Article Text

Statistics from Altmetric.com
In seeking an imaging solution to the limitations of standard exercise stress testing, echocardiography is attractive on practical grounds. It is the most widely disseminated and inexpensive technique for non-invasive imaging of the heart. It is “patient friendly” because it is rapidly performed, and is highly versatile, being usable in a variety of environments. In combination with various stressors, echocardiography provides a means of identifying myocardial ischaemia by detection of stress induced wall motion abnormalities.
Indeed, an impressive clinical evidence base matches these theoretical benefits. The accuracy of stress echocardiography for detection of significant coronary stenoses ranges from 80–90%, exceeding that of the exercise ECG (especially in women and patients with left ventricular hypertrophy), and being comparable to that of stress myocardial perfusion scintigraphy. Stress echocardiography is a powerful prognostic tool in chronic coronary disease, after myocardial infarction, and in evaluation of patients before major non-cardiac surgery. It is an accurate test for prediction of functional recovery of dyssynergic zones after revascularisation, and also provides valuable physiologic information in patients under consideration for valve surgery.
Unfortunately, however, the disadvantages of the technique are not trivial. Advances in imaging and image processing have solved most—but not all—problems of image quality. Test interpretation remains very much in the eye of the beholder. The only mainstream marker of ischaemia is abnormal wall motion, and the need to induce ischaemia in the metabolic sense limits the accuracy of stress echocardiography in detecting coronary artery disease in patients who exercise submaximally or who are on antianginal treatment.
This article reviews the methodology and the favourable and unfavourable aspects of stress echocardiography. Technological advances in ultrasound and digital technology are likely to refine further the technique and move from a simple test of wall motion to portraying local contractile behaviour and perfusion. The automation of these processes will realise the vision of stress echocardiography as the stress imaging test of choice.
PATHOPHYSIOLOGY
Exercise and inotropic stress normally provoke a generalised increase of regional wall motion and thickening, with an increment of ejection fraction mainly caused by a reduction of systolic dimensions. Regional systolic dysfunction is usually caused by coronary artery disease, but cardiomyopathies may also show regional variation in function.1 Resting wall motion abnormalities are the hallmark of prior myocardial infarction, but do not necessarily imply that the segment is non-viable. The presence of residual viable tissue is more common in hypokinetic than akinetic segments, and least common in dyskinetic segments. However, hypokinesis may also imply non-transmural infarction, and even perfusion data or the dobutamine response may not solve this ambiguity.
Ischaemia is typically manifest as new or worsening wall motion abnormalities, delayed contraction, or (if severe) the development of left ventricular enlargement or a decrease in ejection fraction. Regional systolic changes generally precede the development of ST segment changes and chest pain, but follow the initial development of abnormalities of diastolic function and regional malperfusion. The presence of inducible wall motion abnormalities implies a significant limitation of bloodflow at peak stress, and usually corresponds to a stenosis of > 50% diameter, although the anatomic severity and physiologic consequences are poorly related. The provocation of ischaemia in the setting of relatively mild coronary stenoses is dependent on the performance of maximal stress. Inducible wall motion abnormalities often recover rapidly after stress, but may be persistent if ischaemia is severe and stunning is induced.
METHODOLOGY
Stress testing
Patients who are able to exercise should undergo exercise stress testing, which can be performed on the treadmill with images obtained within one minute of the conclusion of exercise imaging—although upright images may be performed immediately in some patients. Upright or supine cycle exercise permits imaging during exercise, which permits assessment of the ischaemic threshold and avoids the possibility of resolution of ischaemia between the end of exercise and the start of imaging—which may reduce sensitivity.
The primary indications for pharmacologic stress are inability to exercise or the desire to identify viable myocardium. Dobutamine infusion to a peak dose of 40 μg/kg/min is the most commonly used pharmacologic stressor, and increases myocardial oxygen consumption through increments in inotropic state, heart rate (usually to 120–140 beats/minute), and blood pressure (by 30–40 mm Hg with peak pressures of 170–180 mm Hg). Serious complications occur in about 3:1000.
Vasodilator agents (adenosine to 0.18 mg/kg/min and dipyridamole to 0.84 mg/kg) are less commonly used for pharmacologic stress echo, and work by the induction of coronary steal, which occurs in the setting of severe or extensive coronary disease. The haemodynamic effects of these stressors are minor, and the most common side effects of dipyridamole and adenosine are headache and dyspnoea, respectively; serious side effects occur in about 1:1000 patients. Atropine may be added if the response to dipyridamole is negative, and other protocols involve combination of dobutamine with a vasodilator.
The selection of non-exercise stress is mostly determined by local experience and sometimes cost. For diagnostic indications, the sensitivity of dobutamine echo is somewhat greater, especially in patients with single vessel disease. From a prognostic angle, both pharmacologic tests are supported by a strong evidence base. Side effects occur with similar frequency with dipyridamole and dobutamine, although serious problems are more likely with dobutamine. Dobutamine stress is a better choice for those with asthma or untreated conduction system disease, while dipyridamole stress is preferable in patients with serious arrhythmias or severe hypertension.
Imaging techniques
A screening exam with M mode and limited Doppler should be performed at the start of the test, but a detailed echo examination is usually not feasible from a logistic standpoint. Stress echo is almost universally performed using transthoracic imaging, usually with harmonic imaging and usually in the two parasternal and three apical views. Transoesophageal imaging is occasionally used in the setting of poor image quality, but has been superceded by use of contrast agents for left ventricular opacification.
Digital imaging is very important for stress echo—mostly for side-by-side comparison of regional function at rest and stress, as well as the ability to review the progression of contraction on a frame-by-frame basis (which facilitates assessment of the timing of contraction). However, because of the ability to store non-standard views and multiple cardiac cycles on videotape, review of the videotape is sometimes still of value.
Interpretation of stress echocardiography
The standard approach to interpretation is qualitative. The attendant need for training2 and problems posed for reproducibility of the test are the greatest shortcomings of this technique.3 Visual assessment is based on analysis of thickening (rather than motion, which may be influenced by translation or tethering) before, during, and after stress. Table 1 summarises the criteria to identify ischaemia, viability, and scar. A systematic approach to review is essential. First, images are examined to assess their quality and the presence of technical limitations. On the resting images, global function is assessed by calculation of wall motion score index or ejection fraction, and regional function is evaluated using regional wall motion scoring. Rest and stress images are then compared for the development of global dysfunction (left ventricular enlargement and shape changes) and regional dysfunction. A normal response involves the augmentation of function in all segments (video sequence 1). The presence of a new or worsening wall motion abnormality identifies ischaemia (video sequence 2), but rather than identifying the test as simply positive, the site, extent, and severity of abnormal function should be identified, as well as the ischaemic threshold if a bicycle or dobutamine stress study is being examined.
Interpretation of exercise and pharmacologic stress echocardiography
A quantitative approach may be able to address some of the limitations of the qualitative approach, and a number of techniques for the measurement of radial or longitudinal function have been studied (table 2). Unfortunately, there is no easy solution to the need to quantify regional function—the problem being complicated by issues of translational motion, tethering, torsional movement, image quality, and so on. The main quantitative approaches include the centreline technique or automated border recognition methods (both measures of radial excursion), and longitudinal velocity, displacement or strain (measured by tissue Doppler).
Quantitative techniques for the evaluation of stress echocardiography
DIAGNOSTIC APPLICATION
Indications
Like other stress imaging tests, the chief indications for stress echo are patients who either cannot exercise or exercise submaximally (who should undergo pharmacologic stress) and patients with an uninterpretable ECG caused by repolarisation abnormalities (who should undergo exercise echo). The latter group may be supplemented by other subgroups among whom the exercise ECG is suboptimal.
Accuracy of stress echocardiography
The accuracy of stress echo tests for the detection of coronary artery disease is expressed as the sensitivity and specificity of the technique for the detection of angiographically demonstrated stenoses. Nonetheless, this parameter has a number of limitations, some reflecting the limitations of an angiographic cutoff for significant disease, including the variation of the physiologic effect of a stenosis based on site, length, and vessel size, as well as over- and underestimation of coronary lesion severity.4 Populations with a high prevalence of multivessel coronary disease and previous myocardial infarction are more likely to develop ischaemia in response to stress, and referral bias may also influence the recorded accuracy. As stress echo is dependent on the induction of ischaemia, the adequacy of stress has a pivotal influence on sensitivity. Finally, accuracy will be influenced by echocardiographic factors including image quality and left ventricular morphology; the lateral wall is a frequent site of false negatives and the inferior wall for false positives. Causes of false positive and negative tests are listed in table 3.
Causes of false negative and false positive stress echocardiograms
In significant studies of exercise echocardiography (> 100 patients), the sensitivity and specificity range from 74–97% and 64–86%, respectively (fig 1). Higher sensitivity may be obtained with bicycle exercise (as there is no loss of ischaemia in the post-stress period), but this is at the cost of some impairment in specificity. Comparisons with quantitative angiography have shown stenosis diameters of 0.7–1.0 mm to be associated with ischaemia.

Summary of the mean, high, and low values for sensitivity and specificity in studies of > 100 patients with exercise (ExE), dobutamine (DbE), and dipyridamole stress echo (DpyE).
Significant studies (> 100 patients) of dobutamine stress echocardiography show a range for sensitivity of between 61–95%, while that for specificity ranged from 51–95% (fig 1). The increment in cardiac workload is less with dobutamine than exercise, and sensitivity can be compromised if workload is reduced by medical treatment or dose limiting side effects. The addition of atropine augments sensitivity. Dobutamine echocardiography is a more sensitive marker of ischaemia in lesions involving larger (> 2.6 mm diameter) vessels than smaller vessels. The quantitative angiography parameters associated with ischaemia are a lumen diameter of < 1 mm diameter, per cent diameter stenosis of 52%, and per cent area stenosis of 75%, of which the minimal lumen diameter is most predictive of an abnormal dobutamine stress test.
The sensitivity and specificity of dipyridamole and adenosine stress echocardiography for the detection of coronary artery disease range from 61–81% and 90–94%, respectively (fig 1). Some studies with these techniques have included populations with a high prevalence of extensive coronary disease or prior infarction—both of which are associated with a high sensitivity. However, single vessel disease is more difficult to detect using this technique.
Limitations in the diagnostic use of stress echocardiography
Although the presence of coronary artery disease is readily recognised in the setting of multivessel disease, and multivessel pathology is readily recognised in the presence of prior infarction (“ischaemia at a distance”), the technique has a sensitivity of only 50% for the recognition of multivessel disease in normal ventricles. The development of global ventricular dysfunction (reduction of ejection fraction or left ventricular enlargement) should increase the interpreter’s suspicion of multi-vessel disease, although it may reflect loss of contractile reserve in valvar heart disease (video sequence 3). Clues to the presence of extensive disease despite apparently localised wall motion abnormalities include the early onset of ischaemia, at a low heart rate and rate–pressure product, or at a low dose of pharmacologic stressor.
The detection of single vessel stenoses may also be problematic, and the sensitivity of stress echo for this problem is probably less than that of myocardial perfusion scintigraphy. This reflects the need for ischaemia to involve a significant extent of myocardium in order for the stress echocardiogram to be positive—which may not be fulfilled if the involved vessel is small or distal, or the stenosis only mildly flow limiting.
Because of problems posed by identification of minor gradations of wall motion in the setting of abnormal function, the identification of ischaemia within areas of resting wall motion abnormalities may be difficult. The problem is probably less during dobutamine stress because ischaemic segments with abnormal resting function often show a biphasic response.
The last three issues reflect fundamental limitations of an ischaemia based technique,5 which will require either a more sensitive tool for assessment of wall motion, or combination with a perfusion marker such as contrast echocardiography. At present, however, the best way to approach them is to focus on the prognostic, rather than the diagnostic, implications of the test.
PROGNOSTIC EVALUATION
Stress echo techniques offer valuable prognostic information in the risk evaluation of stable chronic coronary artery disease, after myocardial infarction, in left ventricular dysfunction, and in patients undergoing major non-cardiac surgery. Each of these indications has their own evidence base but the principles of risk evaluation are the same.
-
Stress echo data are most useful when risk has been allocated on clinical grounds; age, diabetes, prior coronary events, and heart failure are typical markers of clinical risk. Inability to exercise is a powerful marker of a high risk patent. This selection process is absolutely critical in the appropriate selection of patients for preoperative testing—for example, using Eagle’s criteria for assigning the risk of a cardiac event. Patients with none of these factors (diabetes, age > 70 years, angina, myocardial infarction or heart failure) have a negligible risk of cardiac complications, irrespective of the results of stress testing.6
-
A normal stress echo carries a very low risk (< 1% per year) of major events in the subsequent 4–5 years.7 The warranty of a negative test is less in patients with disease associated with accelerated atherogenesis (for example, diabetes, chronic renal impairment).
-
A positive test carries a 10–30% risk of a perioperative event or a spontaneous event in the subsequent years. Patients should be substratified on the basis of their clinical risk level, other stress data (for example, exercise capacity, haemodynamic responses to exercise, and the ST segment response), ischaemic threshold, and type and extent of abnormal wall motion. It is reasonable to combine with clinical data because the stress data are not only independent but also incremental to the information obtained clinically.8,9
Both preoperative and post-infarct risk stratification studies have been addressed predominantly with pharmacologic stress, which appears be at least as useful for prognosis as does exercise stress. Indeed, because dipyridamole and dobutamine leads to a smaller increment of cardiac workload than dobutamine, these agents are attractive for stress testing early after infarction.
IDENTIFICATION OF MYOCARDIAL VIABILITY
Early after infarction (especially after thrombolysis) myocardium may demonstrate reversible dysfunction related to stunning. In this situation, dobutamine echo may predict the spontaneous recovery of regional functional recovery at follow up. The more critical issue, however, is to identify tissue that will likely recover after revascularisation. Pharmacologic stress echo (mainly dobutamine echo but also dipyridamole) has been shown to be effective for the prediction of myocardial viability in this group of patients, possibly because recurrent episodes of myocardial stunning are an important source of viable tissue late following infarction. In these studies, the sensitivity of dobutamine stress to identify an improvement of systolic function in response to revascularisation ranged from 69–86%, with a range of specificity from 57–100%.
Steps in the prognostic application of stress echocardiography: key points
-
Normal test result is generally associated with low risk (events <1% per year)
-
In a positive test, risk is determined by
-
– extent
-
– nature (scar/ischaemia)
-
– ischaemic threshold
-
– combination with treadmill score
The literature regarding the prediction of myocardial viability is based on comparison with recovery of regional left ventricular function, but the likelihood of improving ejection fraction, functional capacity, and quality of life are the important factors that would help decision making regarding revascularisation in patients with left ventricular dysfunction. The response to revascularisation is dependent on a number of non-echocardiographic variables, including the adequacy of revascularisation of target vessels, the overall status of the ventricle (very large ventricles are unlikely to recover dramatically), and the extent of scar tissue (thinned tissue is unlikely to recover). In fact, a large amount of viability (> 25% of the left ventricle) is needed to predict a 5% improvement of ejection fraction10—another useful marker is a 5% improvement of ejection fraction at low dose dobutamine. Extensive viable myocardium has also been associated with improvement in exercise capacity and increased functional class after revascularisation.
Viable myocardium is prognostically important; medical treatment of such patients is associated with adverse outcome, and revascularisation improves survival in patients with viable tissue. This effect is most likely mediated through the increment of ejection fraction after revascularisation and appears related to the extent of viable tissue.11
USE IN NON-CORONARY HEART DISEASES
The functional response to stress is important in the evaluation of myocardial and valvar heart diseases, although this has been outweighed by the application in ischaemic heart disease. Subclinical left ventricular dysfunction (for example, anthracycline toxicity) may become apparent during stress while resting function is still normal. Similarly, loss of contractile reserve is a marker of impending contractile dysfunction in patients with left ventricular volume loading caused by regurgitant valves (video sequence 3).12
Tricuspid regurgitant velocity may be used to calculate pulmonary artery pressure after exercise. This parameter may be abnormal in patients with apparently moderate mitral stenosis at rest who have pronounced exercise limitation, and may also be seen in early pulmonary vascular disease.
The response to stress in patients with stenotic valve lesions may differentiate the relative contribution of the stenosis and ventricular function to the patient’s symptoms. For example, in low gradient aortic stenosis, lack of a response of reduced ventricular function to dobutamine signifies that the patient is unlikely to respond to intervention.13 In those that do respond, an increment in valve gradient with dobutamine implies the stenosis to be the main contributor to a low output state.
COMPARISON WITH OTHER TECHNIQUES
Diagnostic testing
The selection criteria for stress echo include those who are able to exercise but have a non-diagnostic ECG. However, if the echo test is applied in other groups, exercise echo nonetheless has benefits in both sensitivity and specificity. However, it would be financially and logistically impossible to replace diagnostic exercise testing with imaging. If such a replacement were to be considered, it would have to be focused on groups where the ECG is least reliable—such as women,14 patients with hypertensive heart disease or suspected left ventricular hypertrophy, and patients with previous revascularisation.
Perfusion scintigraphy is the main diagnostic alternative to stress echo, and this technique has a sensitivity > 90% for the detection of coronary artery disease. Previous reports of a specificity of 70% partly reflect the phenomenon of post-test referral bias, and the problems of false positives related to image artefacts have likely been reduced by recent developments including gated single photon emission computed tomography (SPECT). Review of both techniques in recent meta-analyses show that the superior sensitivity of SPECT is balanced by a greater specificity with echocardiography, so that the accuracy of the techniques was comparable.15 A number of large studies have compared the results of stress echocardiography and perfusion scintigraphy in the same patients, using various stressors.
Comparisons of exercise and dobutamine stress have shown that the sensitivity of perfusion scintigraphy is slightly better, reflecting the superiority of perfusion imaging (which does not require the development of ischaemia in a metabolic or functional sense) for the identification of patients with single vessel disease. For similar reasons, patients being treated with antianginal agents may be better studied using perfusion scintigraphy, than stress echocardiography. Perfusion scintigraphy appears to be significantly more sensitive for the recognition of multivessel disease, and for the detection of ischaemia in the setting of resting wall motion abnormalities, in which circumstance the recognition of worsening wall motion may be difficult. Finally, scintigraphy can be expected to be superior in patients with poor echocardiographic windows—for example, caused by pulmonary disease.
Stress echocardiography versus perfusion imaging: key points
-
Diagnostic testing
-
– similar accuracy in meta-analyses and head-to-head studies
-
– stress echo less sensitive for mild disease
-
– stress echo more specific, especially with left ventricular hypertrophy
-
Prognostic evaluation
-
– similar prognostic implications of a negative test
-
– limited head-to-head studies showing similar efficacy
-
Detection of myocardial viability
-
– stress echo less sensitive for prediction of recovery
-
– stress echo more specific
Echocardiography has shown persistent superiority with respect to specificity, especially in patients with left ventricular hypertrophy16 and left bundle branch block. Breast attenuation artefacts and other issues have led to lower reported levels of accuracy of perfusion imaging in women, and the results of a meta-analysis suggest that women may be better studied with stress echocardiography. Finally, stress echocardiography is versatile, rapidly performed, and less expensive than perfusion imaging. In situations where other cardiac problems are present as well as ischaemia (for example, valvar or pericardial diseases), the selection of stress echocardiography avoids duplicate testing. However, the most important factor in the decision of which test to select is local expertise.
Strengths and weaknesses of stress echocardiography: key points
-
Strengths
-
– “patient friendly”, versatility
-
– accuracy
-
– prognostic value
-
– detection of viable myocardium after infarction
-
– assessment of left ventricular reserve (for example, valvar heart disease)
-
Weaknesses
-
– dependence on image quality
-
– subjectivity, need for an expert reader
-
– dependence on ischaemia (hence problems with mild disease, submaximal stress, and testing on treatment)
-
– recognition of ischaemia with resting wall motion abnormalities
-
– recognition of multivessel disease
Prediction of events
The implications of a negative test (yearly event rate < 1%) are similar in separate studies of stress echo and SPECT, but these findings may be influenced by the nature of the patients referred for each test. The findings are also analogous with respect to positive test results. Unfortunately, only limited head-to-head comparisons are available regarding the ability of these tests to predict events, but these data suggest that the techniques are comparable and that one does not provide additive data to the other.17
Identification of viable myocardium
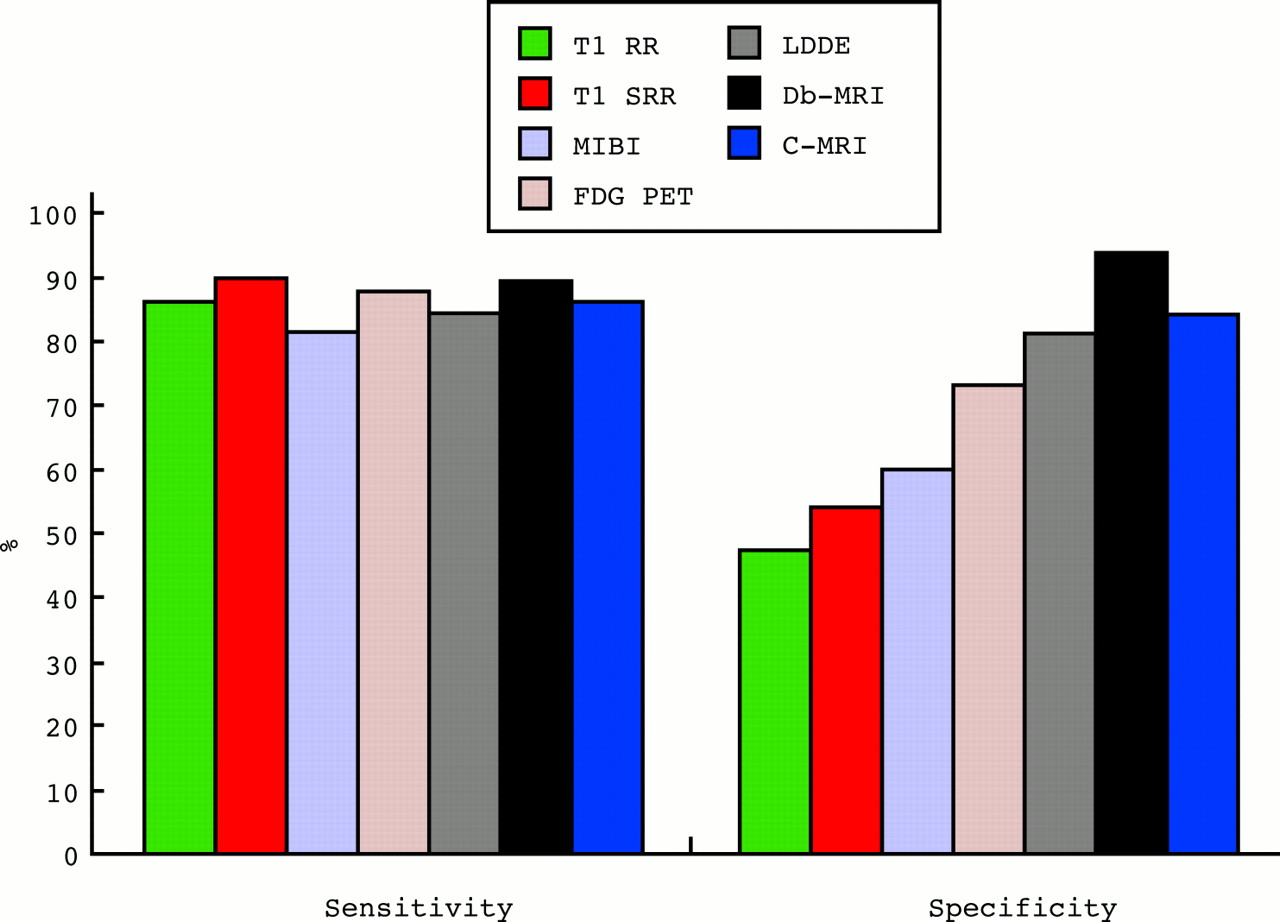
The prediction of recovery of regional function by dobutamine echo and other techniques has been compared in meta-analyses (fig 2)18 and by direct comparison in individual patients. Both analyses suggest that the accuracy of the common non-invasive tests are similar, with stress echocardiography being a little less sensitive but rather more specific than the competing modalities. Stress imaging with magnetic resonance imaging (MRI) has shown similar accuracy to echocardiography both for identification of ischaemia and assessment of viable myocardium, with a benefit for MRI in the setting of technically difficult echo studies. There are limited data available to permit comparison of stress echo with the newer MRI techniques such as late enhancement.
{kind=link}
{kind=link}
Sensitivity and specificity of thallium rest redistribution (Tl RR), thallium stress-rest reinjection (Tl SRR), Tc-99m sestamibi (MIBI), positron emission tomography (FDG PET), low dose dobutamine echocardiography (LDDE), dobutamine MRI (Db-MRI), and contrast enhanced MRI (C-MRI) for the prediction of viability (defined as recovery of regional function after revascularisation). Modified from Bax et al,17 Kim et al, N Engl J Med 2000;343:1445–53, and Baer et al, J Am Coll Cardiol 1998;31:1040–8.
CONCLUSIONS
Stress echocardiography is a versatile tool that derives physiologic information about the presence, site, and extent of ischaemia from regional wall motion responses to stress, and has provided from these data diagnostic and prognostic information in a variety of disease states. The weakness of this tool is that its use by the occasional user (rather than its published evidence base in the hands of experts) may be attended with loss of accuracy. Therefore, the future of this technique will be determined by the development of better training, and technical developments such as myocardial Doppler and contrast echocardiography will address situations where stress echo has insufficient sensitivity as well as increasing quantitation.19,20
REFERENCES
Supplementary materials
Stress echocardiography
Thomas H Marwick
Video Sequences
Video Clip 1
Figure 1: Normal exercise echocardiogram including parasternal (1a), apical 4- and 2-chamber (1b) and apical long axis views (1c). Resting images (left) are compared with post-stress images (left). All segments show augmentation of wall motion and thickening and there is a reduction of LV volume and increment of ejection fraction with stress. Parasternal images are of excellent quality. Although the apical images are of imperfect quality, these are still sufficient for interpretation.
[View Clip 1a] [View Clip 1b] [View Clip 1c]
File Sizes: 1.52MB, 1.67MB, 751KBVideo Clip 2
Figure 2: Exercise echocardiogram (same orientation as figure 1) showing inducible wall motion abnormality in the distal anterior and lateral walls. The parasternal images show no evidence of ischemia in the posterior wall, making the changes more likely due to diagonal than circumflex vessel disease.
[View Clip 2a] [View Clip 2b]
File Sizes: 1.41MB, 1.46MBVideo Clip 3
Figure 4: Loss of contractile reserve in the presence of severe valvular regurgitation and normal resting function. The LV volumes after stress (right) are larger than at rest. As end-diastolic volume increases less than end-systolic volume, this corresponds to a decrement in ejection fraction, signifying decompensation of LV function with stress.
[View Clip]
File Size: 921KB
Linked Articles
- Miscellanea