Article Text

Abstract
Objective To define the incidence and risk factors for infective endocarditis (IE) following surgical aortic valve replacement (SAVR) and transcatheter aortic valve implantation (TAVI).
Methods All patients who underwent first SAVR or TAVI in England between 2007 and 2016 were identified from the NICOR databases. Hospital admissions with a primary diagnosis of IE were identified by linkage with the NHS Hospital Episode Statistics database. Approval was obtained from the NHS Research Ethics Committee.
Results 2057 of 91 962 patients undergoing SAVR developed IE over a median follow-up of 53.9 months—an overall incidence of 4.81 [95% CI 4.61 to 5.03] per 1000 person-years. Correspondingly, 140 of 14 195 patients undergoing TAVI developed IE over a median follow-up of 24.5 months—an overall incidence of 3.57 [95% CI 3.00 to 4.21] per 1000 person-years. The cumulative incidence of IE at 60 months was higher after SAVR than after TAVI (2.4% [95% CI 2.3 to 2.5] vs 1.5% [95% CI 1.3 to 1.8], HR 1.60, p<0.001). Across the entire cohort, SAVR remained an independent predictor of IE after multivariable adjustment. Risk factors for IE included younger age, male sex, atrial fibrillation, and dialysis.
Conclusions IE is a rare complication of SAVR and TAVI. In our population, the incidence of IE was higher after SAVR than after TAVI.
- transcatheter aortic valve replacement
- aortic valve stenosis
- endocarditis
Data availability statement
Raw data are not available due to restrictions on data sharing imposed by NICOR and NHS Digital.
Statistics from Altmetric.com
Introduction
Infective endocarditis (IE) is a life-threatening complication of prosthetic valve replacement which affects approximately 3–10 per 1000 person-years.1 2 In the last 15 years, transcatheter aortic valve implantation (TAVI) has revolutionised the treatment of aortic stenosis, leading to an expanded population with prosthetic valves. The reported incidence of IE in patients with prosthetic valves is over 100 times that of the general population,3 and this risk may be even higher in elderly patients undergoing frequent hospitalisation and invasive medical procedures.4
To date, few studies have systematically evaluated the population risk of IE after TAVI and SAVR over long-term follow-up. Insights concerning risk factors for IE have largely been limited to registry studies and clinical trial populations with attendant selection bias or incomplete follow-up.5–8 There is ongoing uncertainty as to which patients with prosthetic valves are most susceptible to IE and how to reduce this risk.9 Unlike in Europe and the USA, routine oral antibiotic prophylaxis for at-risk patients undergoing invasive dental procedures has not been recommended in the UK since 2008.10 11
In this study, we use linked national registry data to provide insights into the epidemiology of IE following TAVI (TAVI-IE) and surgical aortic valve replacement (SAVR-IE) in England. The primary aims were (1) to understand the relative incidence of IE after SAVR and TAVI, and (2) to determine the risk factors for developing IE in each population.
Methods
Design
We performed a retrospective cohort study using database linkage to identify all first episodes of IE in a consecutive series of patients undergoing TAVI or SAVR in England. Ethical approval for the study was provided by the London Bromley Research Ethics Committee (reference 16/LO/0275) and the National Health Service confidentiality advisory group (reference 17CAG0001).
Study populations
All patients undergoing first TAVI or SAVR (±coronary artery bypass grafting, CABG) between 1 January 2007 and 31 December 2016 in England were identified from the National Institute for Cardiovascular Outcomes Research (NICOR) TAVI and Adult Cardiac Surgery databases, respectively. These data are submitted by implanting clinical teams, with case ascertainment performed centrally by NICOR.12 We extracted data concerning baseline patient demographics (age, sex), comorbidities (smoking, atrial fibrillation, previous percutaneous coronary intervention, kidney disease, lung disease, prior cardiac surgery) and key procedural variables for TAVI (valve type, post-deployment hemodynamics) and SAVR (valve type, procedural urgency, concurrent CABG). Patients undergoing repeat SAVR or valve-in-valve TAVI were excluded.
Cases
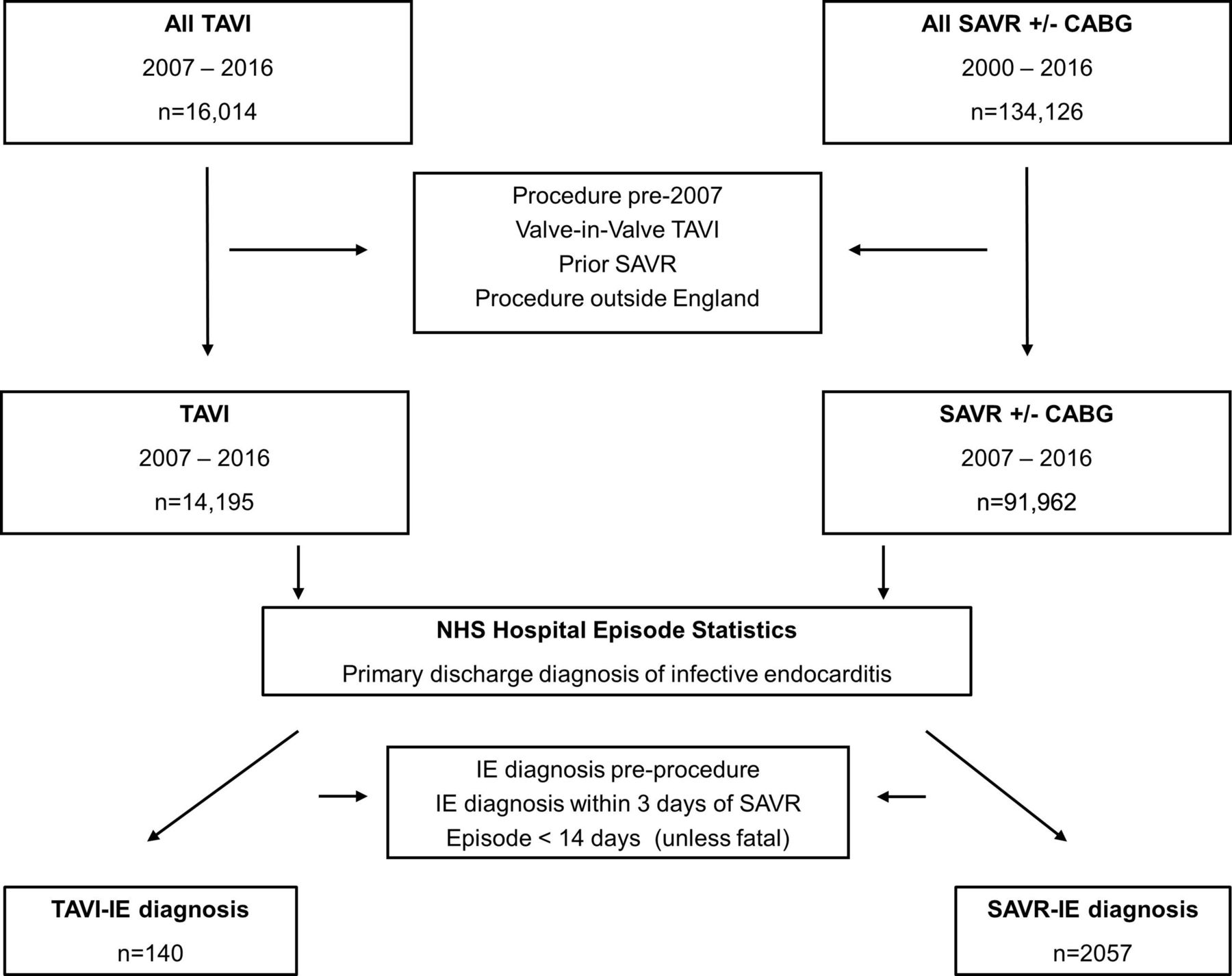
The National Health Service (NHS) records a primary discharge diagnosis using the ICD-10 coding system in the NHS Digital Hospital Episode Statistics Admitted Patient Care database (HES APC) for all patients admitted to hospital in England. We used linkage between the NICOR datasets and HES APC to identify patients hospitalised with a primary discharge diagnosis of “acute or subacute infectious endocarditis” (ICD-10 I33.0), “endocarditis, valve unspecified” (ICD-10 code I38) or “endocarditis and heart valve disorders in diseases classified elsewhere” (ICD-10 code I39), from any date up to 1 May 2017 (figure 1). NHS Digital performed linkage using a deterministic algorithm to match patients by exact NHS number and at least one other identifier (date of birth and sex).
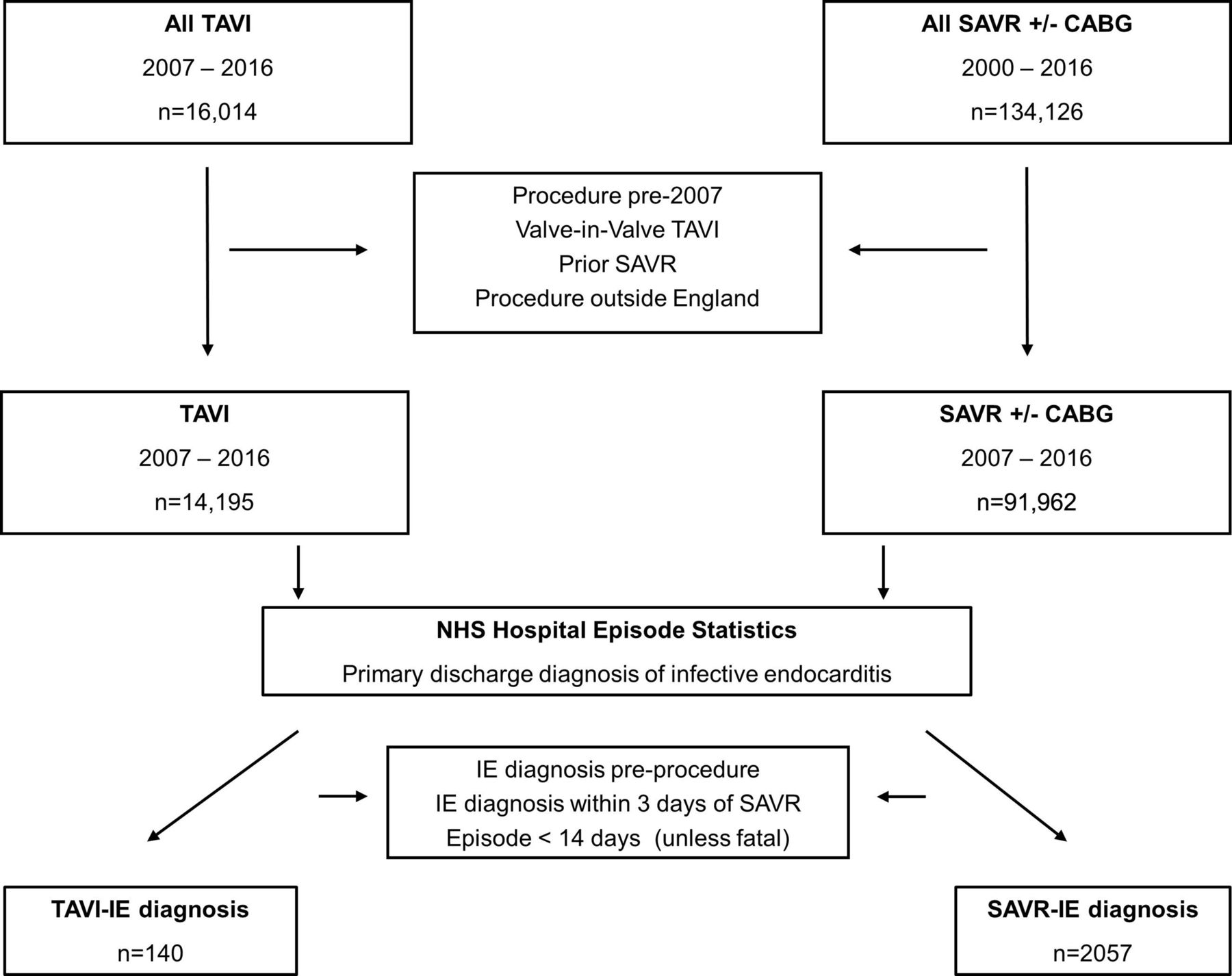
Flowchart of the study cohorts.
All patients with a known episode of IE (based on HES APC episodes, from 1999 onwards) prior to first SAVR or TAVI were excluded from the analysis. The first admission with IE after SAVR/TAVI was used to calculate time to IE. To reduce the possibility of including cases where SAVR may have been undertaken for the treatment of IE, the diagnosis of SAVR-IE had to be established a minimum of 72 hours after the time of surgery. Only first admissions were included: by searching individual patient level data, we were able to identify when patients admitted to one hospital were transferred to another, and these continuous periods of illness (so called ‘superspells’) were counted only once. Only admissions of ≥14 days’ duration were included, unless fatal, to improve the specificity of the diagnosis.
Outcomes
The primary outcome was the incidence of IE during follow-up, analysed as cumulative incidence and incidence rate per 1000 person-years.
Statistical analysis
Continuous data are expressed as mean±SD or median with IQR. Categorical data are presented as absolute number with percentage. Comparison between groups was performed using the Fisher exact or χ2 test for categorical variables (with Fisher exact used preferentially), and Student’s t-test for continuous variables. A p value <0.05 was defined as significant. All tests were two sided. Cumulative incidence of IE was calculated in the competing risk setting, using death as a competing risk. Time-to-event data analysis was performed using a Cox proportional hazards model, with Kaplan-Meier survival curves drawn to assess differences between groups for the time to an event. Models were checked for violation of the proportional hazards assumption by assessing log-minus-log survival plots and scaled Schoenfield residuals. For Cox modelling, single variable analysis was used to examine the independent effect of clinical factors on outcome, and only those variables which were significant at p<0.1 were included in the multivariable model. For multivariable models, a backward elimination model was used to identify significant risk factors, and independent variables with p value >0.1 were sequentially excluded. Also, 95% CIs were calculated. Missing data were assumed to be missing completely at random. Patients with ≥10% missing data for the covariate of interest were excluded. Where there was <10% missing data, imputation was performed for the multivariable model using a Markov chain Monte Carlo approach implemented in SPSS. Data were analysed with SPSS V.22.0 and R V.3.6.3 (R: a language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria, http://www.R-project.org).
Results
Incidence of IE after SAVR and TAVI
Between 1 January 2007 and 31 December 2016, a total of 14 195 TAVI and 91 962 SAVR procedures were performed across England (figure 1). As anticipated, there were significant differences in the demographics of patients undergoing TAVI and SAVR (online supplemental table 1). Patients undergoing TAVI had a median age of 83.0 (IQR 77.0–86.0) years, compared with a median age of 72.0 (IQR 63.9–78.1) in the SAVR cohort (p<0.0001). The TAVI cohort had a significantly higher surgical risk (median logistic Euroscore 16.1 [IQR 10.7–25.3] vs 5.8 [IQR 3.3–10.1)], p<0.001). In the SAVR cohort, 33,527/92,961 (36.1%) underwent concomitant coronary artery bypass grafting (CABG) and 7202/92,961 (7.7%) underwent greater than one valve intervention.
Supplemental material
There were 2057 cases of IE after SAVR (SAVR-IE) over a median follow-up of 53.9 (IQR 22.3–88.8) months, giving an incidence rate of 4.81 (95% CI 4.61 to 5.03) per 1000 per-years (figure 2). In comparison, there were 140 cases of IE after TAVI (TAVI-IE) over a median follow-up of 24.5 (IQR 8.2–54.0) months, corresponding to an incidence rate of 3.57 (95% CI 3.00 to 4.21) per 1000 person-years. The cumulative incidence of IE at 60 months was 2.4% (95% CI 2.3% to 2.5%) for SAVR compared with 1.5% (95% CI 1.3 to 1.8) for TAVI (HR 1.6, p<0.001; figure 2). The median time to IE was 12.9 (IQR 1.78–42.0) months after SAVR and 10.15 (IQR 4.05–21.7) months after TAVI. The distribution of time to IE following SAVR and TAVI is shown in online supplemental figure 1.
Supplemental material

{kind=link}
{kind=link}
Cumulative incidence of IE in patients after surgical aortic valve replacement (SAVR) and transcatheter aortic valve implantation (TAVI).
Patient demographics according to the presence of IE are shown in table 1. For both SAVR and TAVI, patients with IE were younger (TAVI: 81.5 [IQR 75.8–85.0] vs 83.0 [IQR 77.0–86.0], p=0.02; SAVR: 69.5 [IQR 59.5–76.6] vs 72.0 [IQR 64.0–78.2], p<0.0001) and a higher proportion of IE cases occurred in males (TAVI 69.3% vs 53.3%, p=0.0002; SAVR 71.4% vs 63.7%, p<0.0001). In the SAVR cohort, patients with IE were more likely to be on dialysis, have a history of prior PCI, smoking or atrial fibrillation, have impaired LV function and had a higher logistic Euroscore. There was no difference in the proportion of patients with SAVR-IE according to valve type (p=0.2). Concomitant CABG was associated with a lower rate of IE (29.0% vs 36.6%, p<0.0001).
Baseline patient and procedural factors according to the occurrence of infective endocarditis
Risk factors for IE after TAVI
In patients undergoing TAVI, Cox regression modelling was performed to identify baseline clinical and procedural factors associated with subsequent IE. On univariable analysis, younger age, male sex, valve design and increasing post-deployment peak gradient were associated with subsequent TAVI-IE (table 2). Factors which retained statistical significance on multivariable analysis were younger age (per year, HR 0.98, 95% CI 0.96 to 0.99, p=0.01), male sex (HR 1.83, 95% CI 1.26 to 2.64, p=0.001), implantation of a mechanically expandable valve (compared with self-expandable valve, HR 3.14 [95% CI 1.85 to 5.35], p<0.001) and increasing residual peak gradient after TAVI (per mmHg, HR 1.002 [95% CI 1.00 to 1.005], p=0.04).
Cox regression analysis of factors associated with occurrence of TAVI-IE
Risk factors for IE after SAVR
In patients undergoing SAVR, Cox regression modelling was performed to identify baseline factors associated with subsequent IE. On univariable analysis, younger age, male sex, current smoking, elevated body mass index (BMI >30 kg/m²), atrial fibrillation, higher serum creatinine, current dialysis, elevated logistic Euroscore (greater than the median) and non-elective surgery were associated with subsequent SAVR-IE (table 3). On multivariable analysis, factors that retained statistical significance as predictors of IE were younger age (per year, HR 0.97, 95% CI 0.97 to 0.98, p<0.001), male sex (HR 1.39, 95% CI 1.21 to 1.60, p<0.001), elevated BMI (1.13, 95% CI 0.99 to 1.29, p<0.01), atrial fibrillation (HR 1.30, 95% CI 1.09 to 1.54, p<0.01), current dialysis (HR 2.36, 95% CI 1.13 to 4.97, p=0.03), elevated logistic Euroscore (HR 1.88, 95% CI 1.64 to 2.15, p=0.02) and a non-elective procedure (HR 2.19, 95% CI 1.92 to 2.48, p<0.01). Concomitant CABG was associated with a lower risk of future IE (HR 0.64, 95% CI 0.56 to 0.74, p<0.01).
Cox regression analysis of factors associated with SAVR-IE
Risk factors for IE across all patients undergoing aortic valve replacement
Across the entire cohort undergoing aortic valve replacement by TAVI or SAVR (n=106 157), there was an increased risk of IE in patients undergoing SAVR on univariate analysis (HR 1.65, 95% CI 1.39 to 1.96, p<0.001). The increased risk of IE in patients undergoing SAVR was consistent across subgroups, although a significant interaction was identified with procedural urgency and renal function (online supplemental file 3). Multivariable analysis was then performed, with procedural urgency treated as an interaction term (table 4). Creatinine was excluded from the multivariable analysis due to additional interaction with dialysis. On multivariable analysis, factors which retained statistical significance as predictors of IE were younger age (per year, HR 0.98, 95% CI 0.98 to 0.99, p<0.001), male sex (HR 1.30, 95% CI 1.17 to 1.44, p<0.001), atrial fibrillation (HR 1.39, 95% CI 1.23 to 1.58, p<0.001), higher logistic Euroscore (per point, HR 1.004, 95% CI 1.000 to 1.001, p=0.01), and both elective SAVR (HR 1.86, 95% CI 1.23 to 2.83, p=0.003) and urgent SAVR (HR 3.54, 95% CI 2.33 to 5.38, p<0.001) compared with elective TAVI.
Supplemental material
Cox regression analysis of factors associated with IE for all patients undergoing SAVR or TAVI
Discussion
The key findings of this study are as follows: (1) in an unselected consecutive nationwide population over long-term follow-up, the risk of IE following SAVR was 4.81 per 1000 person-years, and after TAVI was 3.57 per 1000 person-years; (2) this difference in the incidence of SAVR-IE and TAVI-IE was small but statistically significant, with SAVR remaining an independent predictor of IE across the entire cohort; (3) risk factors for IE among all patients undergoing aortic valve replacement (SAVR or TAVI) included younger age, male sex, atrial fibrillation, dialysis and an elevated logistic Euroscore; (4) specific risk factors for TAVI-IE included patients with mechanically expandable valves and those with an elevated post-deployment residual gradient.
Incidence of IE following SAVR and TAVI
Several prior studies have compared the incidence of IE after SAVR and TAVI (table 5).13–18 Observational analyses using the United States Readmissions Database,13 Danish National Patient Registry,14 the FinnValve Registry15 and a pooled analysis from the PARTNER trials16 identified no difference in the incidence of IE over a follow-up period of 5–44 months. A large study of 107 786 patients in France identified a numerically higher incidence of IE after TAVI compared with SAVR, but this difference was not statistically significant after propensity score matching.17 In contrast, a pooled analysis from three randomised controlled trials of the self-expanding CoreValve transcatheter heart valve family against SAVR reported a higher cumulative incidence of IE after SAVR compared with TAVI over a mean follow-up of approximately 2 years.18
Summary of studies comparing the incidence of infective endocarditis after SAVR or TAVI
The incidence of IE after SAVR and TAVI in our cohort was extremely low and similar to incidence derived from pooled analyses of the PARTNER16 and CoreValve trials,18 in which patients had an adjudicated diagnosis of IE. The mechanisms behind an apparent excess of IE cases after SAVR compared with TAVI seen in our cohort (and the CoreValve trials) are currently unclear and require further investigation. One possible explanation is that the risk of IE post-TAVI might be less than for SAVR because of the lack of an open sternotomy wound and reduced need for invasive monitoring following the procedure.
Risk factors for IE after aortic valve replacement
Several risk factors for IE were identified across the entire cohort undergoing aortic valve replacement, including younger age, male sex, atrial fibrillation, dialysis and increased logistic Euroscore. Male sex has previously been reported as a risk factor for prosthetic valve IE after both SAVR and TAVI.6 19 20 The underlying mechanism is unclear and may be driven by differences in the burden or frequency of bacteraemia, immune response or aortic anatomy.21 Patients on dialysis were at markedly increased risk of IE (likely due to bacteraemia arising from indwelling lines or dialysis) and represent a key group in whom novel preventative strategies should be targeted.22
Specific risk factors for IE after SAVR and TAVI
In patients undergoing SAVR, elevated body mass index was a specific risk factor for IE. Obesity is a well-established risk factor for sternal wound infection after cardiac surgery, and this may explain the increased risk of IE in this subset.20 We did not observe an association between the type of surgical valve implanted and future IE, in contrast to a prior observational study that suggested increased risk associated with bioprosthetic valves (in comparison with mechanical valves).19 Unexpectedly, we found that concomitant CABG at the time of SAVR was associated with reduced risk of future IE, a finding which requires further validation.
In patients undergoing TAVI, elevated post-deployment gradient was associated with increased risk of IE. Consistent with these findings, an elevated post-deployment gradient (>15 mmHg) has been identified as a risk factor for IE following transcatheter pulmonary valve implantation.23 Elevated transvalvular gradients may lead to turbulent flow and endothelial damage, which then acts as a nidus for vegetation formation.24 Indeed, there may be a role for aggressive post-dilatation to minimise the residual transvalvular gradient. Mechanically expandable valves were also associated with increased risk in our series. Previously, self-expanding valves have also been identified as a risk factor for TAVI-IE, and further studies of the risk associated with different valve designs are required to resolve this discordance.5 Current expert consensus for prevention of TAVI-IE focuses on antibiotic prophylaxis at the time of implantation, careful patient preparation and sterile implant technique.25
Limitations
We used hospital discharge coding data to identify IE cases and there is a possibility that our incidence estimates are underestimates. Reported estimates for coding accuracy for IE vary, with a range for sensitivity of 56%–79% and specificity of 94%–100%.26 27 In our population, coding was performed independently by trained and accredited personnel. Despite our efforts to mitigate against this, it is possible that some cases of SAVR undertaken as treatment for native aortic valve IE may have been miscoded as SAVR-IE. For both cohorts, there are missing data for some variables (as indicated), which we have assumed is missing completely at random. For multivariable modelling, we cannot exclude the possibility of residual confounding accounting for our observations.
Given the very substantial differences in comorbidities and risk scores of the populations undergoing TAVI and SAVR during the period of our study, including both measured and unmeasured variables, we have elected to avoid propensity score matching but present the raw analyses for interpretation. Although the median follow-up time for the SAVR cohort was longer than for TAVI, the risk of IE appeared to be early after valve intervention, and we do not believe that this affected the difference in (adjusted) incidence rate.
Conclusions
IE is a rare adverse outcome following aortic valve replacement which may be slightly less common after TAVI than after SAVR. Key risk factors for IE in patients undergoing aortic valve replacement include younger age, male sex, atrial fibrillation and dialysis. Further research is required to translate insights into this condition into novel preventative strategies.
Key messages
What is already known on this subject?
Prosthetic valve infective endocarditis (IE) is a potentially life-threatening complication of aortic valve replacement. The relative incidence of IE after SAVR and TAVI, and risk factors for developing prosthetic valve IE, are poorly defined.
What might this study add?
Prosthetic valve IE was rare, affecting approximately 2% of patients 5 years following aortic valve replacement. The incidence of IE in our population was slightly lower in patients undergoing TAVI compared with SAVR. Risk factors for IE across the study cohort included younger age, male sex, atrial fibrillation and dialysis. In patients undergoing SAVR, elevated body mass index (>30 kg/m²) and higher logistic Euroscore were also identified as risk factors for IE. In patients undergoing TAVI, implantation of a mechanically expandable valve and an elevated post-implantation peak aortic gradient were specific risk factors for subsequent IE.
How might this impact on clinical practice?
All patients undergoing aortic valve replacement should be educated about the risk of IE, and these efforts should be amplified in at-risk groups. Further research is required to understand the mechanisms by which IE occurs and translate these insights into novel preventative strategies.
Data availability statement
Raw data are not available due to restrictions on data sharing imposed by NICOR and NHS Digital.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and received Ethical Approval from the London Bromley Research Ethics Committee (reference 16/LO/0275) and the United Kingdom confidentiality advisory group (reference 17CAG0001). These data were acquired retrospectively. Given the high mortality associated with infective endocarditis, we applied to the UK Confidentiality Advisory Group to use anonymised data without consent as it was felt to be not practical to request individual patient consent when a large proportion of patients would already be deceased. This permission was granted after review of the research protocol.
Acknowledgments
The authors are grateful to all clinicians who supported this study. We also acknowledge the staff at NHS Digital and NICOR who assisted with data procurement and linkage.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @tomjcahill, @j_sandoe
Correction notice This article has been corrected since it was first published. The total number of SAVR cases in Figure 1 and 2 has been corrected to 91962, as per the main text.
Contributors TJC, PL, DJRH-S, SRR and BDP conceived and designed the study. TJC, JR, PDJ, PFB, APB, JB, RKK, PAM, MHT, JATS, MSS, PL, DJRH-S, SRR and BDP performed data extraction and/or analysis. TJC and BDP wrote the first draft of the manuscript and all authors reviewed, interpreted and commented on the final version. All authors agree with the results and conclusions of the manuscript and meet the ICMJE criteria for authorship. TJC and BDP are guarantors for the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests BDP has received unrestricted education and research grants from Edwards Lifesciences and speaker fees from Edwards Lifesciences. SRR has served as a proctor for and received speaker fees from Edwards Lifesciences, and has served on the advisory board for Medtronic. All other authors declare no competing interests.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.