Article Text

Abstract
Objective To determine whether the effect of South Asian ethnicity differs between studies of incidence and prognosis of coronary disease.
Design Systematic literature review and meta-analysis, and cohort analysis from a national acute coronary syndrome (ACS) registry linked to mortality (National Institute of Cardiovascular Outcomes Research/Myocardial Infarction National Audit Project).
Setting International for the review, and England and Wales for the cohort analysis.
Patients The numbers of South Asians included in the meta-analysis were 111 555 (incidence) and 14 531 (prognosis) of whom 8251 were from the ACS cohort.
Main outcome measures Incidence studies: non-fatal myocardial infarction or fatal coronary heart disease; prognostic studies: mortality; HRs for 1-year all-cause death in ACS cohort.
Results South Asians had higher incidence of coronary disease compared with white subjects (HR 1.35 95% CI 1.30 to 1.40) based on meta-analysis of nine studies. Among 10 studies on prognosis, South Asians had better prognosis compared with white subjects (HR 0.78 95% CI 0.74 to 0.82). In the ACS cohort, the impact of diabetes (42.4% of South Asians, 16.9% of white subjects) on 1-year mortality was stronger in South Asians than white subjects (age-adjusted HR 1.83 95% CI 1.59 to 2.11 vs 1.53 95% CI 1.49 to 1.57). However, prognosis was better in South Asians even among diabetics, older people and those living in areas of the highest social deprivation.
Conclusions South Asian ethnicity is associated with higher incidence of coronary disease, but lower mortality once coronary disease is manifest. The dissociation between effects on incidence and prognosis suggests that public health initiatives to reduce inequalities in mortality between South Asian and white populations should focus on primary prevention.
This is a CALIBER study with ClinicalTrials.gov Identifier: NCT01163513.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/
Statistics from Altmetric.com
Introduction
Coronary death rates among first-generation migrants from South Asia in high income countries have long been found to be higher than those of the white majority population.1 Understanding the relative contribution of incidence and prognosis to overall coronary death rates allows preventive interventions to be targeted where they are likely to be more efficacious, that is, should public health policy seeking to address ethnic inequalities in coronary death rates focus more on primary prevention, secondary prevention or both? The last systematic review in this field was published in 2000;2 of 19 studies, none were of incidence nor were there any prospective studies of prognosis, studies found being mostly of disease prevalence and mortality.
A worse prognosis in South Asian people might be expected for three main reasons. First, South Asian populations have a higher prevalence of insulin resistance and diabetes mellitus than white populations3 and the presence of diabetes with coronary disease is associated with worse survival in both ethnic groups in large registries.4 However, whether the effect of diabetes confers a worse prognosis in the South Asian compared with white patient is not fully known. Second, some,5 ,6 but not all,7 ,8 studies suggest that underuse of medical treatments is more common among South Asian patients, partly because they are more likely to live in areas with relative social and economic deprivation.9 Third, severity of disease at presentation may be different between ethnic groups.10 However, recently some studies have suggested that South Asians may not have a worse prognosis.11
Our research objective was to test whether the impact of South Asian ethnicity on coronary disease differed between studies of incidence and prognosis. Thus, we sought to compare the long-term influence of South Asian ethnicity on the onset of coronary disease in populations without manifest coronary disease (aetiological effects) and survival in populations with coronary disease (prognostic effects). Discordance between onset of disease and progression would have significant public health implications. We carried out for the first time a systematic review and meta-analysis of published incidence studies and prognosis studies and report a large registry cohort of patients with acute coronary syndrome (ACS). This approach of combining literature review with the largest newly reported study is a combination used often in biomarker research.12 ,13 The new ACS cohort data allowed us to investigate the role of diabetes, secondary prevention medication at discharge, social deprivation and whether Indians, Pakistanis and Bangladeshis differed respectively in associations with prognosis compared with majority white populations.
Patients and methods
Systematic review
Using a search strategy developed with an expert librarian based on terms for coronary disease (from the Cochrane Library of systematic reviews and protocols), incidence or prognosis and South Asian ethnicity, we searched MEDLINE (PubMed) from inception until January 2012. Our definition of a South Asian was that of a person whose ancestry was in the countries of the Indian subcontinent (India, Pakistan, Bangladesh and Sri Lanka). We included initially any prospective studies on coronary artery disease comparing white and South Asian populations which reported outcomes as fatal or non-fatal coronary disease for incidence studies and death for prognostic studies. On reviewing the full manuscripts of the remaining papers, we excluded studies that used composite outcomes that included non-coronary events such as stroke for improved comparability. We excluded studies that disaggregated the South Asian group into its component groups (eg, Pakistani, Bangladeshi). For incidence, we included both general population studies and high risk populations free from manifest coronary disease at baseline, and for prognosis, populations both presenting with angina and myocardial infarction. No language or date restrictions were used. This search was repeated in the EMBASE database. Hand-searching of the reference list of eligible studies was conducted to identify further relevant work (backward citation tracking). Science Citation Index was used to identify all the subsequent papers that cited any of the eligible studies (forward citation tracking) using Institute for Scientific Information (ISI) Web of Science.
MJZ (cardiologist and epidemiologist) and AF (cardiologist) independently initially reviewed the titles and abstracts of all studies retrieved. MJZ and HH (epidemiologist) reviewed full manuscripts of papers obtained following initial inspection of titles and abstracts to determine final papers included. Once included papers were agreed upon, the following data were extracted by MJZ, AF and PP (statistician) according to a predetermined protocol: setting of study, number of participants by ethnic group, age range (mean or median), numbers of women/men and participants with diabetes, outcome measures (fatal, non-fatal, all-cause, coronary), and duration of follow-up and risk factors that were adjusted for in prospective analyses. Relative risks were extracted, adjusted where available, from each study. In studies in which summary relative risk estimates were not given, the crude data in the paper were examined to estimate unadjusted ORs and CIs and we approached the authors of studies to confirm relevant numerical data (data available on request). Where studies reported multiple relative risk estimates within a study, we extracted the most coronary-specific risk and 95% CI adjusted for the most number of variables.
Population, definitions and follow-up in a new ACS cohort
The ACS cohort consists here of all patients with ACS collected consecutively between 2004 and 2008 from all 230 hospitals in England and Wales using the Myocardial Infarction National Audit Project (MINAP).14 ACS type was categorised into ST-elevation myocardial infarction (STEMI), non-ST-elevation myocardial infarction (NSTEMI, any level of elevated troponin) or unstable angina (negative troponin), categories we validated against ECG and troponin data in the database. The patient's ethnic group was classified in MINAP as white Caucasian, Asian, Black, Oriental and Other by the audit nurse or other coder based on using the case notes and from 2007 onwards, MINAP further categorised the Asian group into Indian, Bangladeshi or Pakistani as per contemporary census categories. Diabetes was defined as known and newly-diagnosed cases. We defined secondary prevention management as receipt of aspirin, statin, β-blocker and ACE inhibitor drug at discharge. Smoking data were collected as current/previous/never. Area deprivation was collected as the Index of Multiple Deprivation 2004 score. Actual troponin levels were available, and we stratified at three levels (≤0.05, 0.05–1, >1 ng/ml). We had information on receipt of or plan for coronary angiography, and receipt of inpatient revascularisation. Admission heart rate, admission systolic blood pressure and age are among the strongest correlates of ACS survival15 and were combined into a prognostic score. The estimated coefficients of the patients’ values for these variables were added together to form a prognostic score for severity of disease. Ethnic density was defined as a hospital-level variable that considered the proportion of South Asian admissions among all ACS admissions for each hospital. It was then converted into three groups (low/medium/high using <1% as low, between 1% and 5% as medium and >5% as high), as according to the Office for National Statistics April 2001 census, South Asian people made up just over 3.5% of the total UK population. Vital status was available in 98.4% of patients and we analysed all-cause death at 1 year from admission as our primary endpoint; we used 30-day all-cause death as a sensitivity analysis. We registered this cardiovascular disease research using Linked Bespoke studies and Electronic health Records16 with ClinicalTrials.gov (reference number NCT01163513) and the analytic protocol was uploaded prior to analyses.
Statistical analyses
For the studies selected in the systematic review, we undertook a meta-analysis according to Meta-analysis of Observational Studies in Epidemiology (MOOSE) criteria.17 The results from these studies were combined using the metan command in Stata 11 and pooled ORs, weights and 95% CIs were calculated using a random effects model. For incidence, we divided studies into those examining fatal or non-fatal/fatal outcomes. For prognosis, we divided studies by acute and chronic coronary disease. Heterogeneity was examined using the I2 statistic.
In our ACS cohort, we performed Cox proportional hazards regression for the risk of all-cause death adjusted for age (as a continuous variable), sex, hypertension, hypercholesterolaemia, smoking, diabetes, Index of Multiple Deprivation and ACS phenotype (whether a NSTEMI, STEMI or unstable angina patient). In order to examine potential reasons for ethnic differences in prognosis, we compared the prevalence of baseline characteristics between ethnic groups through cross tabulations and χ2 tests. We then compared age-adjusted risk of death at 1 year within strata defined by these baseline characteristics using Cox regression methods. Continuous variables were tested for non-linearity and spline terms included where appropriate.18 We tested for non-proportionality using the Therneau and Grambsch test (based on Schoenfeld residuals). We allowed the possibility of a spline term for age but there was no real deviation from linearity so the final model has age as a linear function. For these analyses, 203 092 white and Asian patients had complete data for our a priori full adjustment model, of which there were first admissions for 72 892 STEMIs and 111 728 NSTEMIs. Of 355 088 records, 151 996 had missing values for at least one of the 12 a priori defined covariates: ethnicity, age on admission, gender, smoking status, previous diagnosis of diabetes, history of hypertension, history of hypercholesterolaemia, Index of Multiple Deprivation and four secondary prevention medications (ACE inhibitor, aspirin, β-blocker, statin). In order to minimise selection bias and to reduce variability in the model estimates, we imputed missing data using multivariate imputation by chained equations (MICE)19 in the statistical package R (open source Comprehensive R Archive Network (CRAN) package MICE).20 Full details are available on request.
All main analyses were performed in Stata V.11 (Stata, College Station, Texas, USA), and in R or MICE where stated.
Results
Incidence of coronary disease in South Asian compared with white people: systematic review and meta-analysis
Of the 191 potentially relevant publications on incidence from the search strategy, we excluded 178 as they were on ethnic groups other than South Asian (eg, studies on East Asian populations such as the Chinese), not on coronary disease or not of prospective design. No further papers were found on Embase. Of the 13 full papers examined, we excluded four due to the South Asian participants being analysed by their component groups or when a composite outcome included cerebrovascular disease: we were unable to get aggregated ethnicity data and disaggregated outcome data after contacting authors (see online supplementary figure 1). The remaining nine studies are tabulated in online supplementary table 1.21–29 Three of these studies were in people with a cardiovascular risk factor but without manifest coronary disease.23 ,25 ,27 For the meta-analysis, the Whitehall II study was split into two studies based on fatal or non-fatal outcomes,28 and one study was analysed by sex resulting in 11 populations from the nine studies.22 Meta-analysis of all 11 incidence populations (111 555 South Asians with 2527 events, 4 197 923 white subjects with 65 241 events) showed that South Asians had a higher incidence of coronary disease compared with white majority populations (figure 1 HR 1.35 (1.30 to 1.40)). This was consistent for the two cohorts examining incidence of fatal coronary disease (figure 1 upper panel, HR 2.18 (95% CI (1.65 to 2.87)) and the studies examining incidence of non-fatal (alone or with fatal) coronary disease (figure 1 lower panel HR 1.34 (HR 1.29–1.39)).
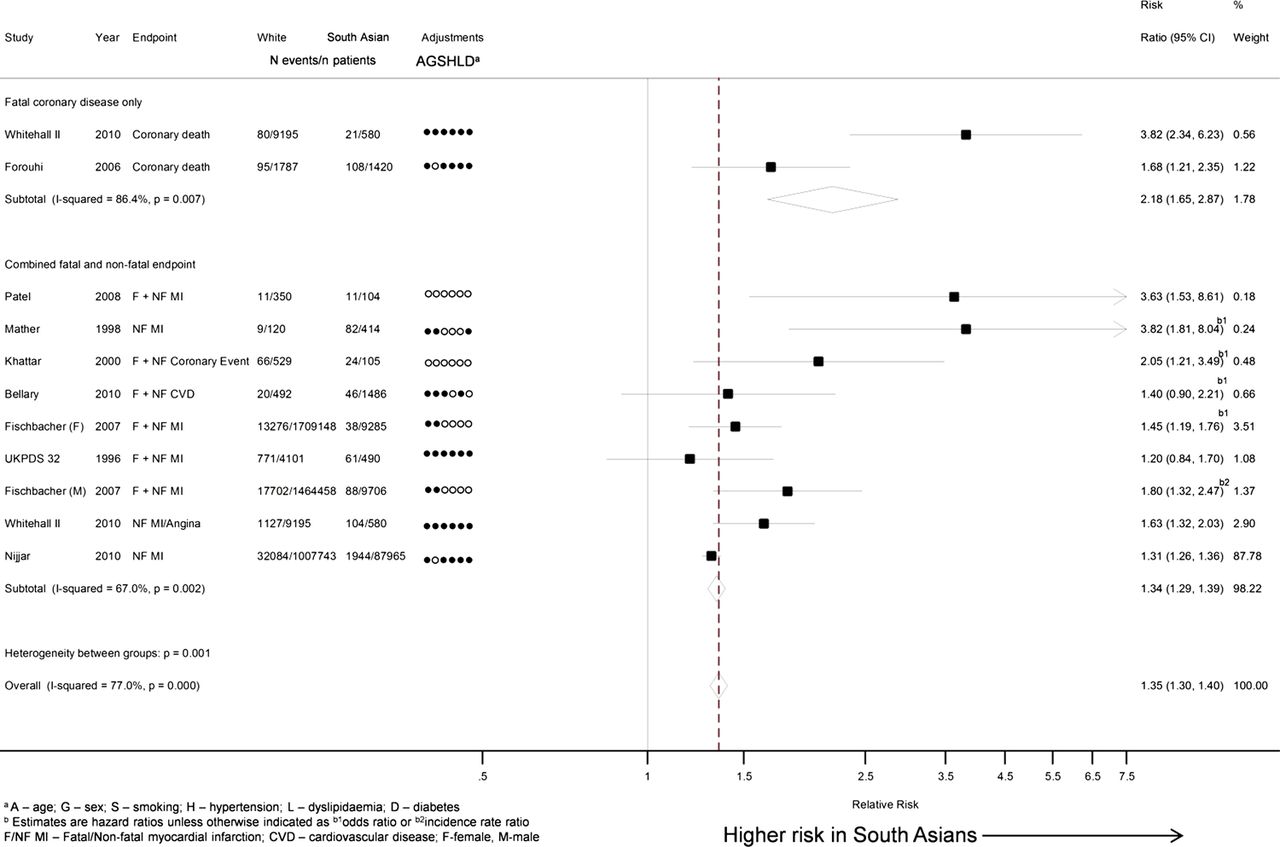
Incidence of coronary disease in South Asians compared with white subjects meta-analysis of 11 incidence populations including 111 555 South Asians. This figure is only reproduced in colour in the online version.
Prognosis of coronary disease in South Asian compared with white people: systematic review and meta-analysis
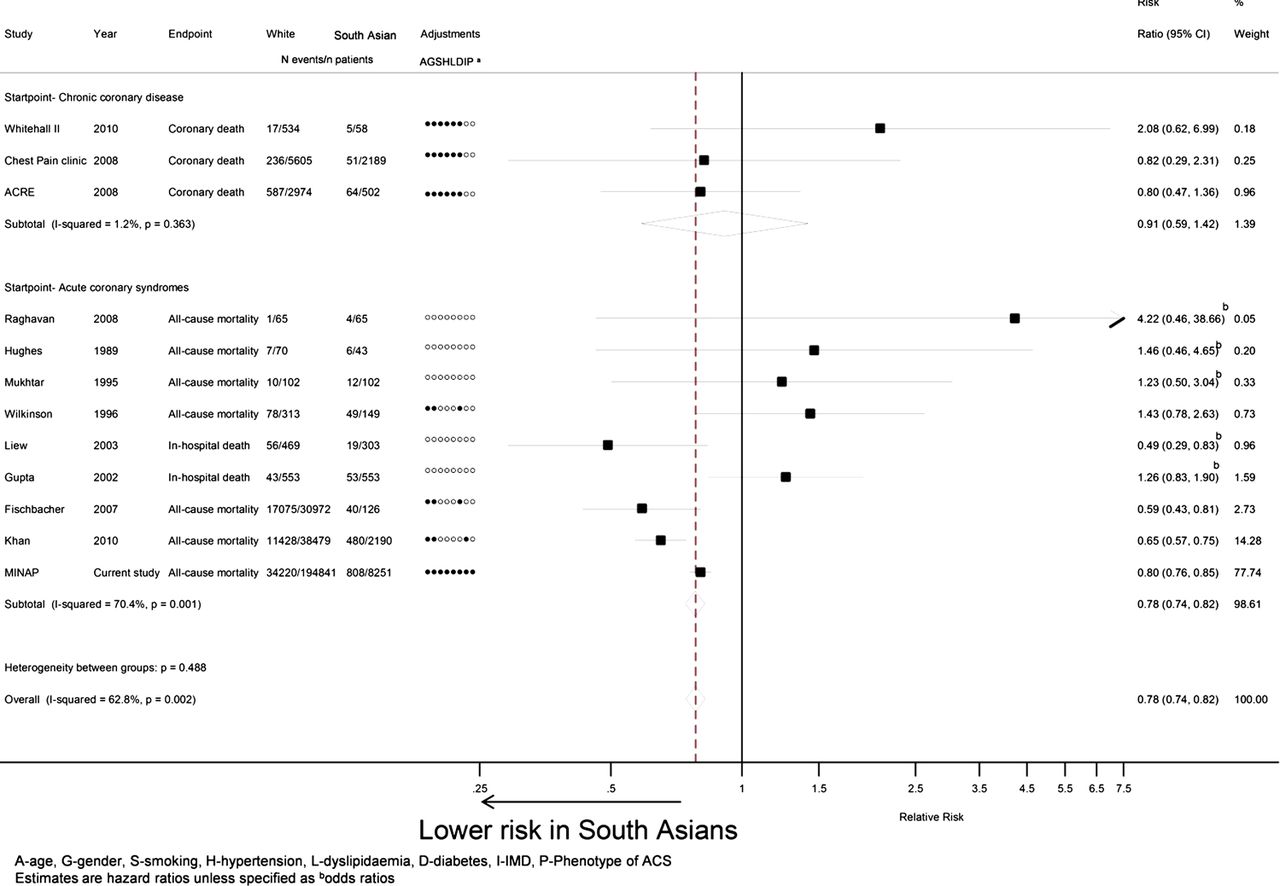
Of the 642 potentially relevant publications on prognosis from the search strategy, we excluded 624 as they were on ethnic groups other than South Asian, not on coronary disease or not of prospective design. No further papers were found on Embase. Of the 18 full papers examined, we excluded eight (see online supplementary figure 1) and the remaining studies are tabulated in online supplementary table 2.11 ,22 ,28 ,30–36 In all, this table contains 12 populations examining prognosis as we additionally included a prognostic population from our Whitehall II study28 (in those participants who, from responses on the Rose questionnaire, had typical angina at baseline) and our ACS cohort. Meta-analysis of all 12 prognosis populations (14 531 South Asian patients with 1591 events, 274 977 white subjects with 63 758 events) showed that South Asians had a better prognosis from coronary disease compared with white majority populations (figure 2 HR 0.78 (95% CI 0.74 to 0.82)). This better prognosis in South Asians compared with white subjects was particularly apparent in bigger, more recent studies on acute clinical presentations.
{kind=link}
{kind=link}
Prognosis of coronary disease in South Asians compared with white subjects meta-analysis of 12 prognosis populations including 14 531 South Asian patients. This figure is only reproduced in colour in the online version.
Stratified analyses of ethnic differences in prognosis after ACS
Using the ACS cohort (our new study), we performed stratified analyses (table 1) to test in more detail whether the better prognosis in South Asians found on meta-analysis differed according to demographic, risk factor, disease phenotype and management characteristics. In no age group was prognosis significantly worse in South Asians. South Asians were younger and thus all further stratified analyses were adjusted by age. By sex, South Asian men had a better prognosis than white men (HR 0.88 (0.81 to 0.96)), prognosis being equitable among women between ethnic groups (0.96 (0.85 to 1.07)). The test for heterogeneity however was not significant (0.22) refuting the possibility of a significant interaction of sex on the relationship between ethnic group and mortality. Within the most socially deprived group, South Asians had a better prognosis compared with white subjects (HR 0.73 (0.65 to 0.82)). The association of prognosis with South Asian ethnicity was consistent among Indians (HR 0.84 (0.73 to 0.96)), Pakistanis (HR 0.77 (0.66 to 0.91)) and Bangladeshis (HR 0.86 (0.61 to 1.21)). In preliminary analyses, we had found diabetes to be more prevalent in South Asian (42.4%) compared with white (16.9%) patients, and the impact of diabetes on mortality stronger in South Asians than white subjects (age-adjusted HR 1.83 (95% CI 1.59 to 2.11) vs 1.53 (95% CI 1.49 to 1.57)). Despite this, from table 1, it can be seen that South Asians had a better prognosis than white subjects irrespective of diabetic status (HR=0.78 in both diabetics and non-diabetics). South Asians at low and high prognostic risk at admission had better survival than their white counterparts (HR 0.74 (95% CI 0.64 to 0.86) in high risk patients). South Asian participants were more likely to be on four secondary prevention medications following ACSs than white participants. South Asians were more likely to receive angiography and revascularisation than white subjects but receipt of these was associated with higher mortality (age-adjusted HR for South Asians vs white subjects of 1.50 (1.24 to 1.81) for patients with revascularisation and 0.88 (0.82 to 0.96) among patients without revascularisation).
Age-adjusted mortality at 1 year after ACS in South Asian compared with white patients according to demographic, risk factor, disease phenotype and management characteristics (n=203 092)
Thus, throughout these stratified analyses, there were no strata in which South Asians had a worse prognosis than white subjects.
Imputation within the ACS cohort and 30-day mortality
Results from using the imputed datasets were further away from the null and had tighter CIs, with South Asians still having a better survival at 1 year than white subjects (HR 0.77 (0.73 to 0.82), adjusted for age, sex, smoking status, previous diagnosis of diabetes, hypertension, hypercholesterolaemia, Index of Multiple Deprivation and ACS phenotype). When we further adjusted for all of the variables reported in table 1 the better prognosis in South Asians compared with white subjects in this imputed model (HR 0.83 (0.78 to 0.89)) remained. When examining 30-day mortality, South Asians still had a better survival than white subjects (HR 0.85 (0.77 to 0.94), adjusted for age (as a continuous variable), sex, smoking, diabetes, hypertension, hypercholesterolaemia, Index of Multiple Deprivation and ACS phenotype).
Discussion
Objective addressed
The available evidence which we present here strongly suggests that South Asian ethnicity has a different effect on incidence and prognosis. Our systematic review and meta-analysis demonstrate that the prognosis of coronary disease is better among South Asian compared with white patients after adjustment for age, risk factors and disease severity. This is in contrast to the higher incidence of disease in South Asian compared with white populations. This dissociation between aetiology and prognosis has implications for public health and prevention strategies within healthcare settings.
Meta-analyses demonstrates discordance
Our meta-analyses robustly address our research objective: that incidence and prognostic effects are discordant. We acknowledge that for incidence we used both general populations combined with populations with a risk factor (such as diabetes) albeit with no coronary disease but by definition these studies are in the same group because they fulfil our criteria of answering questions of coronary disease onset. To examine incidence of coronary disease yet exclude data from people with diabetes, an important group among both ethnic groups, we feel would be a significant omission. We separately report both chronic and acute coronary disease in the prognostic meta-analysis because of the possibility that South Asians with acute myocardial infarction might die before reaching hospital more often than white subjects. In our three chronic coronary disease cohorts we found an overall protective effect, though those in the Whitehall study had a worse prognosis Those presenting to chest pain clinic or undergoing coronary angiography are clearly different populations from those (in Whitehall II) reporting symptoms of angina, and this might contribute to differences in the point estimates. Furthermore, Fischbacher et al22 found that sudden death in the community was less likely among South Asians (16.7%, 21/126) compared with white subjects (31.2%, 9672/30978). Thus, the possibility that South Asians with acute myocardial infarction might die before reaching hospital more often than white subjects is not substantiated. We found that more recent studies, which were larger and more detailed in their adjustments for confounders, reported that prognosis was better in South Asians than in white subjects.11 ,22 We found considerable heterogeneity in both studies of incidence and prognosis, arising from differences of population selection, differing outcomes and measurement of and adjustment for confounders. This means that precise, unbiased estimates of the magnitude of effect of South Asian ethnicity on incidence or prognosis will require larger and better studies. However, with the available evidence that we present here, we can infer that there is a qualitative difference in direction of effect of South Asian ethnicity between incidence and prognosis.
International literature in meta-analyses
A further finding from our systematic review and meta-analysis was that only the UK and Canada produced eligible studies. There are other high-income countries (such as Australia, Singapore, Norway and the USA) to which South Asians migrate. This is important because some studies comparing South Asian and white overall coronary mortality suggest a contextually-specific relation according to the country of migration.37 These studies however did not distinguish incidence and prognosis and were not therefore eligible for inclusion in our systematic review. We are unable to account for whether migrants to the UK and Canada are in anyway different, but it is of interest to observe that the most recent and largest studies on prognosis in the UK (our ACS cohort) and in Canada11 both revealed a better prognosis in South Asians, while older and smaller studies in each country did not.
Diabetes in ACS cohort
We found in our ACS cohort that the impact of diabetes for worse survival after ACS was stronger in South Asians than white subjects within the ACS cohort: this is consistent with evidence from other studies that glycaemic control is poorer,38 and the risk of diabetes complications such as end-stage renal disease higher, in South Asians compared with white subjects.39 This makes the better prognosis we observed in the ACS cohort among South Asians, both diabetic and not, particularly surprising. These findings in our ACS cohort are consistent with others who also demonstrate that South Asian patients with diabetes experience a significantly lower death rate following hospitalisation for ACS compared with white patients with diabetes.40
Case mix in ACS cohort
We examined whether age, type of ACS or severity of ACS might explain our findings. To account for the younger age of South Asians at presentation, we presented results age-adjusted and age-adjusted within age strata, and found that this did not account for their better survival. We were able to examine whether South Asians had less severe presenting manifestations of ACSs. The profile of ACS type did differ by ethnic group, with more unstable angina and less NSTEMI among South Asians, but this did not explain why South Asians had a better prognosis. We found that the effect of South Asian ethnicity on 30-day mortality remained beneficial as per that of 1-year mortality. If South Asians did have unmeasured differences in acute disease severity, we hypothesise that the 30-day effects should have been more marked. The category ‘unstable angina’ in South Asians may also have included more non-cardiac diseases such as oesophageal reflux due to misdiagnosis and the known higher prevalence of atypical pain in this group,31 but even after excluding this relatively small group from analyses, prognosis remained better among South Asians.
Quality of care in ACS cohort
We found South Asians were more likely to be on all four secondary prevention medications at discharge and were more likely to have had received coronary angiography or this procedure planned. Thus, these data do not suggest a negative differential access to treatment in South Asians and may reflect physician knowledge of a heightened awareness of coronary risk in South Asians. Previous work by others on this ACS cohort has reported that South Asian patients were less likely to arrive by ambulance but more likely to receive thrombolysis, with no evidence of a delay in receiving thrombolysis after arrival at hospital in South Asians.41 The better survival observed in South Asians in the most deprived areas and in those areas with the highest ethnic density may reflect enhanced care provided by hospitals more focused on South Asian health, their geographical proximity to hospitals, better community support and more ethnic-specific services, which are data not available in the ACS cohort. Overall, however, the finding of equivalent care between South Asians and white subjects and the better survival in South Asians is encouraging and suggests that inequalities that might result from differences in care can be remedied.
Heterogeneity of effects within South Asian groups
A further contribution of the ACS cohort was the ability to test whether there are differences between South Asian component groups in association with prognosis. We show in the ACS cohort that patients of Indian, Pakistani and Bangladeshi origin all have better prognosis compared with white subjects, although for Bangladeshis the CIs spanned unity. For the meta-analysis, we excluded studies that disaggregated the South Asian group into its component groups for ease of comparison, as the vast majority of work in this field to date uses the combined ethnic group definition. We appreciate that analyses by South Asian component groups are of real importance, and other studies on incidence suggest that Pakistani and Bangladeshi populations may have a higher incidence of cardiovascular disease compared with Indians.42–45
Strengths and weaknesses of the ACS study
Our cohort has strengths: it is the largest yet reported and unlike previous similar studies contained data on risk factors and clinical management (both drugs and invasive procedures), socio-economic deprivation and acute disease severity data. However, our study lacked data on more detailed phenotyping (acute angiographic findings, other biomarkers), longitudinal patterns of risk lowering interventions and cause of death. Ethnicity was not self-defined in this ACS cohort and would have been logistically very hard to do so but the baseline characteristics (such as the high prevalence of diabetes in Asians) confirms that the ‘Asian’ category was likely to be mostly comprised of South Asians. In order to better understand how South Asian ethnicity influences the onset and progression of coronary and other cardiovascular diseases there is a role for much larger scale cohort studies which may be identified through linkage of primary care, ACS registry, hospitalisation and cause-specific death data.16 Such studies will allow longitudinal patterns of risk, and missed opportunities to lower risk (before admission and after discharge) to be evaluated.
Implications for clinicians and policy makers
Clinicians and the health systems in which they work have repeatedly been criticised for providing inequitable care and outcomes to different groups in society: we provide strong evidence of a situation where this does not occur that ethnic inequalities in health are not inevitable. The dissociation between the aetiological and prognostic findings suggests that public health policy to reduce ethnic inequalities in coronary mortality needs to concentrate on reducing ethnic inequalities in disease incidence (ie, primary prevention) as provision of healthcare to those with disease (ie, a range of secondary preventive measures influencing prognosis) appears not to be unequal.
Conclusions
The available evidence reviewed here suggests that the higher overall cross-sectional coronary death rates in the South Asian population are due to higher incidence rather than a worse prognosis. Public health efforts to reduce South Asian ethnic inequalities in overall coronary mortality need a heightened focus on primary prevention.
Key messages
-
Meta-analysing data from all previous comparative studies of South Asians and white populations, South Asian ethnicity exerted a strong effect on the incidence of coronary disease, but their prognosis was not worse once coronary disease was manifest.
-
From analyses within an acute coronary syndrome cohort, South Asians had a better prognosis than white subjects irrespective of diabetic status and South Asian patients were not undermanaged for coronary disease.
Acknowledgments
We acknowledge the contribution of the MINAP group, including the Academic Group and Steering Committee, and the National Institute of Cardiovascular Outcomes Research (NICOR). The authors would like to thank Bridget Cole, Librarian at the Norfolk and Norwich University Hospital, for her expert assistance on the systematic review and Marina Daskalopoulou for assistance with the Forest plots.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
-
Collaborators None.
-
Contributors MJZ and HH had the original idea. MJZ and AF performed the systematic review. MJZ and PP did the statistical analyses. MJZ wrote the first draft and is the guarantor. RC and MS were involved in further analysis. ADT and MM were involved in the discussion and interpretation. HH contributed to the first draft and analysis, and was involved in the discussion and interpretation. All authors participated in the discussion and interpretation of the final results and contributed to the final paper.
-
Funding MJZ was supported by a National Institute for Health Research Clinical Lectureship and a UCLH Clinical Research and Development Committee Project Grant (GQPT). MJS is supported by the British Heart Foundation. This study was supported by grants from the UK National Institute for Health Research (RP-PG-0407-10314) and the Wellcome Trust (086091/Z/08/Z) which funds the Cardiovascular disease research using LInked Bespoke studies and Electronic Records (CALIBER) programme. The funding bodies were not involved in study design or analysis. We acknowledge the use of the UCL Legion High Performance Computing Facility, and associated support services, in the completion of this work.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement The MINAP data are accessible through the MINAP academic group after a peer-reviewed application process.
-
Disclaimer None.
-
Patient consent/Ethics approval statements not required as paper is a systematic review, and MINAP data has National Patient Information Advisory Group and Central Office for Research Ethics Committees approval for individual patient anonymous linkage for mortality and no patient identifiers are given out to researchers.