Article Text

Abstract
Objective The aim of this study was to examine the association between age at onset of overweight and incident hypertension.
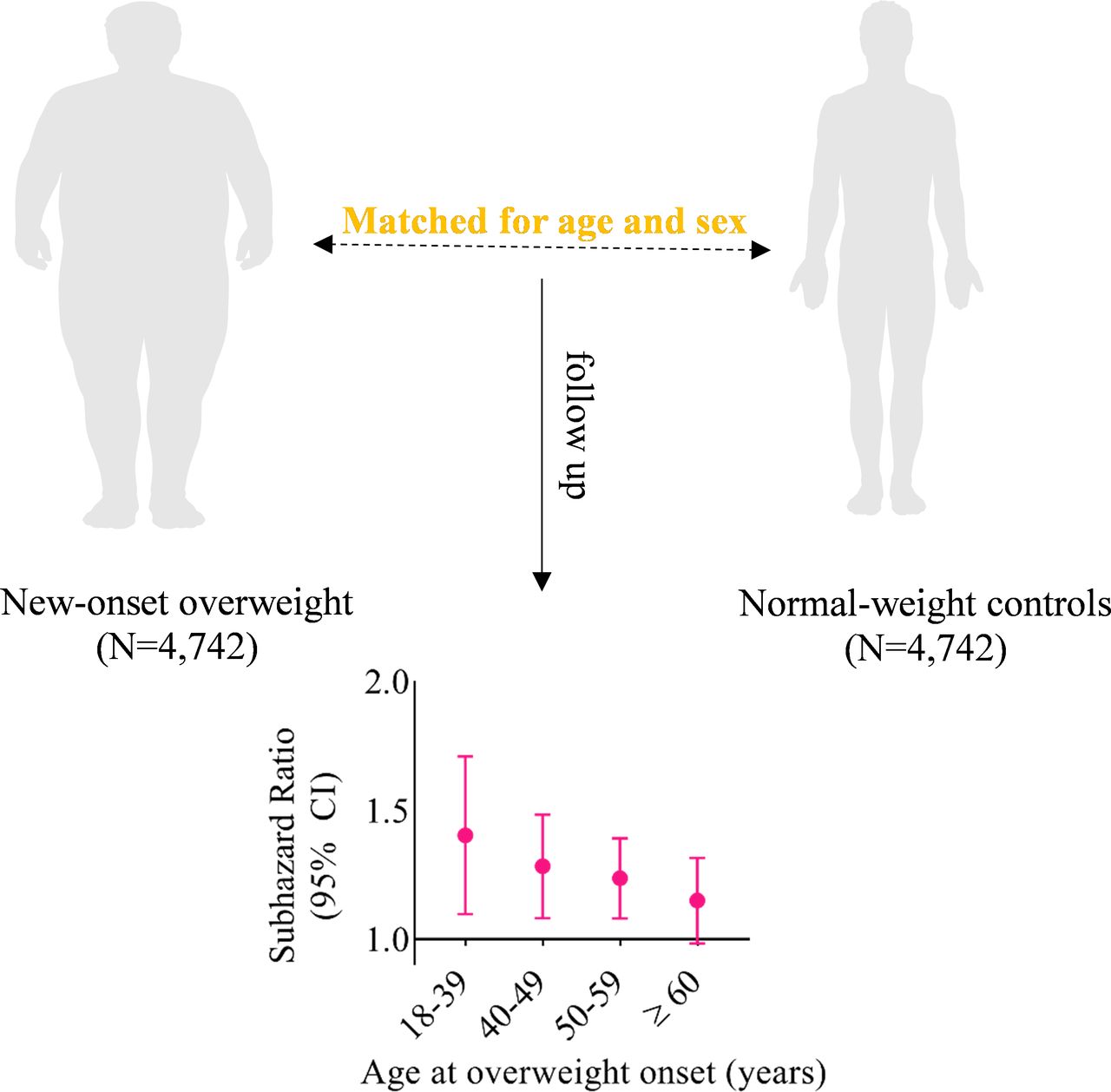
Methods We analysed 4742 participants with new-onset overweight from the Kailuan study between 2006 and 2015 and and 4742 age-matched and sex-matched controls selected randomly from the same cohort but with normal weight. Participants were compared with respect to subsequent risk of hypertension, with sub-HR calculated with the Fine and Gray model, according to age of onset of overweight.
Results Over a mean follow-up period of 5.17 years, 1642 overweight participants (34.6%) and 1293 normal-weight controls (27.3%) were subsequently diagnosed with hypertension. The median age at onset of overweight was 49.1 years. Compared with normal-weight controls, the multivariable-adjusted sub-HR for hypertension among participants with onset of overweight at 18–39 years of age, 40–49 years of age, 50–59 years of age and ≥60 years of age was 1.38 (95% CI 1.11 to 1.72), 1.27 (95% CI 1.09 to 1.49), 1.23 (95% CI 1.09 to 1.38) and 1.14 (95% CI 0.99 to 1.32), respectively. Onset of overweight in each age range was significantly associated with increased risk of hypertension, except for the group with onset at ≥60 years of age. The risk increased with each decade of attenuation of age at onset, peaking at 18–39 years of age.
Conclusions Younger age at onset of overweight across adulthood was associated with significantly increased risk of hypertension, with the highest relative risk among participants with onset of overweight at 18–39 years of age.
- hypertension
- risk factors
- epidemiology
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
The increasing trend in the prevalence of excess weight gain is worrisome and a worldwide challenge.1 2 It is well established that overweight, defined as increased body mass index (BMI), is associated with increased risk of high blood pressure.3–6 Moreover, because the onset of overweight in adulthood is occurring at increasingly younger ages,7 this is likely to translate into a high cumulative incidence of hypertension. This raises the question as to whether younger age at onset of overweight is more detrimental to the risk of hypertension than weight gain occurring later in life.
Because younger individuals are experiencing a greater cumulative exposure to excess adiposity over the life course,8 understanding the effect of age at onset of overweight on the progression of hypertension is important. Emerging evidence has demonstrated that individuals who were overweight or obese during early adulthood or middle age were at higher risk of hypertension later in life, although no information on age at onset was provided in these studies.9 10 To our knowledge, the role of timing of onset of overweight remains weakly studied.
In the present study, we analysed longitudinal data spanning from early adulthood to older age to investigate whether age at onset of overweight is associated with differences in subsequent risk of hypertension.
Methods
Study population
The Kailuan study is an ongoing, community-based, prospective cohort designed to assess the determinants and progression of cardiovascular disease over time in 101 510 adults who were 18–98 years old between 2006 and 2007. We recruited participants from the employee and retiree populations of the Kailuan Group, a coal mining company in Tangshan, China. Participants were followed up every 2 years beginning from study inception by means of health assessments and questionnaires on demographic features, lifestyle factors, and medical and other health-related information. To date, participants have been re-examined 2 (2008–2009), 4 (2010–2011), 6 (2012–2013), 8 (2014–2015) and 10 (2016–2017) years after baseline. All participants provided written informed consent for inclusion in the cohort.
We excluded those with missing data on BMI or blood pressure at baseline or who were underweight (BMI <18.5 kg/m2), overweight (BMI 25.0–<30.0 kg/m2) or obese (BMI ≥30.0 kg/m2) at the baseline survey performed in 2006. Those whose BMI changed from normal weight to obesity (the timing of overweight was not recorded), or who were diagnosed with hypertension at or before the diagnosis of overweight, or who were unavailable for follow-up after the date of diagnosis of overweight were also excluded. No participants were excluded due to previous type 2 diabetes. Of the 74 254 excluded participants, 1820 (2.5%) were underweight, 22 638 (30.5%) were of normal weight, 40 328 (54.3%) were overweight, 7998 (10.8%) were obese and 1470 (2.0%) were missing data on BMI at baseline.
Among the 27 256 participants who had normal weight according to the initial survey (2006–2007), 4755 were diagnosed with overweight by 31 December 2015 (the fifth survey). The date of the examination that initially identified manifestation of overweight was used to define the age at onset. Each overweight participant was age-matched (±1 year) and sex-matched with one control selected randomly from the population with normal weight (BMI 18.5–<25.0 kg/m2) who attended the examination in the same year that overweight was found to have manifested. Follow-up for each matched pair began from the time when overweight first manifested to the date of incident hypertension, death or last available follow-up. For example, for a case confirmed with onset of overweight at 55 years of age in 2008, the matched control was randomly selected from those aged 54–56 years and with normal weight when they attended the re-examination in 2008 (both initiated the follow-up in 2008). Ultimately, a total of 4742 normal-weight participants and 4742 participants with new-onset overweight formed the analysis population (figure 1).

Flow chart of the study. BMI, body mass index.
Patient and public involvement
Patients or the public were not involved in the design, or conduct, or reporting or dissemination plans of our research.
Ascertainment of new-onset overweight
Weight status in adulthood was ascertained based on BMI (weight in kilograms divided by the square of height in metres) using cut-off points according to the WHO’s standard ranges (underweight, BMI <18.5 kg/m2; normal weight, BMI 18.5–<25.0 kg/m2; overweight, BMI 25.0–<30.0 kg/m2; obesity, BMI ≥30.0 kg/m2). New-onset overweight was defined as a participant whose BMI changed from normal weight to overweight during the 8-year period before the fifth survey. During inperson assessments, weight (to the nearest 0.1 kg) and height (to the nearest 0.1 cm) were measured with participants wearing light clothes but no shoes, using standardised equipment. BMI was then calculated as described above. Body weight and height were updated every 2 years through examination.
Assessment of hypertension
At clinical examinations, systolic and diastolic blood pressure were measured at least twice in the right arm according to standardised protocols, using calibrated mercury sphygmomanometers, after participants were allowed to rest in a seated position for 5 min. Blood pressure was then remeasured if the difference between the two measurements was ≥5 mm Hg. These measurements were averaged for analysis. We defined incident hypertension based on a self-reported physician diagnosis, antihypertensive drug use or elevated systolic/diastolic blood pressure (≥140/90 mm Hg).11 Hypertension status was ascertained at follow-up examinations after the start of the study. The final date for matched pair inclusion in the present study was 31 December 2015. Participants were followed until 31 December 2017 for incident hypertension.
Assessment of covariates
Detailed information on cigarette smoking habits, alcohol consumption habits, physical activity and several biochemical variables was updated every 2 years. The covariates were derived from the examination year at which each matched pair was confirmed. Cigarette smoking status and alcohol consumption status were both dichotomised as ever or never based on information obtained at each examination. Physical activity was defined as aerobic exercise performed three times per week or more. Parental history of hypertension was obtained by self-report. Fasting blood glucose, total cholesterol, triglycerides and serum creatinine were assayed using an autoanalyser (Hitachi 747, Hitachi, Tokyo, Japan) across all examinations. Estimated glomerular filtration rate (eGFR) was calculated using the Chronic Kidney Disease Epidemiology Collaboration creatinine equation.12
Statistical analysis
The association between overweight and incident hypertension was examined according to age at onset of overweight (18–39 years, 40–49 years, 50–59 years and ≥60 years) compared with the matched normal-weight controls in each age range. Regarding descriptive analyses, categorical variables are expressed as percentages and were compared using χ2, while continuous variables are expressed as mean (SD) or median (IQR) and were compared using analysis of variance or the Kruskal-Wallis test, as appropriate.
We assumed missing data as missing at random (MAR) and used the multiple imputations by chained equations method to account for missing covariates.13 We generated five imputed data sets and used Rubin’s rules to combine estimates across the data sets. The number of imputed missing data is shown in online supplemental table S1. The incidence rates of hypertension (per 1000 person-years) were calculated as the number of events divided by the number of person-years at risk, times 1000. The Fine and Gray proportional hazards model of death as a competing risk was used to estimate the sub-HR (sHR) associated with age at onset of overweight and hypertension.14 15 Analyses were performed with adjustment for systolic blood pressure (continuous), fasting blood glucose (continuous), total cholesterol (continuous), triglycerides (continuous), eGFR (continuous), parental history of hypertension (yes/no), cigarette smoking status (never/ever), alcohol consumption status (never/ever), physical activity (yes/no) and education attainment (less than high school, high school, college or more).
Supplemental material
We also performed a number of sensitivity analyses to assess the robustness of our findings. First, to assess potential reverse causality, we excluded hypertension that occurred within the first 2 years of follow-up. Second, we repeated analyses using Cox proportional hazards models. Third, we excluded individuals who did not remain overweight following its initial manifestation. Fourth, we excluded overweight individuals who progressed to obesity. Fifth, we accounted for time-varying covariates, including fasting blood glucose, total cholesterol, triglycerides and eGFR. Sixth, we also used the definition of overweight based on the International Obesity Task Force criteria for East Asians (BMI 23.0–<25.0 kg/m2). Lastly, under the missing not at random assumption, we applied pattern-mixture model approach to multiple imputation to assess the MAR assumption. Statistical analyses were performed using SAS V.9.4 software at a two-tailed alpha level of 0.05.
Results
Baseline characteristics
Of the 4742 eligible individuals with new-onset overweight and 4742 matched controls with normal weight, the number of participants in each age at onset category was as follows: 2206 at 18–39 years of age, 2510 at 40–49 years of age, 2974 at 50–59 years of age and 1794 at ≥60 years of age. The characteristics of the participants according to matching design are shown in table 1. According to matching design, the mean age and sex distribution of overweight participants and matched controls were similar. Compared with the normal-weight controls, overweight participants were more likely to have higher systolic blood pressure, fasting blood glucose, total cholesterol and triglycerides. The characteristics of the participants who developed overweight stratified according to age at onset are shown in table 2. The median age at onset was 49.1 (39.9–57.0) years. Among those who gained excess weight, those with younger age at onset of overweight were more likely to have higher levels of triglycerides and eGFR, to be ever smokers or drinkers of alcohol, to be physically inactive, and to have a higher proportion of parental history of hypertension.
Baseline characteristics of participants with new-onset overweight and their normal-weight controls
Baseline characteristics of participants with new-onset overweight across age groups (n=4742)
Incident hypertension
During a mean follow-up of 5.17 years (49 005.47 person-years), 1642 overweight participants (34.6%) and 1293 normal-weight controls (27.3%) were subsequently diagnosed with hypertension. The proportion of patients with hypertension by hypertension diagnostic criteria is reported in online supplemental table S2. The incidence of hypertension in overweight patients was 68.6 per 1000 person-years and in the controls was 51.6 per 1000 person-years. Figure 2 shows the incidence rates of hypertension per 1000 person-years in participants with new-onset overweight versus their corresponding controls within each age group. The cumulative incidence function curves for hypertension are depicted in online supplemental figures S1 and S2.

Incidence of hypertension per 1000 person-years in participants with new-onset overweight versus their corresponding controls within each age group. Error bars indicate 95% CI.
Unsurprisingly, the occurrence of overweight at any age was positively associated with increased incidence of hypertension, except in those 60 years of age or older. Compared with normal-weight controls, the multivariable-adjusted sHR of hypertension in participants with onset of overweight at 18–39 years of age was 1.38 (95% CI 1.11 to 1.72); in participants with onset of overweight at 40–49 years of age, the sHR was 1.27 (95% CI 1.09 to 1.49); in participants with onset of overweight at 50–59 years of age, the sHR was 1.23 (95% CI 1.09 to 1.38); and in participants with onset of overweight at ≥60 years of age, the corresponding sHR was 1.14 (95% CI 0.99 to 1.32). Notably, earlier age at onset of overweight was more strongly associated with subsequent risk of hypertension and the risk increased consistently with each decade of attenuation of age at onset, peaking at sHR of 1.38 at 18–39 years of age (figure 3).

Sub-HR for incident hypertension according to age at onset of overweight. Analyses were based on the Fine and Gray proportional hazards model of death as a competing risk and adjusted for systolic blood pressure, fasting blood glucose, total cholesterol, triglycerides, estimated glomerular filtration rate, parental history of hypertension, cigarette smoking status, alcohol consumption status, physical activity and education attainment, with matched controls served as the reference group.
Sensitivity analysis
The first sensitivity analysis and Cox proportional hazards models yielded results similar to those of the main findings (online supplemental tables S3 and S4). Furthermore, when we excluded those who did not remain overweight subsequent to its initial manifestation, the evidence for associations was largely strengthened, and even being overweight from age of 60 years or older was significantly associated with an sHR of hypertension of 1.29 (95% CI 1.07 to 1.57) (online supplemental table S5). According to the sensitivity analysis restricted to the subset of participants without progression to obesity, the results were similar, suggesting that excess weight gain in young adulthood affects hypertension risk, even in the absence of subsequent obesity (online supplemental table S6). Similar results were obtained after adjusting for time-varying covariates (online supplemental table S7). With the use of alternative definitions for overweight, the magnitude of the association was attenuated except for the 18–39 years age group (online supplemental table S8). The pattern-mixture model sensitivity analysis produced nearly identical results, suggesting that MAR assumption for the multiple imputation is plausible (online supplemental table S9).
Discussion
This community-based, longitudinal cohort study of 4742 patients newly diagnosed with overweight and 4472 age-matched and sex-matched controls showed that age at onset of overweight is an important determinant of incident hypertension. Younger age at onset of overweight was associated with higher sHR of hypertension, whereas late-onset overweight was not significantly associated with subsequent hypertension. Additionally, the risk of hypertension was continuously attenuated with each decade increase in age at onset of overweight (figure 4).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Key finding of the study
Studies on hypertension have primarily focused on change in weight status during childhood or adulthood,16–19 and studies that explicitly considered age at onset of overweight are scarce. Consistent with our results were those of the 1946 British birth cohort study, which showed that being overweight at a younger age was positively associated with higher blood pressure at 53 years.20 Additionally, results from the Johns Hopkins Precursors Study suggested that obesity in young adulthood (age 25 years) conferred a threefold risk of hypertension (HR, 2.79, 95% CI 1.30 to 6.00), whereas the risk was two times higher in men who became overweight or obese in midlife (age 45 years) compared with those of normal weight (HR, 1.91, 95% CI 1.46 to 2.49).9 Data from the Nurses’ Health Study and Health Professionals Follow-Up Study indicated that weight gain from young adulthood (ages 18 years for women and 21 years for men) to middle life (age 55 years) was associated with a higher risk of hypertension in both women (incident rate ratio (IRR), 1.24, 95% CI 1.20 to 1.28) and men (IRR, 1.21, 95% CI 1.12 to 1.31).10 Nonetheless, such existing findings may be susceptible to bias resulting from self-reporting or recalling body weight, or they were restricted to a narrow age window that did not extend beyond middle age. Additionally, other studies also observed an attenuated relationship between obesity and obesity-related hypertension with increasing age across adulthood, although the risks according to age at onset were not examined.21–23
The mechanisms underlying how age at onset of overweight contributes to hypertension remain unclear. Given that few individuals with young-onset overweight return to normal weight later in life,24 the strong association between hypertension and overweight in younger adulthood as opposed to later adulthood may be explained by longer duration of exposure to excess adiposity.25 It is well known that overweight and obesity arise from the interplay between genetic and environmental factors. In individuals with a very strong genetic cause, early-onset overweight has been associated with multiple genetic variants, which may influence susceptibility to hypertension. Another hypothesis is that early-onset overweight in those without a strong genetic component may reflect an unhealthy lifestyle, including smoking, alcohol consumption and physical inactivity, which substantially contributes to the risk of hypertension. Alternatively, the attenuated relationship may reflect decreased validity of BMI as a measure of adiposity due to age-related declines in height and muscle mass.26 Moreover, the increased prevalence of competing risk factors at older ages may reduce the proportional effect of BMI on subsequent risk of hypertension, leading to a null or weakened association among those 60 years of age or older. Accordingly, caution should be exercised when interpreting the results from later-onset participants.
Young adulthood is a neglected period of risk for excessive weight gain. Many adults with early-onset overweight, particularly those aged 18–39 years, feel healthy and have no medical problems that prompt a visit to a physician. Consequently, prevention of hypertension through control of adult weight gain, particularly among young adults between 18 and 39 years, must be emphasised.
Our study had several strengths, including the large sample size, availability of matched controls and repeated measurements of weight and height through adulthood. Furthermore, we confirmed cases of incident overweight that occurred during the follow-up period, which reduced the influence of the potential prevalence-incidence bias that is present when analysing prevalent cases.
Our study also had limitations. First, we cannot exclude the effects of residual confounding factors due to the observational nature of the study. Second, ascertainment of hypertension was based on a single measurement of blood pressure or use of antihypertensive medication in adulthood, which likely led to a wrong estimation of the incidence of hypertension. Third, recorded age at diagnosis was used as a surrogate for age at onset, which is vulnerable to inaccuracy because there is lag time between onset and diagnosis. More frequent assessments may contribute to a more accurate estimation of the ages of manifestation of overweight during follow-up. Fourth, we used BMI in adulthood as a proxy of overweight and additional studies are required using other measures of adiposity, such as waist circumference and body fat percentage. Fifth, the cut-off value of BMI 25–30 kg/m2 is not generally accepted for overweight diagnosis for East Asians, but we repeated our analysis using an alternative definition of overweight to compare our results. Sixth, the generalisability of our evaluations may be limited because the entire study population was derived from an occupational cohort. Finally, the sample size of women was limited for sex-stratified analyses.
Conclusions
In the present study, we found that younger age at onset of overweight was associated with a higher risk of hypertension and the risk increased gradually with each decade of attenuation of age at onset of overweight, peaking at 18–39 years of age. Considering the age at onset of overweight may contribute to risk stratification of hypertension of overweight adults in clinical practice. Greater focus on weight control may be warranted in individuals with early-onset overweight to prevent hypertension.
Key messages
What is already known on this subject?
Overweight is strongly associated with higher risk of developing hypertension.
Trends in overweight have shown an increase in prevalence along with younger age of onset.
However, the association between age at onset of overweight across adulthood and risk of hypertension remains unclear.
What might this study add?
Younger age at onset of overweight was significantly associated with higher risk of incident hypertension and the risk decreased with increase in age at onset of overweight.
How might this impact on clinical practice?
Assessment of age at onset of overweight may hold promise to improve risk stratification for developing hypertension.
Prevention or delay of onset of overweight in young adulthood may lower the subsequent risk of hypertension.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by the Ethics Committee at Kailuan General Hospital (reference number: 2006-5). Participants gave informed consent to participate in the study before taking part.
Acknowledgments
We thank the dedicated participants and all the investigators of Kailuan study for their support and contribution to this work.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors All authors contributed to the study design, acquisition or interpretation of data, and critical revision of the manuscript. All authors read and approved the final manuscript. SW and YC are guarantors. SW accepts full responsibility for the work and conduct of the study, has access to the data and controls the decision to publish.
Funding This study was supported by the National Natural Science Foundation of China (NSFC) (81870312).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.