Article Text

Statistics from Altmetric.com
Heart failure is a common disorder that is associated with significant morbidity, mortality and financial burden to healthcare services. In the UK, around 900 000 people have been diagnosed with heart failure and the prevalence of the condition increases as the population ages.w1 Population-based studies suggest that heart failure carries a worse prognosis than breast and colon cancer, with estimates suggesting a 1 year mortality of 40% from the time of diagnosis. Heart failure currently accounts for a total of one million inpatient bed days and admissions are projected to rise by 50% over the next 25 years. Heart failure treatment currently absorbs 1.8% of the total National Health Service budget, of which 70% is spent on hospitalisation.
Accurate diagnosis, assessment and risk stratification of such patients by imaging modalities is important, particularly with the advent of effective but expensive implantable devices. In the last 5 years, there have been tremendous advances in the ability of cardiovascular magnetic resonance (CMR) to fulfil many of these needs and provide a comprehensive assessment.1 A combination of hardware and software developments means that a modern CMR scanner is able to yield information on myocardial anatomy, function, tissue characterisation, viability, perfusion and flow within a single 45–60 min study.
HOW DOES CMR WORK AND WHAT INFORMATION CAN IT PROVIDE?
Basic principles
Understanding the way in which CMR works provides a basis for appreciating its role in evaluating patients with heart failure. CMR yields high contrast and high resolution images of the heart by mapping radio wave signals absorbed and emitted by hydrogen nuclei (protons) in a powerful magnetic field. Most cardiovascular pathologies manifest with an increase in water content which is rich in protons so that CMR is a sensitive guide to early disease states. CMR is currently mainly performed at a magnetic field strength of 1.5 Tesla (T). The two main types of sequences used are gradient echo and spin echo imaging techniques. Gradient echo techniques lead to blood and fat both appearing white. They enable the acquisition of cine images with a high temporal and spatial resolution that can be used to identify myocardial function and abnormal flow patterns. Velocity mapping is based on gradient echo and can be used in a similar way to two-dimensional Doppler or provide multidimensional flow imaging for complex flow dynamics problems. Based on the different relaxation properties of tissues such as fat, muscle, and areas of inflammation, a range of sequences can be used to enable tissue characterisation. T1-weighted spin echo techniques lead to blood appearing black, while fat appears white. They are useful for high resolution anatomical as opposed to functional imaging. T2-weighted spin echo sequences contain a water excitation pulse that can be used to highlight myocardial inflammation or oedema. Valvular function can be assessed both qualitatively from cine imaging as well as quantitatively from phase contrast velocity mapping with accurate measurements of peak velocity and regurgitant volumes.
While most image acquisition is performed without the routine need for contrast agents, an important development has been the use of gadolinium-chelated contrast agents (Gd-CA), such as Gd-DTPA (gadolinium diethylenetriamine penta-acetic acid), to document perfusion defects, microvascular ischaemia and areas of scar tissue/fibrosis. Gd-CA has paramagnetic properties and thus gives a bright signal on scanning. It is metabolically inert and safe to administer via a peripheral line as a single bolus with a negligible risk of nephrotoxicity, although it is best avoided in patients with severe renal impairment. Due to its chemical properties and large molecular size, Gd-CA is unable to penetrate the intact myocyte membrane. However, it can passively diffuse and accumulate into the extracellular space around muscle cells or into myocytes where the cell membrane has been ruptured. The typical dose given is 0.1–0.2 mmol/kg (usually between 12–40 ml).
Following administration, there are three phases. In the very early phase (first 60 s) Gd-CA will penetrate all myocardial segments with a normal blood supply. These areas will hyperenhance. By contrast, segments with an impaired blood supply, due to either coronary stenosis or microvascular ischaemia, will appear dark (hypoenhanced). This property can be used to assess myocardial perfusion when performed at rest and with adenosine stress. In the next phase (1–3 min), Gd-CA will wash out of normal myocardium but fail to penetrate areas of microvascular obstruction (post-acute infarction). Depending on the dose, by 10–15 min, a third “late” steady-state phase is reached where very little Gd-CA is present in healthy myocardium but has accumulated in areas of replacement scar tissue/fibrosis containing a collagenous matrix, due to the higher volume of distribution and slower washout kinetics. In these regions, its paramagnetic properties result in a bright signal on specialised T1-weighted inversion recovery scans, while the signal from normal myocardium has been “nulled” and appears black. This has led to the maxim that “bright is dead”.2 There is excellent subendocardial resolution of the late gadolinium enhancement (LGE) CMR technique to detect scar tissue with a spatial resolution of 1 g of myocardium.3
More recently, T2-weighted spin echo sequences such as STIR (short tau-inversion recovery) have been validated in identifying myocardial inflammation or oedema that may accompany scarring both in acute infarction and myocarditis.4,5
CMR does not involve the use of ionising radiation and is a very safe technique.
PRACTICAL ASPECTS
A typical CMR examination can be performed on an outpatient basis in 30–45 min. There is no preparation required beforehand. Most patients, including those in New York Heart Association (NYHA) functional class III and IV, are able to undergo a detailed assessment with minimal discomfort. Patients should continue on their normal medications unless a perfusion scan is to be performed, when β-blockers are withheld for 24 h.
LIMITATIONS OF CMR
The presence of a pacemaker/implantable cardioverter-defibrillator (ICD) is still a strong contraindication to performing CMR. This is likely to change as MR compatible devices are developed. Importantly, coronary artery stents, all prosthetic mechanical valves, sternal clips and prosthetic joints are not contraindications.
Valvular and diastolic function is presently better assessed by echocardiography. For optimal image acquisition, a patient should be in sinus rhythm. However, diagnostically useful information can be obtained in patients with rate controlled atrial fibrillation and occasional ectopics. In approximately 2% of patients, claustrophobia may be a problem. However, reassurance and a small dose of an anxiolytic is often enough to permit image acquisition. The lack of portability and access, particularly compared to echocardiography, remain important issues. Further work is underway to determine the sensitivity and specificity of CMR in early detection of aetiologies and in comparative trials with other imaging modalities.
ASSESSMENT OF FUNCTION
Accurate quantitative measurement of left and right ventricular volumes and function is the mainstay of initial diagnosis for the patient with suspected heart failure, particularly in borderline cases. CMR is the gold standard for measurement of cardiac parameters. A stack of 9–10 contiguous breath-hold, retrospectively-gated, short-axis cine slices of the left (LV) and right (RV) ventricles is obtained from the base to apex. Planimetry of the endocardial and epicardial borders (summation of disks method) is used to derive the LV and RV end-systolic and diastolic volumes, and also the ejection fraction and myocardial mass. There is excellent reproducibility of measurements so that serial assessment—for example, to assess therapeutic response—is facilitated.6 Diastolic function can be assessed from the short axis stack by determining the peak filling rates and time–volume curves and also from the long axis motion and left atrial dimensions. Multiplanar images are obtained with no geometrical assumptions made, which is important in patients with heart failure where the LV is often abnormally shaped. Reflecting these strengths is the growing number of trials using CMR derived volumetric parameters as the primary end-point where the better accuracy and interstudy reproducibility result in a lower requisite sample size than using other imaging modalities.w2–4 In patients experiencing difficulty holding their breath, a navigator-based respiratory gating technique can be used to obtain the necessary images.w5 Patients with arrhythmias, including atrial fibrillation, may require real-time imaging which provides sufficient resolution to deliver clinically useful cine images.w6
Regional assessment of segmental wall motion, including radial and circumferential strain patterns, can be assessed by measuring the deformation of applied grid tags during the cardiac cycle.
DIAGNOSIS OF AETIOLOGY
Left ventricular dysfunction secondary to coronary artery disease
The main current clinical applications of CMR in this group are assessment of anatomy, function, amount of hibernating myocardium, and myocardial perfusion. Cine imaging will provide information on global function and regional motion. Areas of thinning and the complications of infarction such as aneurysm formation can be easily seen due to the wide field of view. T2-weighted imaging is useful in the acute infarct setting to assess for active inflammation.7
Assessment of viability
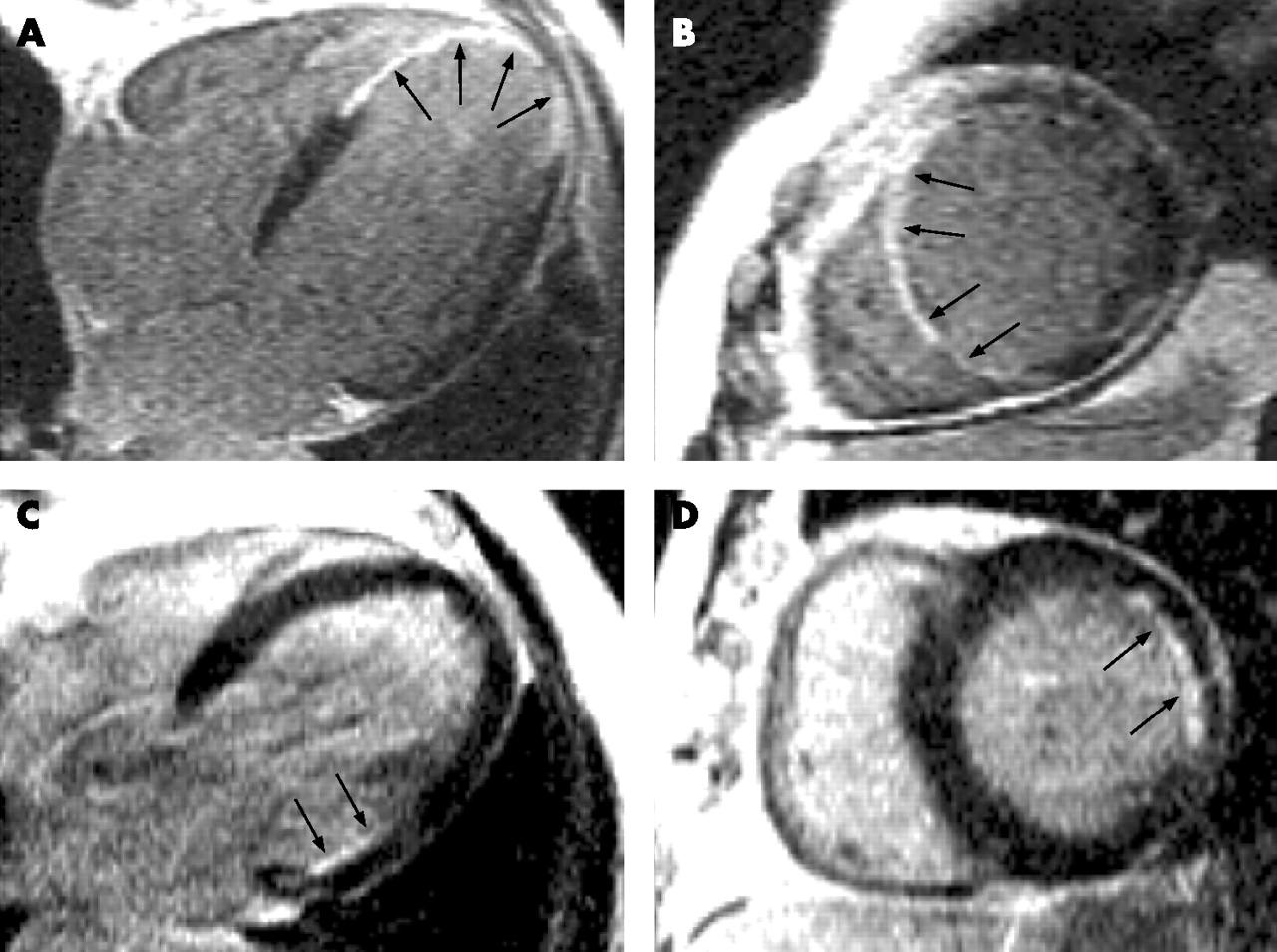
Post-infarction, the region of myocardium most vulnerable to scarring is the subendocardium as this is the most distal from the epicardial coronary artery. Thus following administration of Gd-CA, there is LGE of scar tissue that always involves the subendocardium. Depending on the extent and duration of ischaemia, the necrotic processes will spread transmurally towards the epicardium in a region subtended by the diseased coronary artery(ies). The degree of infarction can be easily and accurately quantified by LGE in both absolute terms and also as the relative transmural extent per segment (fig 1⇓).

Transmural versus subendocardial myocardial infarction. Panels A and B (four chamber and apical short axis views, respectively) show a patient with transmural myocardial infarct in the apical left ventricle (LV) on late gadolinium enhancement (LGE) images. The arrows delineate the bright white signal in the apical LV reflecting transmural myocardial infarction with no viable myocardium. Revascularisation would not result in improved function of the apical LV. Panels C and D (four chamber and short axis views, respectively) show a patient with a limited basal lateral wall subendocardial infarction. The arrows delineate an area of bright signal involving 25–50% of the myocardial wall (viable myocardial is nulled to appear black). Revascularisation of an appropriate target lesion would be expected to result in improved function of the affected segments.
In a seminal study by Kim et al, the transmural extent of infarction as determined by LGE was shown to correlate with the likelihood of functional recovery of the affected tissue at 6 months post-revascularisation.8 Areas of hypokinesia with subendocardial infarction less than 25% of transmural extent have up to an 80% likelihood of functional improvement. By contrast, hypokinetic segments with myocardial infarction involving over 50% of the wall thickness have a low probability of recovery. LGE can therefore be used to provide a detailed topographical map of myocardial viability and hibernation to clinicians, based on the “mismatch” between the transmurality of LGE seen and the degree of regional dysfunction. This allows clinicians the opportunity to synthesise a considered judgement about risks and benefits of offering revascularisation to patients with coronary artery disease (CAD) and impaired LV function. Already these findings are resulting in a paradigm shift, where in thinned (<5 mm) hypokinetic myocardium previously assumed to be scar tissue, the absence of LGE and thus infarction is often associated with restoration in wall thickening and function post-revascularisation, thus challenging previous assumptions. In addition, LGE-CMR is also useful in demonstrating the complications of infarction including true and false aneurysms, ventricular septal defects and apical thrombi.w7 In patients in whom cardiac resynchronisation therapy is being considered, the presence of lateral wall scarring is associated with a lower likelihood of responsiveness at 6 months.9
Compared to established imaging techniques for viability assessment, there is excellent correlation with positron emission tomography (PET) findings.10 In a study by Wagner et al, CMR had a higher sensitivity and specificity to detect infarcted myocardium compared to single photon emission computed tomography (SPECT) in canine hearts.11
Viability and hibernation can also be detected with high sensitivity and specificity using a low and high dose dobutamine infusion protocol to gauge changes in wall thickness and motion, similar to stress echo.w8
Myocardial perfusion assessment
Myocardial perfusion imaging using CMR is a current area of intense development.w19 First-pass imaging with adenosine stress following the injection of a bolus of Gd-CA is useful to both detect coronary stenoses and assess their severity. Under-perfused segments will show hypoenhancement in early imaging in a distribution subtended by the culprit stenoses. It is therefore helpful both in the initial screening assessment of patients with suspected ischaemic aetiologies for their LV dysfunction and also as a complementary adjunct to x ray angiography when the significance of documented lesions is unclear. Combined with the LGE technique, CMR perfusion provides a powerful means of assessment.12 Trials are currently underway comparing CMR perfusion with SPECT imaging.
Assessment of coronary arteries
Imaging of the coronary arteries by magnetic resonance imaging (MRCA) has proved technically challenging. Coronary arteries are small and often tortuous vessels that move during the cardiac cycle as a result of both cardiac contraction and respiratory motion. In addition, these vessels are often surrounded by epicardial fat which can often compromise the contrast-to-noise ratio (CNR). Despite these challenges, MRCA can achieve imaging resolutions of <1 mm.
For patients with disease of the left main coronary artery or three-vessel disease, MRCA was demonstrated in a large prospective multicentre study of 109 patients with suspected coronary disease to have a high sensitivity (100%), specificity (85%), and accuracy (87%). The negative predictive value for this group was 100%.13 However, in the detection of any coronary disease, the accuracy was only 72% with a negative predictive value of 81%. At present, MRCA is therefore not used routinely to exclude stenoses in epicardial vessels. Its use is mainly limited to identifying the origin and course of anomalous coronary arteries and bypass grafts.w10 w11 Recent developments using whole heart imaging,w12 more powerful 3 T scanners and developments in intravascular MR contrast agents are likely to have an impact on the clinical applications of MRCA.
Dilated cardiomyopathy
Dilated cardiomyopathy (DCM) is characterised by the dilatation and functional impairment of the LV in the absence of significant CAD. In a proportion of patients the RV is also affected and this is associated with a poorer prognosis. Histologically, it is characterised by progressive interstitial fibrosis and degeneration of myocytes. Replacement fibrosis is also often seen and, unlike in CAD, there is mid-wall rather than subendocardial fibrosis due to involvement of the circumferential fibre layer.
Clinically, in the patient presenting with new-onset heart failure, it can sometimes be difficult to establish if the aetiology is ischaemic or due to DCM. Patients often present without a history of angina or prior myocardial infarction. The current discriminatory diagnostic tool considered to be the gold standard is x ray coronary angiography.w13 However its invasive nature, use of ionising radiation and nephrotoxic contrast media exposes patients to a small but significant risk of serious complications.
CMR is able to provide reproducible measurement of the ventricular volumes, mass and function, and is useful to determine the response to treatment.
In a prospective study of fibrosis patterns in 63 patients with a clinical diagnosis of DCM and normal coronary angiograms,14 60% of patients showed no late enhancement, while in about 30% of patients a patchy, mid-wall pattern of enhancement is seen that is distinct from that observed in CAD. Moreover, this pattern of mid-wall LGE correlates well with autopsy and explanted hearts from patients with DCM (fig 2⇓).15w14 Also interestingly, in 12% of patients, a subendocardial pattern typical of CAD was seen. In spite of the normal angiogram, an ischaemic aetiology is likely due to recanalisation, spasm or arterial emboli. This study highlights some of the limitations of luminography in assessing patients with heart failure. The clinical implications are important prognostically and because this latter cohort of patients would have been mislabelled as having idiopathic DCM when in fact they warrant treatment for secondary prevention of ischaemic heart disease with agents such as aspirin and statins. In addition, some patients with co-existent minor CAD on invasive coronary angiography (for example, single vessel disease) may be misdiagnosed as having an ischaemic aetiology when the primary pathology is a non-ischaemic DCM.
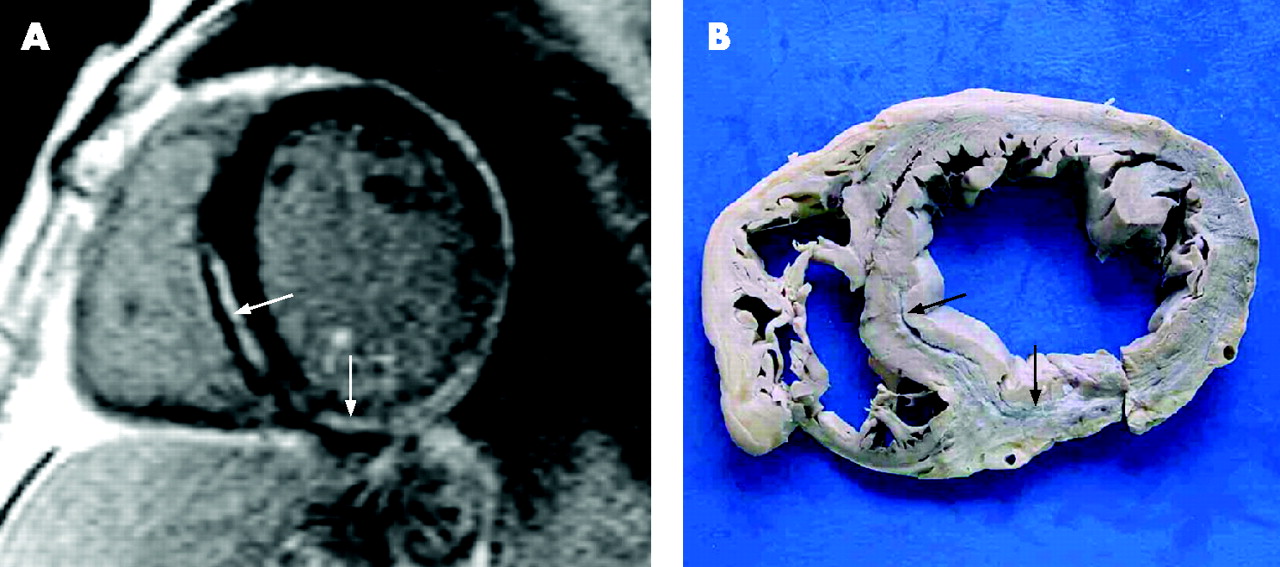
Mid-wall fibrosis in dilated cardiomyopathy. Panel A shows the pattern of patchy mid-wall late gadolinium enhancement (LGE) found in ∼30% of patients with dilated cardiomyopathy (DCM). The arrows delineate mid-wall fibrosis in the septum and inferolateral walls. Panel B shows an autopsy sample from a patient with DCM with a strikingly similar pattern of fibrosis (black arrows).
The same study also demonstrated that in 27 heart failure patients with previous infarctions and documented CAD on x ray angiography, a subendocardial pattern of LGE characteristic of ischaemic cardiomyopathy was always seen.
LGE is therefore useful to differentiate aetiology in such patients. It has a complementary role to angiography and in many cases may avoid the need for the latter.
It has also been proposed that in patients with the typical pattern of subendocardial enhancement in a coronary artery territory, primary DCM can be excluded as a sole cause. Subsequent prospective studies using LGE to differentiate the underlying aetiology have already produced promising results with a high accuracy.16w15 Ongoing trials using augmented protocols with MRCA and/or CMR perfusion with LGE in this group may produce even better results, thereby providing robust evidence for LGE as a valid non-invasive alternative to invasive x ray coronary angiography.
Left ventricular non-compaction
Left ventricular non-compaction (LVNC) is a specific cardiomyopathy characterised by hypertrabeculation of the left ventricle with deep intertrabecular recesses, resulting in a distinct non-compacted layer lining the cavity of the LV. This non-compacted layer is most prominent in the apex of the LV. The condition is thought to result from a failure of the compaction process of myocardial trabeculae during endomyocardial embryogenesis. As well as causing heart failure with a phenotype similar to DCM, it has been associated with malignant arrhythmias and thromboembolism. Current diagnostic criteria are based on echocardiographic definitions of the ratio of non-compacted to compacted layer. However, as the apex may be poorly visualised with conventional echocardiography, recent studies have suggested CMR-derived criteria which may result in increased diagnostic accuracy.w16
Myocarditis
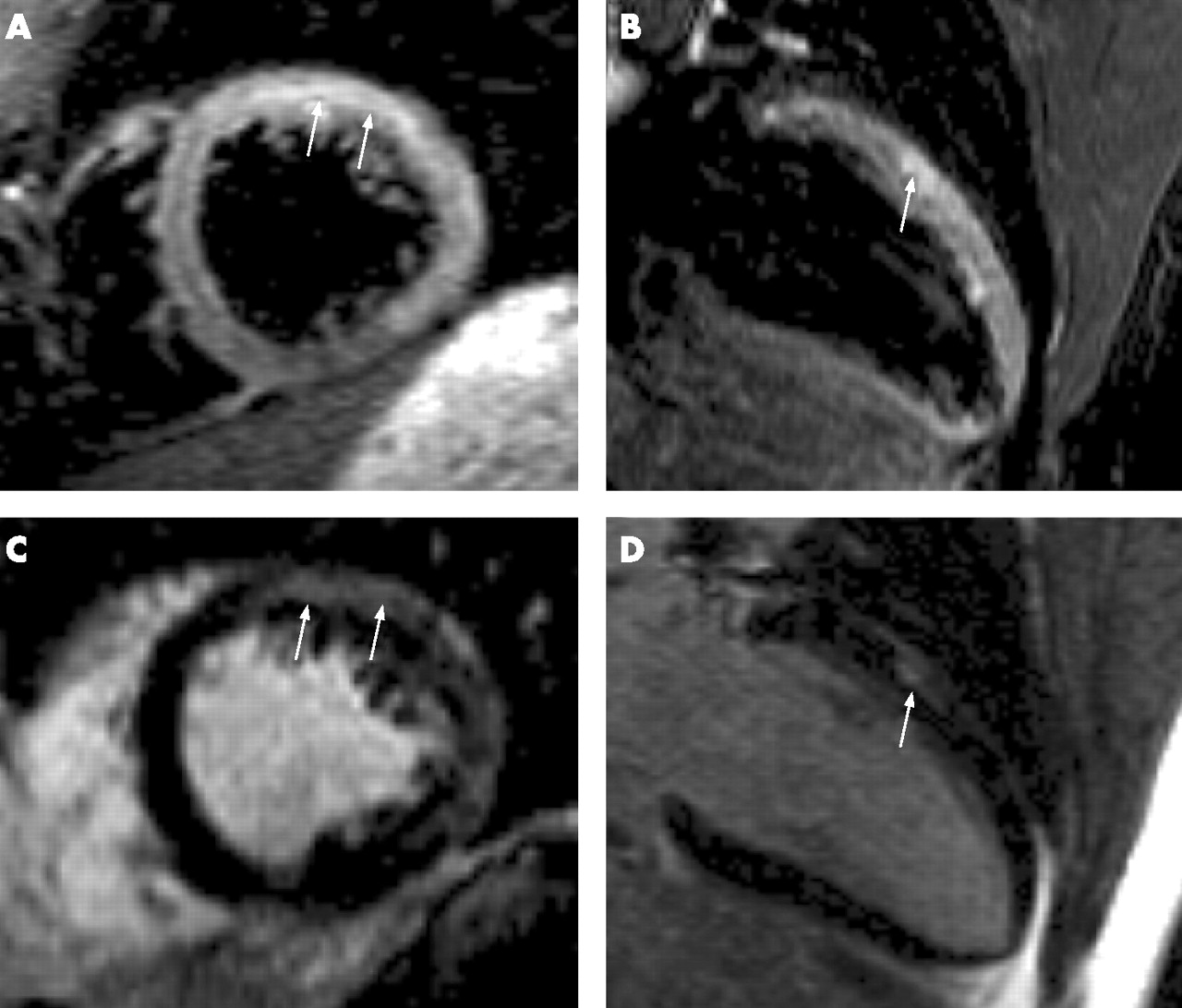
In patients presenting acutely with heart failure, normal coronaries and evidence of DCM, an important cause is myocarditis. Biopsy-validated CMR studies in such patients have been very informative.5 T2 weighted images can show focal increases of mid-wall and subepicardial myocardial signal defining areas of oedema (fig 3⇓). This is particularly in the first 3 weeks from symptom onset. In the proportion where there is residual fibrosis, this can be detected by LGE. CMR is useful to establish the diagnosis and guide biopsy, thereby increasing the yield of this invasive procedure. Early changes in LV remodelling can be identified to guide decisions on implementing treatments such as ACE inhibitors and β-blockers.w17
Inflammation and fibrosis in myocarditis. Panels A and B show T2 weighted images from a patient with myocarditis (mid SA and 2 chamber views, respectively). The arrows delineate a bright area of signal in the mid-wall of the anterior left ventricular wall. Corresponding late gadolinium enhancement (LGE) images (panels C and D) show a smaller area of enhancement indicating fibrosis.
Hypertrophic cardiomyopathy
Hypertrophic cardiomyopathy (HCM) is characterised by asymmetric wall thickening, myocyte disarray and interstitial plus replacement fibrosis. The pattern of replacement fibrosis is unlike that seen in DCM or post-infarction. Typically, it is patchy, mid-wall and most commonly in areas of maximal wall thickening. Microvascular ischaemia is a potential mechanism. A cohort of patients is at risk of developing the progressive variant with heart failure.17 Transthoracic echocardiography is the most commonly used non-invasive method to study HCM. However, the three-dimensional nature of CMR allows for the precise definition of the site and the extent of hypertrophy, especially at the basal anterolateral wall and apex which are less well assessed by echocardiography, sometimes leading to missed diagnoses.18,19 Small cavity volumes with good systolic function can be readily assessed.
Correlating with pathological patterns of fibrosis, several in vivo CMR studies have confirmed the patchy, mid-wall patterns of enhancement that are not attributable to a specific coronary artery territory. LGE may have a role in diagnosing and identifying high risk patients.20
About 4% of patients who present clinically with HCM actually have Fabry’s disease (an X-linked disorder of sphingolipid metabolism causing idiopathic left ventricular hypertrophy). LGE shows a distinct and unusual pattern of lateral wall enhancement in these patients with a concentric pattern of hypertrophy.w18
CMR is also useful in distinguishing heart failure linked to HCM from hypertensive heart disease. In the latter, there is a concentric pattern of wall thickening that usually does not exceed 15 mm, with increased cavity volumes and reduced or normal range systolic function. While these patients have increased interstitial fibrosis, replacement fibrosis of the type detected by CMR is unusual. By contrast, about 60–80% of patients with HCM have evidence of patchy fibrosis.21w19
Arrhythmogenic right ventricular cardiomyopathy
Arrhythmogenic right ventricular cardiomyopathy is characterised by RV dilatation and functional impairment resulting from fibrofatty replacement of the RV myocardium. LV dilatation is a late manifestation. It is a genetic condition and can cause sudden death from arrhythmia or progressive heart failure. Diagnosis is made on the basis of defined taskforce criteria.22 There is biventricular dilatation in about 20% of cases so that it can sometimes be difficult to distinguish from DCM. The disproportionate RV enlargement in conjunction with regional RV wall abnormalities is a useful guide.
The RV is difficult to visualise by echo due to near field signal dropout and the crescentic shape of this ventricle. CMR is able to obtain three-dimensional images to depict structural and functional abnormalities and so is well suited to demonstrate regional wall motion abnormalities, thinning and aneurysmal changes in the RV free wall,23 increased RV and LV volumes, and increased T1 myocardial signal suggesting fatty infiltration. The role of LGE is currently being evaluated in this condition.24 The RV myocardial tissue is significantly thinner than that of the LV and has a higher degree of trabeculation so that detection of RV wall fibrosis is more difficult. Recent work in genotyped cohorts suggests that about 20% of patients have evidence of LV fibrosis.
Amyloidosis
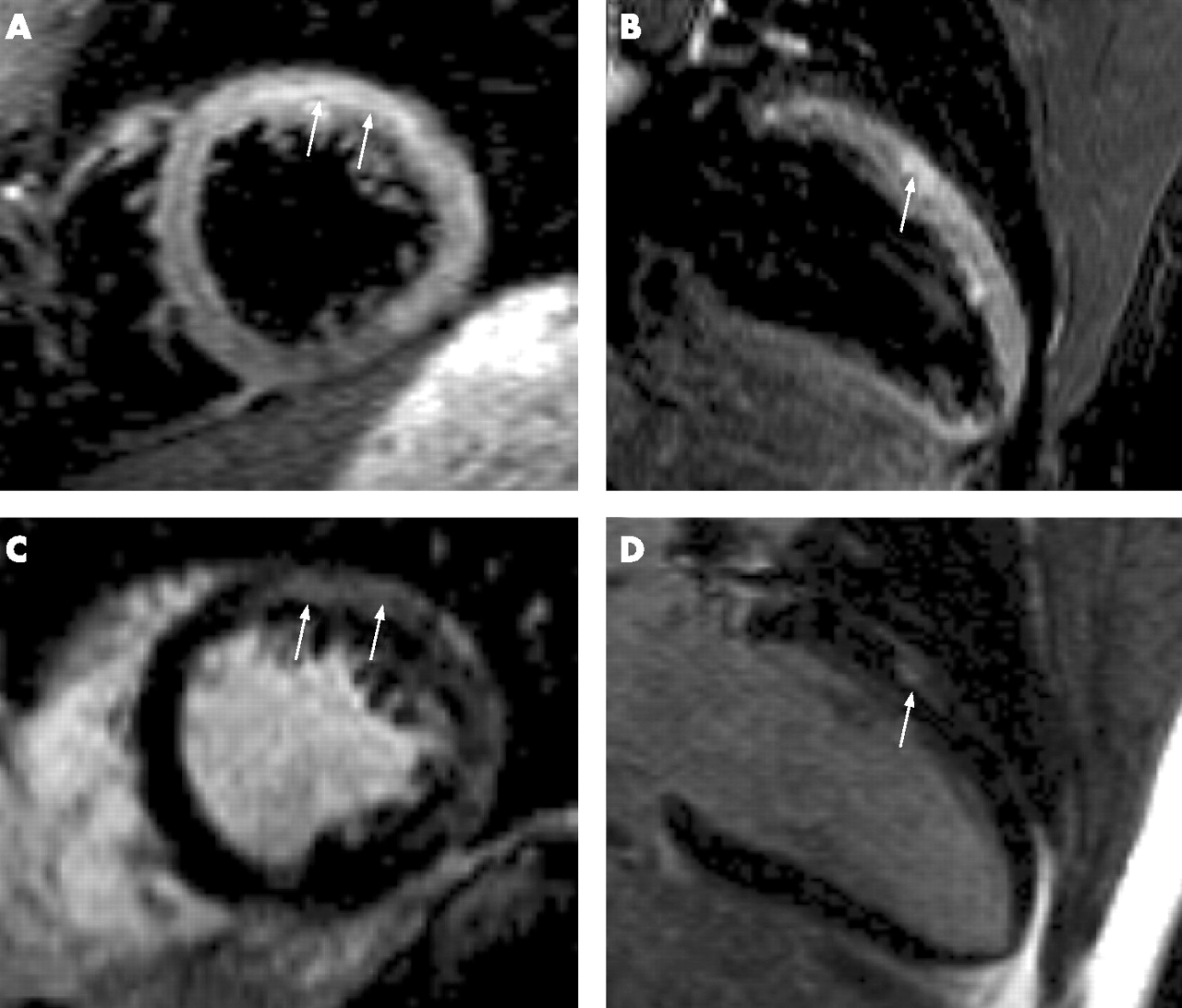
Amyloid heart disease is characterised by fibril deposition within the myocardium. There is concentric wall thickening but poor contractility with pronounced diastolic dysfunction. The interatrial septum is often thickened and there is atrial dilatation. CMR is useful to document these abnormalities. Following Gd-CA, there is a unique pattern of late circumferential enhancement of the subendocardium (fig 4⇓) of the LV and RV in a zebra pattern, with a dark blood pool.25 This reflects high myocardial uptake, fast blood washout, and similar T1 values of the blood pool and myocardium in this condition.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
CMR in cardiac amyloid. Panels A and B show images from a four chamber cine acquisition in diastole and systole, respectively, in a patient with biopsy proven cardiac amyloid. The cine images reflect pronounced left ventricular hypertrophy with poor systolic function. Panels C and D show the circumferential pattern of late gadolinium enhancement (LGE) seen in cardiac amyloid (black arrows).
Constrictive pericarditis
Distinguishing a restrictive from a constrictive cause of cardiomyopathy can be challenging. The wide field of view of CMR enables assessment of the pericardium, particularly by T1 spin echo sequences. Constrictive physiology with inferior vena cava (IVC) dilatation, septal bounce in diastole accentuated during free-breathing, and mild atrial dilatation are well seen.w20 Where surgery is planned, guidance is given on the extent and regions of pericardial thickening as the process can often be patchy, and also if there is a layer of epicardial fat between the heart and visceral layer of the pericardium to facilitate stripping.
When to order a CMR scan in heart failure
Poor acoustic windows on echocardiography
“Borderline cases” on echocardiography
Viability and perfusion assessment in the context of poor left ventricular function and severe coronary artery disease
Non-invasive tissue characterisation for aetiology in cardiomyopathy
Myocardial iron quantification in iron overload cardiomyopathies
Early monitoring of treatment response
Evaluation in patients with dual pathologies
Sarcoidosis
In patients with sarcoidosis at autopsy, 20–30% have evidence of cardiac involvement. Typically granulomatous changes most commonly affect the LV lateral wall, papillary muscles, RV subendocardial surface and RV free wall. The diagnosis of cardiac involvement is important to establish as a proportion of patients may present with sudden cardiac death due to malignant ventricular arrhythmias. Patients with cardiac sarcoid may also develop progressive heart failure due to LV dilatation and functional impairment. LGE is useful to detect cardiac granulomatous disease, and may provide a potential therapeutic marker.w21 In addition, the use of T2 weighted sequences identifies myocardial inflammation which can be used as a guide to disease activity.26 Work is still underway to determine the sensitivity and specificity of CMR in this condition.
Iron overload cardiomyopathy
CMR has established itself as the gold standard investigative tool for the non-invasive assessment of myocardial iron overload. In patients with primary haemochromatosis or secondary forms such as tranfusional iron overload (for example, for treatment of β-thalassaemia major), heart failure is an important cause of morbidity. The extent of iron distribution can be quantified using a measure of myocardial T2 signal. This simple scan can be performed in a single breath-hold and is validated against both biopsy samples and other markers of myocardial dysfunction such as LV ejection fraction.27 More importantly, serial scans can directly guide iron chelating drug regimens.28
RISK STRATIFICATION AND PROGNOSTIC IMPLICATIONS
As a relatively new technology, long-term outcome data are limited at present for patients with heart failure. In patients with ischaemic aetiologies, the amount of scar tissue correlates closely with the likelihood of inducible ventricular tachycardia on electrophysiological studies.29 Quantification of the peri-infarct zone has a high predictive value for clinically significant arrhythmias and so may have a role in guiding adjunctive invasive therapies such as ICDs.30
In DCM, the presence of mid-wall fibrosis is associated with an increased incidence of all cause mortality and unplanned hospitalisation. There is a trend towards increased significant arrhythmia. These findings are independent of established markers of adverse outcome such as LV ejection fraction.15 Further work is required to examine the positive and negative predictive value of this finding in the DCM cohort.
In HCM, long-term outcome data are awaited. There is an association between the presence of fibrosis as detected by LGE and the likelihood of developing heart failure in patients over the age of 40 years.
CONCLUSION
CMR offers the opportunity for a detailed evaluation of patients with heart failure. In addition to myocardial function and anatomy, CMR provides a more comprehensive assessment than other imaging modalities with the opportunity for tissue characterisation, detection of perfusion defects and measurement of hibernation. Such applications give referring clinicians information on the aetiology of the underlying heart failure as well as valuable data in guiding management and risk stratification. Current work with 3T scanners and better targeted contrast agents are likely to expand the usefulness. Important challenges are to collect more outcome data and increase access. As an imaging modality it offers complementary and incremental information to first-line methods such as echocardiography, and is now frequently avoiding the need for more invasive investigations.
Additional references appear on the Heart website— http://heart.bmj.com/supplemental
INTERACTIVE MULTIPLE CHOICE QUESTIONS
This Education in Heart article has an accompanying series of six EBAC accredited multiple choice questions (MCQs).
To access the questions, click on BMJ Learning: Take this module on BMJ Learning from the content box at the top right and bottom left of the online article. For more information please go to: http://heart.bmj.com/misc/education.dtl Please note: The MCQs are hosted on BMJ Learning—the best available learning website for medical professionals from the BMJ Group.
If prompted, subscribers must sign into Heart with their journal’s username and password. All users must also complete a one-time registration on BMJ Learning and subsequently log in (with a BMJ Learning username and password) on every visit.
Acknowledgments
Dr Ravi Assomull is funded by a British Heart Foundation Junior Fellowship.
REFERENCES
Supplementary materials
Files in this Data Supplement:
Footnotes
In compliance with EBAC/EACCME guidelines, all authors participating in Education in Heart have disclosed potential conflicts of interest that might cause a bias in the article
Linked Articles
- Miscellanea