent group 1.82 (0.64) mm), a binary restenosis rate of 16% (stent group 22%) and a one year event free survival rate of 77% (stent group 77%).w13 Similarly, patients in the DEBATE study undergoing balloon angioplasty, whose results were assessed physiologically by means of intracoronary Doppler flow velocity measurement, were found to have a favourable restenosis rate (16%v 41%, p = 0.002) and target lesion revascularisation rate (16% v 34%, p = 0.024), as well as freedom from recurrent symptoms or ischaemia (23% v 47%, p = 0.005) at six months follow up, if the coronary flow reserve was > 2.5 and the residual diameter stenosis < 35%.w14

Flow diagram illustrating the concept of provisional stenting with random patient numbers. The use of coronary artery stents on a provisional basis is associated with an excellent long term outcome and a low restenosis rate at minimised cost.
A strategy of optimal balloon angioplasty with “provisional” stenting in case of early recoil was compared with coronary artery stenting in 116 patients in the OCBAS trial.w15 After randomisation to PTCA, 14% of patients crossed over to stenting owing to early luminal loss. Although acute gain was significantly higher in patients implanted with coronary artery stents, there was no difference in net gain at six months between the two groups (1.32 (0.3) mmv 1.24 (0.29) mm for PTCA, p = ns). Furthermore, there was no difference in the angiographic restenosis rate (19% v 16% for PTCA, p = ns) and event free survival (81% v 83% for PTCA, p = ns). The percentage of patients in whom an optimal result can be achieved with balloon angioplasty alone is not known from controlled studies, but probably is around 30–50%.
Coronary artery stents
Coronary artery stents have become an important adjunct to conventional balloon angioplasty owing to their dual function of reducing acute complications and the long term risk of restenosis.4 w16–18 Various classification schemes of coronary artery stents have been put forward, including: type of delivery system (self expanding, balloon expandable); type of basic structure (mesh, slotted tube, coil, ring, and multidesign); and composition (stainless steel, tantalum, nitinol). More recently additional stent designs, including bifurcation and side branch stents, covered, coated, and radioactive stents, have been introduced. According to their design, coating, and composition stents differ with respect to radial force, flexibility, profile, trackability, radio-opacity, biocompatibility, thrombogenicity, and risk of in-stent restenosis. However, the basic principle underlying the therapeutic value of stents are independent of their design: increasing the arterial lumen by scoffolding the vessel wall; tagging of the intimal flaps between the stent surface and the vessel wall; and sealing of dissections.
Coronary artery stenting has been shown to be successful in > 95% of patients undergoing elective stent implantation in native vessels (single vessel and multivessel stenting) and saphenous vein grafts, and in > 90% of patients undergoing bailout stenting or stenting in the setting of acute MI.3 Stenting has proved useful for two applications: (1) as a bailout device, reducing acute ischaemic complications of PTCA; and (2) as an anti-restenosis device reducing the need for reinterventions in the long term. Threatened or abrupt vessel closure is the best indication for coronary artery stenting, with a dramatic reduction in the immediate need for emergency CABG currently to < 1%, and an improved angiographic outcome with less residual stenosis and increased restoration of TIMI III flow. The impact on death and MI during bailout stenting is less well established.
Elective coronary artery stenting has been compared with balloon angioplasty in several randomised trials, and proved efficacious in: (1) prevention of restenosis in native coronary arteries with a diameter > 3.0 mm (BENESTENT I and II, STRESS I and II),5 ,6 w19 especially in the case of isolated stenosis of the left anterior descending coronary arteryw20; (2) treatment of restenosis after initial balloon angioplastyw21; (3) de novo lesions in saphenous vein graftsw22; (4) acute MIw23; and (5) chronic total occlusion.w24–26 In the BENESTENT I and STRESS I and II trials patients with discrete de novo lesions in vessels > 3.0 mm diameter were randomised to undergo balloon angioplasty or stent implantation using the Palmaz-Schatz stent. Both studies showed that stents resulted in: (1) higher clinical success rate (STRESS 99% v 96% for PTCA, p = 0.04); (2) reduced angiographic restenosis rate at six months (STRESS 30% v 46% for PTCA, p < 0.01; BENESTENT 22% v 32% for PTCA, p = 0.02); (3) reduced target lesion revascularisation rate (STRESS 10%v 15% for PTCA, p = 0.06; BENESTENT 14%v 23% for PTCA, p < 0.01); and (4) reduced clinical event rate at one year (BENESTENT 23%v 32% for PTCA, p = 0.04; STRESS 18%v 27% for PTCA, p < 0.01).5 ,6
Since its introduction stent implantation posed a risk for subacute stent thrombosis with its associated sequelae of MI and death. Two recent modifications have substantially reduced the incidence of subacute stent thrombosis: optimised stent deployment and full stent expansion with circumferential apposition to the vessel wall using routine high pressure (> 10–14 atm) stent inflation;w27and dual antiplatelet treatment with aspirin and ticlopidine or clopidogrel.w28 Intravascular ultrasound assessment of coronary stent placement has not been conclusively shown to improve outcome and is largely omitted in clinical practice. Adoption of these principles led to current subacute stent thrombosis rates of < 2% under elective conditions (table 1), and a decrease in bleeding and vascular access site complications and length of hospitalisation to the same level as with conventional PTCA.
Coronary artery stents as antirestenosis devices—evidence from randomised trials and improved clinical outcome with changes in antithrombotic adjunctive treatment
Although coronary artery stents serve as antirestenosis devices and reduce target vessel revascularisation requirements compared with balloon angioplasty, they can themselves become a source of in-stent restenosis in 20–30% of cases. While stents counteract pathologic arterial shrinkage of the vessel wall, they may fail to prevent neointimal proliferation, which culminates in in-stent restenosis. Recently, Bauters and colleagues, studying 103 consecutive patients, reported a 98% procedural success rate with repeat PCI (versus 85% for PTCA) for treatment of in-stent restenosis, and 22% angiographic restenosis and 17% target lesion revascularisation rate at six months' follow up.w29 However, diffuse in-stent restenosis was associated with significantly higher restenosis rates compared with focal in-stent restenosis (42% for diffuse versus 14% for focal, p < 0.006).
In contrast to PTCA or other devices such as atherectomy or laser angioplasty, coronary artery stenting requires deployment of a permanent prosthesis and therefore requires long term evaluation with respect to potential metal fatigue, stent migration, and inflammatory responses.w30 Serial clinical and angiographic follow up over a three year period in 143 patients implanted with a Palmaz-Schatz stent revealed a favourable outcome with respect to death (9% at three years), MI (6% at three years), and target lesion revascularisation (17% at three years).7 Beside the expected initial loss of gain at six months of follow up owing to intimal proliferation, a late improvement in luminal diameter of the stented coronary artery segments at three years was observed, suggesting that restenosis was in fact prevented and not simply delayed after coronary stenting and indicating long term stabilisation of the lesion (fig 4).

Serial changes in mean (SD) minimal luminal diameter of 72 lesions (blue circles) for which sequential studies over a three year period were completed, compared with a reference diameter (red circles). Note the significant improvement in mean minimal luminal diameter during the period from one year to three years after implantation of the stent; p < 0.001 for the comparison between the points linked by brackets. Reproduced from Kimura T et al15with permission of the Massachusetts Medical Society.
Directional atherectomy
The principle of directional atherectomy (DCA) is removal of the atherosclerotic plaque by a rotating blade.2 The DCA catheter consists of a soft tapered nose cone which serves as a waste basket for ablated tissue, a cylindrical metal housing which contains a coaxial rotating cup shaped blade, and a long flexible shaft for delivery. The metal housing has a window measuring between 9–16 mm on one side and a non-compliant balloon on the opposite side. Once the open window is positioned within the stenosis, the eccentrically positioned balloon is inflated at 2–3 atm for protrusion of the plaque into the cutting chamber. The cutter is connected via a drive cable to a motor outside the patient and rotates at approximately 2000 rpm. By advancing the cutter the plaque material is shaved off and deposited within the nose cone. The balloon is then deflated and the window of the metal housing reoriented by slight rotation; the cutting process is repeated several times to achieve circumferential tissue ablation. Many patients require adjunctive balloon angioplasty for a satisfactory angiographic result.
Complications associated with DCA are side branch occlusion (1–8%), perforation (1%), coronary vasospasm (2%), abrupt vessel closure (1–8%), and distal embolisation (0–13%). DCA has been compared with PTCA in four multicentre randomised trials in native vessels (CCAT, CAVEAT-I, BOAT)w31–33 as well as saphenous vein grafts (CAVEAT II),w34 and resulted in better immediate luminal gain and higher procedural success at similar major complication rates. However, the immediate angiographic success failed to translate into improved clinical outcome. While the BOAT trial was the only study to demonstrate a significant reduction in angiographic restenosis rate,w33 the need for target lesion revascularisation and event free survival at six months and one year were similar between DCA and PTCA in all studies. Disconcertingly, patients in the CAVEAT trial treated by DCA were found to have higher rates of release of creatinine kinase CK-MB after the procedure (19% v 8% for PTCA), a higher one year mortality rate (2.2% v 0.6% for PTCA, p < 0.05), and a higher incidence of MI (7.6%v 4.4% for PTCA; p < 0.01).w32 Developed initially to reduce restenosis and to treat high grade lesions in the proximal coronary artery tree, DCA has been superceded by the more effective and easier to use coronary artery stent. Owing to DCA's unique feature of actually removing plaque material, its only indication may be the complex bifurcation lesion with plaque shifting not suited for stent implantation.
Rotational atherectomy
Rotational atherectomy is based on the concept of debulking an atherosclerotic plaque by drilling.2 The rotablator catheter consists of an elliptical burr coated with 20–50 μm diamond microparticles welded to a metal drive shaft which tracks along a central coaxial 0.009 inch guidewire. The drive shaft is connected to an air turbine which generates between 160 000 and 200 000 rpm. The operator controls the speed of rotation and advancement through the atherosclerotic plaque. Multiple passes of the rotablator are typically done with an initial burr-to-artery ratio of 0.5–0.6:1.0 followed by a second larger burr with a 0.75–0.8:1.0 burr-to-artery ratio. Since typically the burr size is only 80% of the vessel reference diameter the residual stenosis is usually treated with adjunctive PTCA. Rotational atherectomy by means of its high speed spinning burr features differential cutting. While the healthy, elastic arterial wall deflects beneath the spinning burr, hard, calcified and non-elastic atherosclerotic plaque should be selectively ablated. The size of the microparticles generated during rotational atherectomy is usually < 5 μm and the amount of microparticles is too small to result in impairment of blood flow.w35 Complications intrinsic to the rotablator are a potential for heat injury, “slow or no reflow” owing to embolisation of large microparticles or microcavitation bubbles (1.8–6.1%),w36 w37 large dissections (10–13%),w38 and perforation (0–1.5%).
Acute procedural success has been high (90–99%) even in high risk lesions. Rotablation proved superior to PTCA (procedural success 89%v 80% for PTCA, p < 0.05; MACE 3.2%v 3.1%, p = ns) in the ERBAC trial,8 a randomised comparison of rotablation and PTCA in complex lesions (American Heart Association/American College of Cardiology type B and C). However, rotablation failed to improve six month angiographic restenosis rates (57% v47% for PTCA, p = 0.14), and both target lesion revascularisation (42% v 32% for PTCA, p = 0.013) and ischaemic complications (46% v 37% for PTCA, p = 0.04) were more frequent in patients undergoing rotablation (table 2). Rotational atherectomy may still be of value in the treatment of heavily calcified, non-dilatable lesions. However, in long, calcified lesions the advantage of rotational atherectomy levels off and comes at a price of increased complications.
Results of the ERBAC trial, a randomised comparison between balloon angioplasty, rotational atherectomy, and excimer laser angioplasty
Contraindications for the use of rotational atherectomy are thrombus containing lesions, degenerated saphenous vein grafts, and lesions ⩾ 25 mm.
Laser angioplasty
Excimer laser coronary angioplasty (ELCA) is the most thoroughly investigated laser technology applied to coronary interventions. It uses a high intensity, short duration (100–200 ns) pulsed wave ultraviolet light (308 nm) generated in a xenon chloride medium with a penetration depth of 100 μm.w39 The ultraviolet light is transmitted via a fibreoptic bundle arranged around the central lumen of a polyethylene catheter which is available as an over the wire or Monorail system. The laser catheter is advanced over the coronary guidewire to the lesion, and laser energy is applied as the catheter is advanced through the plaque. Excimer laser energy ablates tissue by a combination of three mechanismsw40: (1) photomechanical energy resulting in acoustic shockwaves as the principal modus of luminal gain w41–43; (2) photothermal energy which vapourises tissuew44 w45; and (3) photochemical energy which is able to break directly the intramolecular bonds.w46 To achieve an optimal final result adjunctive balloon angioplasty is required in almost all cases (> 95%).
ELCA has been compared with PTCA in the ERBAC trial.8There was no difference between PTCA and laser angioplasty with respect to procedural success (77% v 80% for PTCA, p = ns) and major in-hospital complications (4.3%v 3.1% for PTCA, p = ns). However, at six months' follow up the angiographic restenosis rate (59%v 47% for PTCA, p = 0.04), target lesion revascularisation rate (46% v 32% for PTCA, p = 0.01), and late ischaemic events (48%v 37% for PTCA, p = 0.02) were significantly more frequent in patients treated with laser angioplasty (table 2).
Complications associated with excimer laser angioplasty are perforations (1–3%) and a high incidence of dissections (13–21%) caused by the formation of intravascular vapour bubbles. The only indication where laser angioplasty may prove of some value is for revascularisation of chronic total occlusions with a laser guidewire. In the randomised TOTAL trial the excimer laser wire increased the initial success rate from around 50% to 60%.w47 However, this effect was largely confined to crossover cases, and conventional guidewires but not specific recanalisation systems or newer generation hydrophilic wires were assessed.
Adjunctive pharmacologic treatment
The therapeutic effect of arterial vessel enlargement through PCI is accompanied by various degrees of arterial injury with exposure of thrombogenic components. Depending on the degree of activation of the coagulation cascade, as well as platelet adhesion and aggregation, this may result in intracoronary thrombus formation and subsequent ischaemic sequelae. Therefore, inhibition of platelets and the coagulation system has always been central to interventional investigations.
Anticoagulants during PCI
Heparin
Unfractionated heparin is a glycosaminoglycan mixture composed of variable length polysaccharides with molecular weights ranging from 3000 to 50 000 daltons.w48 Heparin exerts its anticoagulant effect by formation of the heparin-antithrombin III complex, which inhibits thrombin and activated factors IX, X, XI, and XII. Although there is general agreement that patients undergoing PCI should receive heparin before the intervention, controversy surrounds the issue of optimal heparin dosage and the need for prolonged heparin infusion following PCI. Narins and colleagues observed an inverse relation between the level of anticoagulation (measured by activated clotting time (ACT)) and the occurrence of acute ischaemic complications,w49 and the recommended adequate threshold for anticoagulation is arbitrarily set at an ACT of > 300 seconds. This contrasts with several randomised and open prospective studies which established data on the safety and efficacy of routine low dose heparin (5000 IE) in patients undergoing PCI independent of the level of ACT,w50–52 and failed to demonstrate an additional benefit of continuous heparin infusion after PCI in low risk patients.w51 w53 Without increasing the risk for ischaemic complications, the approach of routine low dose heparin during PCI offers the advantages of a lower incidence of bleeding complications, faster sheath removal, and shorter hospitalisation. In addition it does not preclude the administration of unplanned, adjunctive glycoprotein IIb/IIIa receptor inhibitors, which would be preferable in case of ischaemic complications.
Low molecular weight heparins, obtained by chemical or enzymatic depolymerisation of the polysaccharide chains of unfractionated heparin, have a better bioavailability, result in more reproducible anticoagulation without need of monitoring, and induce less platelet activation compared with unfractionated heparins.w54 The REDUCE trial, a restenosis study, randomly compared intravenous administration of the low molecular weight heparin reviparin with unfractionated heparin during PCI and revealed a significant reduction in early major ischaemic events (first three days) in favour of reviparin (reviparin 4% v heparin 8%, p = 0.03), but no long term clinical or angiographic benefit at six months of follow up.w55 The role of low molecular weight heparins in the prevention of bleeding and ischaemic complications during PTCA and coronary stenting is currently under investigation, and these agents may replace unfractionated heparin as they have for other indications.
Direct thrombin inhibitors
In contrast to heparin direct thrombin inhibitors such as hirudin, hirulog, argatroban, and others do not require antithrombin III as a cofactor, and inhibit both circulating and clot bound thrombin. Three randomised trials with over 6700 patients compared the efficacy of unfractionated heparin with hirudin (HELVETICA, GUSTO IIb)w56 w57 and hirulog (Hirulog angioplasty study)w58during PCI. Patients receiving direct thrombin inhibitors had a lower incidence of bleeding complications; however, the therapeutic benefit was modest at best with a reduction in ischaemic complications limited to subgroups and acute events only. In light of these results and the availability of more potent glycoprotein IIb/IIIa receptor antagonists, the role of direct thrombin inhibitors will probably be reserved for patients with adverse reactions to heparin, for example, heparin induced thrombocytopenia.
Vitamin K antagonists
Coumarin derivatives were administered in conjunction with full dose heparin, aspirin, and dipyridamole as thromboprophylaxis early in the coronary stent era. However, subsequent clinical trials established the superiority of a dual antiplatelet treatment over oral anticoagulants in preventing both cardiac events and bleeding complications after coronary artery stenting.9 w28 w59 w60 This clinical benefit, coupled with the salutary effects of shorter hospitalisation time, reduced cost, and simplification of the pharmacological regimen, no longer support the use of oral anticoagulants after stent implantation.
Antiplatelet agents during PCI
Aspirin
The beneficial effect of aspirin during PCI has been shown in the Montreal heart study, in which treatment with aspirin and dipyridamole was superior to placebo in the prevention of periprocedural Q wave MI (aspirin and dipyridamole 2% v placebo 7%, p = 0.01).w61 Dipyridamole has not been found to provide an additional benefit over aspirin alone in subsequent studies.w62 Low dose aspirin (75–325 mg per day) is recommended in patients undergoing PCI, ideally administered at least one day before the procedure and continued indefinitely thereafter.
Thienopyridines
Ticlopidine and clopidogrel are thienopyridine derivatives which inhibit platelet function independent of aspirin by interference with the platelet ADP receptor.w63 The interest in dual antiplatelet treatment with aspirin and ticlopidine in patients undergoing coronary stent implantation stemmed from the pathophysiological understanding that stent thrombosis was predominantly mediated by platelets rather than abnormalities of coagulation activation.w64 Furthermore, intensive anticoagulation after stent placement was complicated by excessive vascular access site problems, prolonged hospitalisation, and increased cost, seriously limiting the benefits of coronary artery stents. Several randomised clinical trials assessed the efficacy of dual antiplatelet treatment with aspirin and ticlopidine compared with aspirin alone and aspirin-anticoagulant treatment after coronary stent implantation in low (STARS),9 intermediate (ISAR, FANTASTIC),w60 w65 and high risk (MATTIS)w59patient populations (fig 5). These trials showed that: (1) dual antiplatelet treatment with aspirin and ticlopidine is superior to both aspirin monotherapy and a combination of aspirin and oral anticoagulation in the prevention of stent thrombosis; (2) rates of bleeding and vascular complications are less frequent; and (3) hospitalisation duration is shorter with antiplatetet compared with anticoagulant treatment.

Summary of results of four randomised coronary artery stent thromboprophylaxis trials. Dual antiplatelet treatment with aspirin and ticlopidine was superior to oral anticoagulation and aspirin treatment in the prevention of major adverse cardiac events in all trials. In the STARS trial dual antiplatelet treatment was superior to aspirin alone.
Moussa and colleaguesw66 recently compared the safety and efficacy of ticlopidine with clopidogrel in a longitudinal uncontrolled study, and found no difference in rates of stent thrombosis or major adverse cardiac events at one month follow up. In the CLASSICS trial clopidogrel with and without a loading dose was compared with ticlopidine in patients undergoing coronary stenting. The findings of the study at 28 days of follow up were: (1) a superior safety profile of clopidogrel with a significantly reduced combined end point of major bleeding complications, neutropenia, and thrombocytopenia (ticlopidine 9% v clopidogrel 5%, p = 0.005); (2) a well tolerated loading dose of clopidogrel without increased bleeding complications; and (3) a comparable efficacy with respect to major adverse cardiac events. Therefore, it is anticipated that clopidogrel will replace ticlopidine as the thienopyridine of choice.
Glycoprotein IIb/IIIa inhibitors
While platelets may be activated by numerous agonists, platelet aggregation, the prerequisite for thrombus formation, has one final common pathway mediated by the platelet glycoprotein IIb/IIIa receptor, a member of the integrin family. Therefore, inhibition of the glycoprotein IIb/IIIa receptor appealed as the therapeutic target in the prevention of largely platelet mediated ischaemic complications during PCI. Several randomised trials have assessed the role of glycoprotein IIb/IIIa receptor antagonists during coronary interventions, including the monoclonal antibody abciximab (EPIC, EPILOG, EPISTENT, CAPTURE, RAPPORT),10 w67–70the peptide molecule eptifibatide (IMPACT II),w71 and the non-peptide molecule tirofiban (RESTORE)w72 in over 15 000 patients with clinical presentations ranging from stable coronary artery disease to unstable angina pectoris and acute MI. All trials consistently demonstrated benefits in the reduction of early death, non-fatal MI, and urgent revascularisation (fig 6).11While this effect was maintained in patients receiving abciximab during long term follow up, the benefits have not been durable with tirofiban and eptifibatide. Specifically, abciximab is the only glycoprotein IIb/IIIa receptor antagonist reported to reduce mortality significantly in a subgroup of patients in the EPIC trial admitted with an acute coronary syndrome (three year mortality reduction 60%, p = 0.01),w73 and more recently in the EPISTENT trial (one year mortality reduction of 50%, p = 0.04).12 In summary glycoprotein IIb/IIIa receptor antagonists administered during PCI appear to: (1) reduce the incidence of death or non-fatal MI complicating PCI (in case of abciximab); (2) reduce the need for bailout stenting during PCI; (3) provide benefit in all patient subgroups, and (4) do not result in excessive bleeding complications if weight adjusted lower doses of heparin are adhered to.

Odds ratio and confidence interval (CI) concerning death, MI, or additional coronary revascularisation at 30 days with glycoprotein IIb/IIIa receptor antagonists compared with placebo. Reproduced with permission from Meier B. Balloon angioplasty. In: Topol EJ, ed. Comprehensive cardiovascular medicine. Philadelphia: Lippincott-Raven, 1998:2251–84.
Indications for PCI in chronic coronary artery disease
The indications for PCI have expanded during the past two decades, and no absolute contraindications remain (table 3). Single vessel coronary artery disease (CAD) remains the principal indication for PCI, with over 80%w74 of procedures performed in Europe and over 90% in the USA. This exponential growth of PCI has been largely at the expense of medical treatment rather than surgical revascularisation. Beside clinical and angiographic factors, operator volume has been recognised as a major determinant of outcome in several recent studies.w75–78 There is no upper patient age limit to the applicability of PCI; however, the threshold is shifted in favour of PCI compared with CABG in the very elderly owing to the higher perioperative morbidity and mortality in this patient population. Initial concerns of a sex difference in the outcome of PCI with women, felt to be at higher risk for acute ischaemic complications, did not find confirmation in more recent registries and clinical trials. While acute thrombotic coronary occlusion, even of the left main stem, represents no major hurdle for performing PCI, chronic total occlusion is the single most important reason not to attempt PCI. The following comparison of PCI with alternative treatments is limited to patients with chronic coronary artery disease.
Trial acronyms
- ACME:
- Angioplasty Compared with Medicine
- ARTS:
- Arterial Revascularisation Therapy Study
- AVERT:
- Atorvastatin Versus Revascularization Treatment Investigators
- BARI:
- Bypass Angioplasty Revascularization Investigation
- BENESTENT:
- Belgium-Netherlands Stent Study
- BOAT:
- Balloon versus Optimal Atherectomy Trial
- CAPTURE:
- Chimeric 7E3 Anti-Platelet in Unstable Angina Refractory to Standard Treatment Trial
- CAVEAT:
- Coronary Angioplasty Versus Excisional Atherectomy Trial
- CLASSICS:
- CLopidogrel plus Aspirin Stent International Cooperative Study
- DEBATE:
- Doppler Endpoints Balloon Angioplasty Trial Europe
- EPIC:
- Evaluation of IIb/IIIa platelet receptor antagonist 7E3 in Preventing Ischemic Complications trial
- EPILOG:
- Evaluation of PTCA to Improve Long-term Outcome by c7E3 GP IIb/IIIa receptor blockade trial
- EPISTENT:
- Evaluation of Platelet GP IIb/IIIa Inhibitor for Stenting
- ERBAC:
- Excimer laser, Rotational atherectomy, and Balloon Angioplasty Comparison Study
- FANTASTIC:
- Full Anticoagulation Versus Ticlopidine plus Aspirin After Stent Implantation Trial
- GUSTO:
- Global Use of Strategies To Open Occluded Coronary Arteries
- HELVETICA:
- Hirudin in a European Trial Versus Heparin in the Prevention of Restenosis After PTCA
- IMPACT:
- Integrilin to Manage Platelet Aggregation to Combat Thrombosis Trial
- ISAR:
- Intracoronary Stenting and Antithrombotic Regimen Trial
- MATTIS:
- Multicenter Aspirin and Ticlopidine After Intracoronary Stenting Trial
- OCBAS:
- Optimal Coronary Balloon Angioplasty with Provisional Stenting versus Stent Trial
- RAPPORT:
- Reo Pro and Primary PTCA Organisation and Randomized Trial
- REDUCE:
- Reduction of Restenosis After PTCA, Early Administration of Reviparin in a Double-blind, Unfractionated Heparin and Placebo Controlled Evaluation
- RESTORE:
- Randomised Efficacy Study of Tirofiban for Outcomes and Restenosis Trial
- RITA:
- Randomised Intervention Treatment of Angina Trial
- SOS:
- Stent Or Surgery trial
- STARS:
- Stent Anticoagulation Regimen Study
- STRESS:
- Stent Restenosis Study
Indications and contraindications for PCI
PCI versus medical treatment
PCI has been compared with medical treatment in patients with CAD in several randomised clinical trials (table 4). In the ACME trial13 involving patients with symptomatic single vessel CAD, the group allocated to PTCA had earlier and more complete relief of angina and better exercise performance during follow up. However, patients undergoing PTCA had an increased risk of undergoing emergency CABG because of procedural complications, although there were no differences with respect to death and infarction. Similar findings were reported in the RITA-2 trial14 comparing PTCA with medical treatment in symptomatic patients with single and double vessel disease. Patients undergoing PTCA featured greater relief of angina and better exercise performance at an increased risk of death and MI (6% PTCA group v 3% medically treated group, p = 0.02), largely because of enzyme elevations at the time of the procedure.
Randomised comparison of medical treatment with PCI in patients with stable CAD
In the recently reported AVERT trial a strategy of aggressive lipid lowering treatment with atorvastatin was compared with PCI in minimally symptomatic (Canadian Cardiovascular Society class I–II), mostly single vessel CAD patients.w79 There was a non-significant trend towards a reduction in the composite end point of death, MI, revascularisation, and worsening angina in patients allocated to atorvastatin (13% atorvastatin group v 21% PCI group, p = ns), but the differences in favour of atorvastatin treatment were exclusively limited to a decreased revascularisation and rehospitalisation rate. As in previous trials patients undergoing PCI in AVERT had significantly improved symptoms compared with medically treated patients, and one wonders why the interventionally treated patients had adequate cholesterol control withheld despite established evidence of their beneficial effect in secondary prevention. All the above studies comparing PCI with medical treatment do not reflect current practice of interventional cardiology with widespread utilisation of coronary stents and glycoprotein IIb/IIIa inhibitors, which contributed significantly to a decrease in major adverse cardiac events and target vessel revascularisation. In summary, PTCA effectively relieves symptoms and improves exercise performance at the cost of a small incidence of MI and a need for reinterventions because of restenosis in patients with single vessel CAD.
PCI versus bypass surgery
PTCA has been compared with left internal mammary artery (LIMA) grafting in 134 patients with isolated proximal left anterior descending artery (LAD) stenosis in the randomised Lausanne study (table 5).w80 At five years of follow up there were no differences between patients allocated to PTCA and LIMA grafting with respect to death, Q wave MI, functional status, and antianginal drug treatment. However, patients allocated to PTCA had more frequent non-Q wave infarction related to abrupt closure or unstable angina related to restenosis, and required additional revascularisation procedures more often compared with surgically revascularised patients. The same investigators initiated a randomised trial in 123 patients with isolated proximal LAD stenosis comparing coronary stenting with LIMA grafting. There were no differences in the incidence of in-hospital death and MI, with low rates in both groups. During follow up the combined end point of death and MI was equal; however, 21% of stented patients required additional revascularisation compared with no patients in the surgical group.
Randomised comparison of CABG with PCI
Several randomised trials compared PTCA with CABG in patients with multivessel CAD.15 ,16 w81–85 The results of these trials have been remarkably consistent (fig 7) and revealed that an initial strategy of PTCA and CABG in selected patients with multivessel CAD results in: (1) similar survival and freedom from MI 1–7 years after the procedure; (2) a better relief of angina in CABG patients at least during the first year after the intervention; (3) an increased need for further coronary interventions in patients allocated to PTCA mostly during the first year after the intervention; and (4) similar long term costs during a follow up period of 5–8 years. An important issue raised in the BARI trial56 was that the subgroup of treated diabetic patients had significantly better survival rates with CABG (66% PTCA v 81% CABG, p = 0.003).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
(A) Risk ratio and 95% confidence intervals for death or MI after CABG or PTCA for multivessel CAD at one, three, and five years in six randomised trials. (B) Risk ratio and 95% confidence intervals for reintervention after an initial strategy of CABG or PTCA for multivessel CAD at one year of follow up in six randomised trials. Reproduced with permission from Meier B. Balloon angioplasty. In: Topol EJ, ed. Comprehensive cardiovascular medicine. Philadelphia: Lippincott-Raven, 1998:2251–84.
The advent of coronary stents has significantly reduced the need for target lesion revascularisation and therefore trials have been initiated comparing stent supported PTCA with CABG in patients with multivessel CAD (ARTS, SOS, ERACI-II). The one year follow up results of ARTS have recently been reported (P Serruys, European Society of Cardiology, Barcelona, 1999) and revealed: (1) a similar incidence of death, MI and stroke; (2) an increased need for additional revascularisation procedures in patients initially treated by coronary stenting, and (3) a cost saving of 4278 Euros during the initial hospitalisation and of 2965 Euros at one year follow up in favour of coronary stenting. The most important finding of ARTS is the reduction by more than half in the need for additional revascularisation procedures in patients undergoing coronary stenting (17%) as compared with the previous PTCA/CABG trials featuring revascularisation rates of 30–40% at one year follow up, confirming the hypothesis that stents improve long term outcome (table 5). An even further improvement of PCI can be predicted by the addition of glycoprotein IIb/IIIa inhibitors to coronary stenting as indicated by the complementary benefit of abciximab and coronary stenting in the EPISTENT trial12(table 1). Compared with coronary stenting alone, the addition of abciximab resulted in improved survival at one year follow up (2.4% stent alone v 1.0% stent plus abciximab, p = 0.04) and an 18% reduction in target vessel revascularisation (10.6% stent alone v 8.7% stent plus abciximab, p = 0.2), which became significant in diabetic patients (16.6% stent alone v 8.1% stent plus abciximab, p = 0.02).
In summary, since there are no major differences in prognosis between the two treatment modalities, in non-diabetic patients with multivessel disease and maintained left ventricular function amenable to both PCI and CABG, the choice of revascularisation method rests on weighing the more invasive nature of CABG against the increased need of additional revascularisation after PCI.
References
Supplementary materials
- Additional references cited in the text for "CORONARY DISEASE: Intervention in coronary artery disease"
Stephan Windecker, Bernhard Meier
Heart 2000;83:481
1 Waller BF. Coronary luminal shape and the arc of disease-free wall: morphologic observations and clinical relevance. J Am Coll Cardiol 1985;6:1100�1.
2 Sanborn TA, Faxon DP, Haudenschild C, et al. The mechanism of transluminal angioplasty: evidence for formation of aneurysms in experimental atherosclerosis. Circulation 1983;68:1136�40.
3 Faxon DP, Sanborn TA, Haudenschild CC. Mechanism of angioplasty and its relation to restenosis. Am J Cardiol 1987;60:5B--9B.
4 Honye J, Mahon DJ, Jain A, et al. Morphological effects of coronary balloon angioplasty in vivo assessed by intravascular ultrasound imaging. Circulation 1992;85:1012�25.
5 Ellis SG, Cowley MJ, Whitlow PL, et al. Prospective case-control comparison of percutaneous transluminal coronary revascularization in patients with multivessel disease treated in 1986�1987 versus 1991: improved in-hospital and 12-month results. Multivessel Angioplasty Prognosis Study (MAPS) Group. J Am Coll Cardiol 1995;25:1137�42.
6 Myler R, Shaw R, Sterzer S, et al. Lesion morphology and coronary angioplasty: current experience and analysis. J Am Coll Cardiol 1992;19:1641�52.
7 Meier B. Balloon angioplasty. In: Topol EJ, ed. Comprehensive cardiovascular medicine. Philadelphia: Lippincott-Raven, 1998:2251�84.
8 Landau C, Lange RA, Hillis LD. Percutaneous transluminal coronary angioplasty. N Engl J Med 1994;330:981�93.
9 Ellis SG, Roubin GS, King SB, et al. Angiographic and clinical predictors of acute closure after native vessel coronary angioplasty. Circulation 1988;77:372�9.
10 Simpfendorfer C, Belardi J, Bellamy G, et al. Frequency, management and follow-up of patients with acute coronary occlusions after percutaneous transluminal coronary angioplasty. Am J Cardiol 1987;59:267�9.
11 Lincoff AM, Popma JJ, Ellis SG, et al. Abrupt vessel closure complicating coronary angioplasty: clinical, angiographic and therapeutic profile. J Am Coll Cardiol 1992;19:926�35.
12 Lincoff AM, Topol EJ. Abrupt vessel closure. In: Topol EJ, ed. Tectbook of interventional cardiology, 3rd edn. Philadelphia: WB Saunders, 1999:163�87.
13 Serruys P, Azar A, Sigwart U, et al. Long-term follow-up of stent-like (<30% diameter stenosis post) angioplasty: a case for provisional stenting. J Am Coll Cardiol 1996;27(suppl):15A.
14 Serruys PW, di Mario C, Piek J, et al. Prognostic value of intracoronary flow velocity and diameter stenosis in assessing the short- and long-term outcomes of coronary balloon angioplasty: the DEBATE study (Doppler endpoints balloon angioplasty trial Europe). Circulation 1997;96:3369�77.
15 Rodriguez A, Ayala F, Bernardi V, et al. Optimal coronary balloon angioplasty with provisional stenting versus primary stent (OCBAS): immediate and long-term follow-up results. J Am Coll Cardiol 1998;32:1351�7.
16 Eeckhout E, Kappenberger L, Goy JL. Stents for intracoronary placement: current status and future directions. J Am Coll Cardiol 1996;27:757�65.
17 Ruygrok PN, Serruys PW. Intracoronary stenting. From concept to custom. Circulation 1996;94:882�90.
18 Holmes DR Jr, Hirshfeld J Jr, Faxon D, et al. ACC expert consensus document on coronary artery stents. Document of the American College of Cardiology. J Am Coll Cardiol 1998;32:1471�82.
19 Serruys PW, van Hout B, Bonnier H, et al. Randomised comparison of implantation of heparin-coated stents with balloon angioplasty in selected patients with coronary artery disease (Benestent II). Lancet 1998;352:673�81.
20 Versaci F, Gaspardone A, Tomai F, et al. A comparison of coronary-artery stenting with angioplasty for isolated stenosis of the proximal left anterior descending coronary artery. N Engl J Med 1997;336:817�22.
21 Erbel R, Haude M, Hopp HW, et al. Coronary-artery stenting compared with balloon angioplasty for restenosis after initial balloon angioplasty. Restenosis stent study group. N Engl J Med 1998;339:1672�8.
22 Savage MP, Douglas JS Jr, Fischman DL, et al. Stent placement compared with balloon angioplasty for obstructed coronary bypass grafts. Saphenous vein de novo trial investigators. N Engl J Med 1997;337:740�7.
23 Suryapranata H, van�t Hof AWJ, Hoorntje JCA, et al. Randomized comparison of coronary stenting with balloon angioplasty in selected patients with acute myocardial infarction. Circulation 1998;97:2502�5.
24 Sirnes PA, Golf S, Myreng Y, et al. Stenting in chronic coronary occlusion (SICCO): a randomized, controlled trial of adding stent implantation after successful angioplasty. J Am Coll Cardiol 1996;28:1444�51.
25 Antoniucci D, Santoro GM, Bolognese L, et al. A clinical trial comparing primary stenting of the infarct-related artery with optimal primary angioplasty for acute myocardial infarction: results from the Florence randomized elective stenting in acute coronary occlusions (FRESCO) trial. J Am Coll Cardiol 1998;31:1234�9.
26 Buller CE, Dzavik V, Carere RG, et al. Primary stenting versus balloon angioplasty in occluded coronary arteries. The total occlusion study of Canada (TOSCA). Circulation 1999;100:236�42.
27 Colombo A, Hall P, Nakamura S, et al. Intracoronary stenting without anticoagulation accomplished with intravascular ultrasound guidance. Circulation 1995;91:1676�88.
28 Schomig A, Neumann FJ, Kastrati A, et al. A randomized comparison of antiplatelet and anticoagulant therapy after the placement of coronary-artery stents. N Engl J Med 1996;334:1084�9.
29 Bauters C, Banos J-L, Van Belle E, et al. Six-month angiographic outcome after successful repeat percutaneous intervention for in-stent restenosis. Circulation 1998;97:318�21.
30 Topol EJ. Caveats about elective coronary stenting. N Engl J Med 1994;331:539�41.
31 Adelman AG, Cohen EA, Kimball BP, et al. A comparison of directional atherectomy with balloon angioplasty for lesions of the left anterior descending coronary artery. N Engl J Med 1993;329:228�33.
32 Topol EJ, Leya F, Pinkerton CA, et al. A comparison of directional atherectomy with coronary angioplasty in patients with coronary artery disease. N Engl J Med 1993;329:221�7.
33 Baim DS, Cutlip DE, Sharma SK, et al. Final results of the balloon vs optimal atherectomy trial (BOAT). Circulation 1998;97:322�31.
34 Holmes DR Jr, Topol EJ, Califf RM, et al. A multicenter, randomized trial of coronary angioplasty versus directional atherectomy for patients with saphenous vein bypass graft lesions. CAVEAT-II investigators. Circulation 1995;91:1966�74.
35 Friedman HZ, Elliott MA, Gottlieb GJ, et al. Mechanical rotary atherectomy: the effects of microparticle embolization on myocardial blood flow and function. J Interv Cardiol 1989;2:77�83.
36 Zotz R, Erbel R, Philip A, et al. High-speed rotational angioplasty-induced echo contrast in vivo and in vitro optical analysis. Cathet Cardiovasc Diagn 1992;26:98�109.
37 Stertzer SH, Pomerantsev EV, Fitzgerald PJ, et al. Effect of technique modification on immediate results of high speed rotational atherectomy in 710 procedures on 656 patients. Cathet Cardiovasc Diagn 1995;36:304�10.
38 Reisman M, Harms V. Guidewire bias: potential source of complications with rotational atherectomy. Cathet Cardiovasc Diagn 1996;37:64�8.
39 Grundfest WS, Segalowitz J, Laudesnlager J, et al. The physical and biological basis for laser angioplasty. In: Litvack F, ed. Coronary laser angioplasty: Blackwell Scientific Publications, 1992:1�12.
40 Mintz GS, Kovach JA, Javier SP, et al. Mechanisms of lumen enlargement after excimer laser coronary angioplasty. An intravascular ultrasound study. Circulation 1995;92:3408�14.
41 van Leeuwen TG, Borst C. Fundamental laser-tissue interactions. Seminars in Interventional Cardiology 1996;1:121�8.
42 van Leeuwen TG, Meertens JH, Velema E, et al. Intraluminal vapor bubble induced by excimer laser pulse causes microsecond arterial dilation and invagination leading to extensive wall damage in the rabbit. Circulation 1993;87:1258�63.
43 van Leeuwen TG, van Erven L, Meertens JH, et al. Origin of arterial wall dissections induced by pulsed excimer and mid-infrared laser ablation in the pig. J Am Coll Cardiol 1992;19:1610�8.
44 Deckelbaum LI. Cardiovascular applications of laser technology. Lasers Surg Med 1994;15:315�41.
45 Deckelbaum LI, Natarajan MK, Bittl JA, et al. Effect of intracoronary saline infusion on dissection during excimer laser coronary angioplasty: a randomized trial. The percutaneous excimer laser coronary angioplasty (PELCA) investigators. J Am Coll Cardiol 1995;26:1264�9.
46 Topaz O. Holmium laser angioplasty. Seminars in Interventional Cardiology 1996;1:149�61.
47 Hamburger JN, Gijsbers GH, Ozaki Y, et al. Recanalization of chronic total coronary occlusions using a laser guide wire: a pilot study. J Am Coll Cardiol 1997;30:649�56.
48 Hirsh J, Fuster V. Guide to anticoagulant therapy. Part 2: oral anticoagulants. Circulation 1994;89:1469�80.
49 Narins CR, Hillegass Jr WB, Nelson CL, et al. Relation between activated clotting time during angioplasty and abrupt closure. Circulation 1996;93:667�71.
50 Boccara A, Benamer H, Juliard JM, et al. A randomized trial of a fixed high dose vs a weight-adjusted low dose of intravenous heparin during coronary angioplasty. Eur Heart J 1997;18:631�5.
51 Garachemani A, Meier B. Heparin for coronary angioplasty: high dose, low dose, or no dose? Heart 1998;80:3�4.
52 Vainer J, Fleisch M, Gunnes P, et al. Low dose heparin for routine coronary angioplasty and stenting. Am J Cardiol 1996;78:964�6.
53 Friedman HZ, Cragg DR, Glazier SM, et al. Randomized prospective evaluation of prolonged versus abbreviated intravenous heparin therapy after coronary angioplasty. J Am Coll Cardiol 1994;24:1214�9.
54 Weitz JI. Low-molecular-weight heparins N Engl J Med 1997;337:688�98.
55 Preisack MB, Bonan R, Meisner C, et al. Incidence, outcome and prediction of early clinical events following percutaneous transluminal coronary angioplasty. A comparison between treatment with reviparin and unfractionated heparin/placebo (results of a substudy of the REDUCE trial). Eur Heart J 1998;19:1232�8.
56 Serruys PW, Herrman JP, Simon R, et al. A comparison of hirudin with heparin in the prevention of restenosis after coronary angioplasty. N Engl J Med 1995;333:757�63.
57 The GUSTO IIb Investigators. A clinical trial comparing primary coronary angioplasty with tissue plasminogen activator for acute myocardial infarction. The global use of strategies to open occluded coronary arteries in acute coronary syndromes (GUSTO IIb) angioplasty substudy investigators. N Engl J Med 1997;336:1621�8.
58 Bittl JA, Strony J, Brinker JA, et al. Treatment with bivalirudin (hirulog) as compared with heparin during coronary angioplasty for unstable or postinfarction angina. N Engl J Med 1995;333:764�9.
59 Urban P, Macaya C, Rupprecht HJ, et al. Randomized evaluation of anticoagulation versus antiplatelet therapy after coronary stent implantation in high-risk patients: the multicenter aspirin and ticlopidine trial after intracoronary stenting (MATTIS). Circulation 1998;98:2126�32.
60 Bertrand ME, Legrand V, Boland J, et al. Randomized multicenter comparison of conventional anticoagulation versus antiplatelet therapy in unplanned and elective coronary stenting. The full anticoagulation versus aspirin and ticlopidine (fantastic) study. Circulation 1998;98:1597�603.
61 Schwartz L, Bourassa MG, Lesperance J, et al. Aspirin and dipyridamole in the prevention of restenosis after percutaneous transluminal coronary angioplasty. N Engl J Med 1988;318:1714�9.
62 Lembo NJ, Black AJR, Roubin GS, et al. Effect of pretreatment with aspirin versus aspirin plus dipyridamole on frequency and type of acute complications of percutaneous transluminal coronary angioplasty. Am J Cardiol 1990;65:422�6.
63 Quinn MJ, Fitzgerald DJ. Ticlopidine and clopidogrel. Circulation 1999;100:1667�72.
64 Topol EJ. Toward a new frontier in myocardial reperfusion therapy: emerging platelet preeminence. Circulation 1998;97:211�8.
65 Schömig A, Neumann FJ, Kastrati A, et al. A randomized comparison of antiplatelet and anticoagulant therapy after the placement of coronary-artery stents. N Engl J Med 1996;334:1084�9.
66 Moussa I, Oetgen M, Roubin G, et al. Effectiveness of clopidogrel and aspirin versus ticlopidine and aspirin in preventing stent thrombosis after coronary stent implantation. Circulation 1999;99:2364�6.
67 The EPIC Investigators. Use of a monoclonal antibody directed against the platelet glycoprotein IIb/IIIa receptor in high-risk coronary angioplasty. The EPIC investigation. N Engl J Med 1994;330:956�61.
68 The CAPTURE Investigators. Randomised placebo-controlled trial of abciximab before and during coronary intervention in refractory unstable angina: the CAPTURE study. Lancet 1997;349:1429�35.
69 The EPISTENT Investigators. Randomised placebo-controlled and balloon-angioplasty-controlled trial to assess safety of coronary stenting with use of platelet glycoprotein-IIb/IIIa blockade. The EPISTENT investigators. Evaluation of platelet IIb/IIIa inhibitor for stenting. Lancet 1998;352:87�92.
70 Brener SJ, Barr LA, Burchenal JE, et al. Effect of abciximab on the pattern of reperfusion in patients with acute myocardial infarction treated with primary angioplasty. RAPPORT investigators. ReoPro and primary PTCA organization and randomized trial. Am J Cardiol 1999;84:728�30, A8.
71 The IMPACT-II Investigators. Randomised placebo-controlled trial of effect of eptifibatide on complications of percutaneous coronary intervention: IMPACT-II. Integrilin to minimise platelet aggregation and coronary thrombosis-II. Lancet 1997;349:1422�8.
72 The RESTORE Investigators. Effects of platelet glycoprotein IIb/IIIa blockade with tirofiban on adverse cardiac events in patients with unstable angina or acute myocardial infarction undergoing coronary angioplasty. The RESTORE investigators. Randomized efficacy study of tirofiban for outcomes and restenosis. Circulation 1997;96:1445�53.
73 Topol EJ, Ferguson JJ, Weisman HF, et al. Long-term protection from myocardial ischemic events in a randomized trial of brief integrin beta3 blockade with percutaneous coronary intervention. EPIC investigator group. Evaluation of platelet IIb/IIIa inhibition for prevention of ischemic complication [[see comments]]. JAMA 1997;278:479�84.
74 Windecker S, Meyer BJ, Bonzel T, et al. Interventional cardiology in Europe 1995. Eur Heart J 1999;20:484�95.
75 Hannan EL, Racz M, Ryan TJ, et al. Coronary angioplasty volume-outcome relationships for hospitals and cardiologists. JAMA 1997;277:892�8.
76 Jollis JG, Peterson ED, DeLong ER, et al. The relation between the volume of coronary angioplasty procedures at hospitals treating medicare beneficiaries and short-term mortality. N Engl J Med 1994;331:1625�9.
77 Jollis JG, Peterson ED, Nelson CL, et al. Relationship between physician and hospital coronary angioplasty volume and outcome in elderly patients [[see comments]]. Circulation 1997;95:2485�91.
78 Ellis SG, Weintraub W, Holmes D, et al. Relation of operator volume and experience to procedural outcome of percutaneous coronary revascularization at hospitals with high interventional volumes [[see comments]]. Circulation 1997;95:2479�84.
79 Pitt B, Waters D, Brown WV, et al. Aggressive lipid-lowering therapy compared with angioplasty in stable coronary artery disease. Atorvastatin versus revascularization treatment investigators. N Engl J Med 1999;341:70�6.
80 Goy JJ, Eeckhout E, Moret C, et al. Five-year outcome in patients with isolated proximal left anterior descending coronary artery stenosis treated by angioplasty or left internal mammary artery grafting. A prospective trial. Circulation 1999;99:3255�9.
81 Hamm CW, Reimers J, Ischinger T, et al. A randomized study of coronary angioplasty compared with bypass surgery in patients with symptomatic multivessel coronary disease. N Engl J Med 1994;331:1037�43.
82 King SB, III, Lembo NJ, Weintraub WS, et al. A randomized trial comparing coronary angioplasty with coronary bypass surgery. N Engl J Med 1994;331:1044�50.
83 CABRI Trial Participants. First-year results of CABRI (coronary angioplasty versus bypass revascularisation investigation). Lancet 1995;346:1179�84.
84 Rodriguez A, Mele E, Peyregne E, et al. Three-year follow-up of the Argentine randomized trial of percutaneous transluminal coronary angioplasty versus coronary artery bypass surgery in multivessel disease (ERACI). J Am Coll Cardiol 1996;27:1178�84.
85 Henderson RA, Pocock SJ, Sharp SJ, et al. Long-term results of RITA-1 trial: clinical and cost comparisons of coronary angioplasty and coronary-artery bypass grafting. Randomised Intervention treatment of angina. Lancet 1998;352:1419�25.