Article Text

Abstract
Objective Among people with Marfan syndrome who have a typical aortic root aneurysm, dissection is a characteristic cause of premature death. To pre-empt Type A dissection, composite root replacement with a mechanical valve became the standard of care in the 1980s and 1990s. This is being superseded by valve-sparing aortic root replacement to avoid lifelong anticoagulation. In 2004, a total root and valve-sparing procedure, personalised external aortic support, was introduced. We report here results among the first 30 recipients.
Methods From cross-sectional digital images, the patient's own aorta is modelled by computer aided design and a replica is made in thermoplastic by rapid prototyping. On this, a personalised support of a macroporous polymer mesh is manufactured. The mesh is positioned around the aorta, closely applied from the aortoventricular junction to beyond the brachiocephalic artery. The operation is performed with a beating heart and usually without cardiopulmonary bypass.
Results Between 2004 and 2011, 30 patients, median age 28 years (IQR 20–44) had this operation and have been prospectively followed for 1.4–8.8 years by February 2013. During a total of 133 patient-years there were no deaths or cerebrovascular, aortic or valve-related events. These early outcomes are better than published results for the more radical extirpative root replacement operations.
Conclusions The aortic valve, the root architecture, and the blood/endothelia interface are conserved. The perioperative burden is less and there has been freedom from aortic and valvular events. A prospective comparative study is planned.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/
Statistics from Altmetric.com
Introduction
Standard surgical management of aortic root aneurysm in Marfan patients is either total root replacement (TRR) or valve-sparing root replacement (VSRR). Current ESC/EACTS guidelines for the management of valvular heart disease state that, whatever the severity of aortic regurgitation (AR), surgery should be considered in patients with Marfan syndrome, with risk factors (family history of dissection, size increase 2 mm/year in repeated examinations) who have aortic root disease with maximal ascending aortic diameter of ≥45 mm (Class IIa, Level C evidence).1
The placement of a personalised external aortic root support (PEARS), computer designed and manufactured to match the aortic root morphology of the individual patient, was introduced in 2004 as a conservative approach for Marfan patients. The device manufacture and operative method were the result of research and development between 2000 and 2004 when the first operation was performed.2 The computer aided design (CAD), manufacturing method and surgical technique have all remained consistent without the iterative development which has characterised the evolution of both TRR and VSRR.3 After proof of principle4 and prospective evaluation in the first 20 patients,5 ,6 the technique has undergone Health Technology Appraisal by the British National Institute for Health and Care Excellence (NICE).7
The purpose of this analysis is to describe the consecutive cohort of the first 30 patients to have undergone this procedure in two centres, the Royal Brompton Hospital, London, UK and the University of Leuven, Belgium, and who have had at least 1 year of follow-up. In this report, patient characteristics, procedural details and clinical outcomes to date will be presented. Survival and the incidence of aortic valve-related events are compared with a published meta-analysis of 1385 patients who received the current standard surgical treatments (TRR and VSRR)8 ,9 to discover whether outcomes following PEARS approach equivalence with those following the existing standard of care.
Methods
PEARS technology employs spatial data from MRI or CT images to create a CAD model from which a replica of the individual aorta is made by rapid prototyping (RP) (figure 1). On this former, a mesh support, customised for the individual patient, is manufactured from a macroporous textile knitted from a medical grade polymer yarn.4 The surgical method has been fully described.10 Briefly, the chest is opened through median sternotomy and the aorta is dissected proximally to the aorto ventricular junction, including creating space proximal to the coronary arteries for passage of the support. The mesh is removed from the former by opening the seam. The positions of the coronary ostia are indicated on the former and the mesh is incised to accommodate them (figure 2). The support is positioned around the aorta and the coronary arteries. The closing seam is secured.

Technical aspects of the support. The panels from left to right show the measurements made on the MRI and the model created from it by computer aided design. The next panel shows the former, a replica of the aorta in thermoplastic, made by rapid prototyping (commonly called 3-D printing29) and the soft macroporous mesh sleeve supported by it. The schematic shows the relationship of the support to the aortoventricular junction (below) and to the coronary and brachiocephalic arteries. Finally, the before and eight years after MRI scans showing complete conservation of the aortic root architecture and, therefore, the aortic valve support.

Surgical details of the opening made in the mesh for a coronary artery, the surgical dissection below the left coronary artery, and the mesh being passed below (proximal) to it.10
Patients diagnosed with Marfan syndrome and other aortopathies have routine interval aortic root measurements with echo and the general criteria for intervention are agreed.1 Criteria for first use of the procedure agreed with the Royal Brompton Hospital Research ethics committee were that patients should have little or no AR, and an ascending aortic root diameter of 40–45 mm.
Statistical methods
Standard descriptive statistical analyses were done with IBM SPSS V.20. Continuous variables are summarised as mean±SD, median±IQR, and range. Categorical data are presented as counts and proportions. Overall non-parametric survival estimates were obtained by the method of Kaplan and Meier. Linearised occurrence rates are calculated by dividing the number of events by accumulated patient years and expressed as % per patient year.
Comparison with existing standards
Meta-analytic analyses were done employing MS Excel 2007. Since patients in the PEARS dataset were operated upon electively to prevent further root dilatation, and may differ with regard to preoperative characteristics from patients undergoing TRR or VSRR, we performed additional weighted pooling of the baseline characteristics: patient age, preoperative root diameter, proportion of patients presenting with dissection, and the operative mortality in the Benedetto study.8 The weighted pooling was done employing inverse variance weighting, and in case of pooling of proportions, the natural log transformation was employed. In case of absent early mortality in a particular study, for the purpose of pooling the data, we assumed that operative mortality was 0.5%.
Results
Of 33 patients clinically evaluated, these 30 patients were offered PEARS surgery. We have not turned anyone down yet on grounds of anatomy, but there are two patients with measurements at 42 mm who have shown no enlargement over 18 months, but are having 6-monthly MRI measurement. One more has been affected by paroxysmal atrial fibrillation and whose aortic root has been 43 mm for last 3 years. These three patients are below root replacement criteria and remain candidates for PEARS.
Baseline
Table 1 displays patient and procedural characteristics. Of the 30 operations, 26 were performed at Royal Brompton Hospital (RBH) and four at Universitair Ziekenhuis Leuven, 23 by JP, four by FR and three by MP. The accrual rate was approximately linear and largely reflects the rate of Marfan patients presenting for surgery at RBH.
Patient and procedural characteristics
One patient had corrective surgery of a pectus excavatum at the time of the aortic root surgery.
Perioperative serious adverse events
One patient had recurrent ischaemia on several attempts to close the suture line in the external support. It was known that there was a small non-dominant right coronary artery which raised the suspicion of short left main coronary anatomy. The chest was closed and the patient recovered. Coronary angiography confirmed that suspicion, and with the imaging available, the support was safely positioned a few days later.
One patient had a ventricular fibrillation arrest in the intensive care unit. The emergency team released the closing suture and the heart rhythm became stable with restoration of a normal ECG. Subsequent imaging has shown the aortic dimensions to be stable. The situation remains under interval monitoring.
Follow-up
Average patient follow-up was 4.4 years, ranging from 1.4 to 8.8 years, with a total follow-up of 133 patient years. Follow-up was complete in 100% of patients until February 2013. During follow-up, no deaths occurred, and cumulative survival was 100% at 7 years. It should be recognized that at 7 years postoperative only five of the original 30 patients were still at risk.
There were no medical or surgical events related to the aorta or aortic valve. There have been no neurologic events.
Serious adverse events
During follow-up there was one patient who experienced exercise-induced constricting chest pain 6.7 years after the procedure (linearised occurrence rate 0.75%/patient year). Exercise ECG showed ischaemic ST depression. It was found to be unrelated to the aortic root pathology or surgery. Coronary angiography revealed the cause of angina to be an atherosclerotic left anterior descending coronary artery stenosis which was successfully stented. Aortography and coronary angiography performed at that time showed widely patent coronary orifices with no sign of impingement of the external support on the smooth lumen of his coronary arteries.11
Cross-sectional survey
Of the 30 patients, 29 were in New York Heart Association (NYHA) class I, and were either working or pursuing full-time study. The one other patient was in NYHA class III and unfit for work due to comorbidity predating surgery and unrelated to his aortic root disease. He has chronic obstructive pulmonary disease, pulmonary hypertension and multiple liver cysts which further impede breathing. At the time of the patient survey, 26 of the 30 patients were on some kind of medication, predominately as continued protective treatment for their Marfan aortic disease: 19 patients received β blocker medication, three patients received ACE inhibitor or AT II antagonist medication, two patients combined β blocker medication with an ACE inhibitor or angiotensin (AT) II antagonist. One patient was on antidepressant medication. The patient in NYHA class III was the only patient requiring anticoagulation therapy (warfarin); additionally, he was on diuretics and β blocker therapy.
Comparison with gold standard surgical results
Table 2 displays preoperative patient characteristics and postoperative and late outcome in the PEARS population (n=30) and in the TRR (n=972) and VSRR (n=413) patient groups from the Benedetto publication. Compared to the Benedetto TRR and VSRR patient groups, patients in the PEARS dataset were, on average, operated upon at a younger age with smaller aortic root diameters. None had dissection at the time of surgery or prior to it.
Comparison of PEARS with total root replacement (TRR) and valve-sparing root replacement (VSRR)
Discussion
Clinical follow-up data on the first 30 consecutive patients undergoing PEARS who have had at least 1 year of follow-up are presented. All patients in whom the intention was to perform this surgery are included. There were no perioperative deaths in this cohort of patients, 1–30.i There have been no aortic, valve-related or cerebral events among these patients. The 34th intended operation in December 2012, performed after the closure of analysis, was abandoned and the patient subsequently died. Details are provided below.
One limitation of the study is that magnitude and nature of the denominator population from which these patients were drawn cannot be reliably estimated, and the factors that influence the decision from one clinical team to another have not been documented.12 The Big Aortic Root Study (BARS) is being designed to capture this process for all patients with root aneurysm due to aortopathy.13
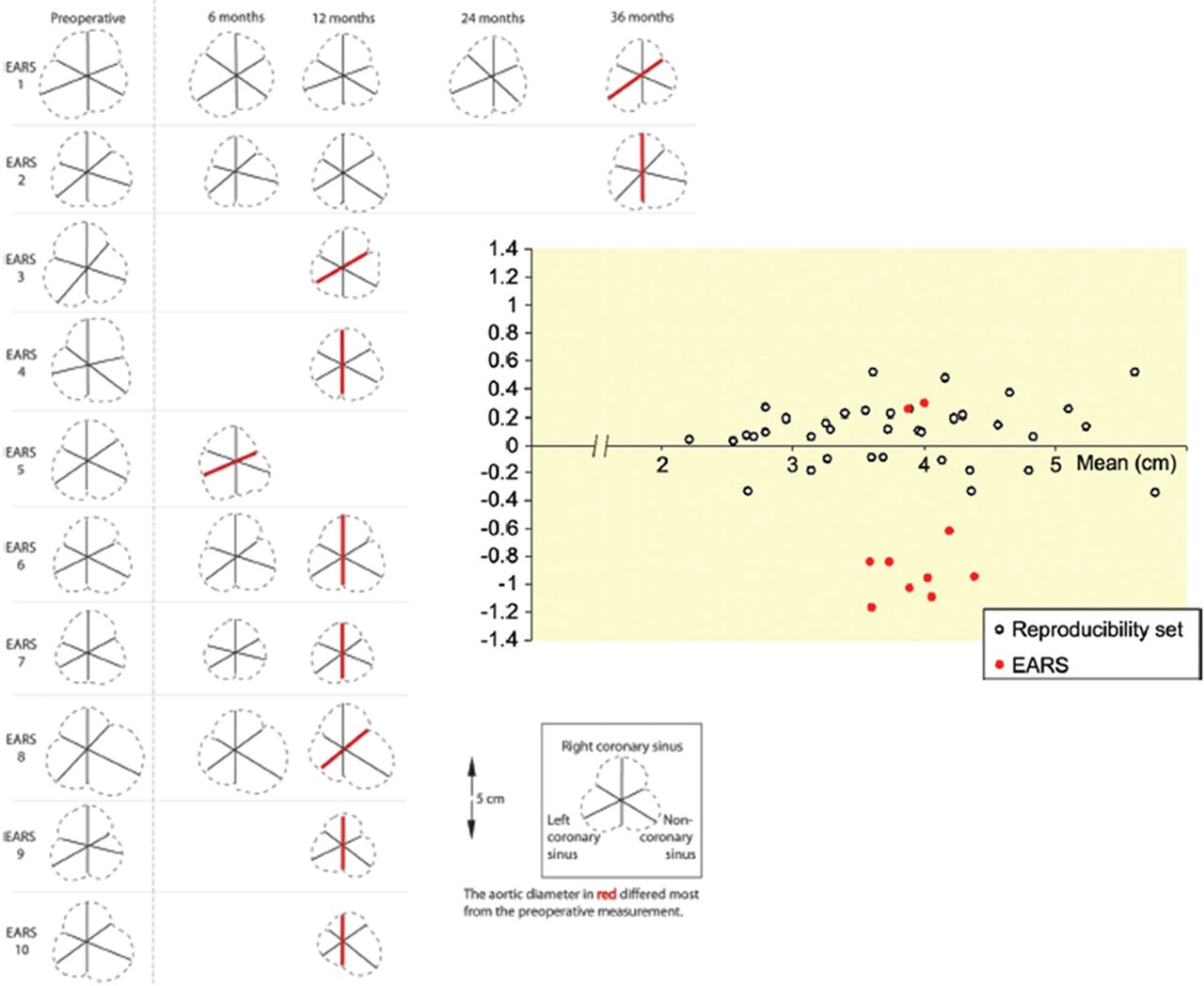
This is a small non-randomised study with a limited follow-up duration, so any conclusions concerning longer-term results are preliminary, and are made with caution, however, this is part of a stepwise prospective evaluation of PEARS. We have already established that the technical intentions of PEARS can be consistently achieved: measurement of multiple before and after images, made in random order without awareness of the identity of any image, showed that PEARS stabilises the size and shape of the aortic root and sinuses4 (figure 3). Analysis of periprocedural variables, compared with similar patients having root replacement surgery, confirmed that the anticipated advantages were achieved, cardiopulmonary bypass is not necessary, cardiac and circulatory arrest are completely avoided, and that blood product usage, operative time and hospital stay are commensurately reduced.6

All MRIs of the first 10 patients before (left), and at intervals after, with the diameter of greatest change shown in red. Duplicate measurements of 37 anonymised MRI images of Marfan aortic roots were presented with those of the patients in a random sequence.4 The black circles show the read-reread variation in the controls, and the largest difference in the patients in red. The variability in read-reread is amplified by choosing to display the one of three diameters with the largest difference, but illustrates the degree of imprecision that should be allowed for when clinical decision are being made. The reduction in size of eight out of ten supported aortas because the aorta is held at the size it was on the operating table illustrates the potential for restoration of aortic valve competence.
Meta-analysis of published results for root replacement showed that the composite risk of a valve-related event (thromboembolism, reintervention, endocarditis) among 972 patients who had TRR was 1.3% (95% CI 0.6 to 2.0), and for 413 who had VSRR it was 1.9 (95% CI 0.8 to 2.9).8 Of particular note is the reintervention rate of 1.3% for VSRR. More recent published results from an expert group continue to show this pattern of failure.14 None of these events have been seen yet in PEARS. (table 2) Varying clinical characteristics among the patient populations having TRR and VSRR, and a lack of intention-to-treat analyses limit the value of these comparisons8 ,9 which will only be resolved by direct comparison including random allocation of patients where equipoise for the surgical options becomes evident.15
There are several factors that limit the validity of this comparison. Patients with severe AR are more likely to have TRR and are not candidates for PEARS, so cannot be directly compared. PEARS is used at smaller size, and therefore, earlier in progression of the aortopathy, and this would create a lead time bias in favour of PEARS during long-term follow-up. Conversely, for patients who wait longer to meet the size criteria for a TRR with a mechanical valve, there is an immortal time bias: having surgery is conditional on having lived to reach the greater aortic root size. We believe that only by prospective data collection to protocol, as envisaged in the BARS study, will we be able to make corrections for these factors.
The intention of all three operations is most commonly to prevent aortic dissection. According to natural history data reported in 1972 for 257 people with Marfan syndrome, median survival was 40–41 years for men and 48–49 years for women. Among 72 patients who were dead at the time of life-table analysis, the average age at death was 32 years.16 As monitoring has become easier, operative risks have reduced, and awareness of the risk of dissection is heightened, root replacement has been advocated at smaller size. The criterion has come down from 60, through 55 and 50 mm 17–20 to the present recommendation of 45 mm.1 Earlier intervention introduces a new problem for patients and those advising them. It has always been possible that some patients having elective root replacement were never destined to have root dissection, and so, as the size criterion was lowered, there is likely to be an increasing number of patients who undergo surgery without gaining any years of life because their survival is determined by other factors. To illustrate the problem, we can consider carotid endarterectomy for which there are randomised controlled trials to evaluate the reduction in the risk of stroke. Using the ‘number needed to treat’ calculation, the number of patients who have an operation in order to prevent one stroke is six. These are patients with neurological symptoms, and a carotid stenosis greater than 70%, for whom the evidence for benefit is most compelling, yet five out of six patients having the operation gain no benefit from it. For clinical recommendations and comparative health economic evaluation, the number needed to treat to prevent a dissection in Marfan syndrome would be a useful statistic, not at present available. An attempt at decision analysis relied on best guesses from a handful of clinicians and, thus, failed for want of data.12 ,21
The most frequently voiced concerns when PEARS has been presented since its inception in 2004 are:
-
The support will migrate and impinge on a coronary artery.
-
A ‘wrapped’ aorta characteristically thins.
-
Aortic dissection may occur within the support.
-
The aorta will dilate beyond the support.
The first concern arises because of the misconception that PEARS is akin to wrapping of aneurysms, promulgated in the 1990s.22 Cut up portions of rigid low-porosity woven grafts were placed around the aorta in an ad hoc fashion, an application for which this material was never intended. There were instances of its hard edges causing erosion of vessels.23 The material used in PEARS is a soft, pliant, macroporous mesh which becomes intimately incorporated in the outer layers of the aorta.24 ,25 There is no potential for ‘migration’. This has been confirmed in controlled laboratory experiments in sheep26 (Figure 4).

Biological incorporation of the mesh. The left-hand panels are of placement of a sleeve of the mesh around the carotid artery of a sheep, and its appearance after five months. The macroscopic and histological appearances, with H&E and elastica stain are in the subsequent panels. The mesh is incorporated, the vascular architecture is preserved and the endothelium never interfered with.26
The second concern about aortic wall thinning is also an extrapolation from misuse of vascular graft material.27 Careful MRI monitoring reveals no sign of aortic wall thinning after PEARS.4 Studies in sheep to address this question show that the arterial wall thickens rather than thins26 (figure 4).
The strongest determinant of aortic dissection is the increasing size of the aorta,18 ,19 and this is halted by PEARS.26 Intimate apposition of the mesh can be achieved consistently (figure 5), and the histological appearances suggest that dissection is unlikely.26 Dissection in the supported aorta was not seen in a 20 year clinical experience (1984–2003) of external aortic support with a macroporous mesh.25 We contend that if dissection were to occur, its consequences might be lessened and more retrievable. However, no aortic root operation obviates all risks and it is the overall outcome that is the measure of effectiveness.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
A selection of the formers, which are replicas of the aortas of these patients indicating the variation in shape and size which can be successfully modelled with this technique.
Dilatation beyond the mesh (the fourth challenge) has not been observed to date. Just as with TRR and VSRR, PEARS itself cannot influence the course of Marfan syndrome or the likelihood of dilation or dissection beyond the limits of the support. The support in PEARS routinely extends beyond the brachiocephalic artery, and is thus more protective than the tube graft component of root replacement operations (figure 1). The transition in TRR and VSRR is at a sutured anastomosis to the remaining aorta, while with PEARS, there is a more gradual transition in hoop strength from the ascending aorta to the proximal arch. Any theoretical effect of dilation beyond the operated segment is, therefore, less likely with PEARS.
There were no perioperative deaths in the first 30 PEARS patients, who are the subject of this planned analysis. There was a subsequent postoperative death of the intended 34th patient in December 2012, 5 days after surgery. We present the details here for the purpose of full disclosure. The left main coronary artery was tortuous with an upward loop, not demonstrated on cross-sectional imaging. This was injured in the course of surgical dissection. Access was limited due to severe pectus excavatum, but exposure was considered adequate. The situation was rapidly retrieved with a suture but transoesophageal echo showed turbulent flow and loss of myocardial contractility. Cardiopulmonary bypass was rapidly instated and an internal mammary artery graft placed. The aorta was opened and the coronary orifice inspected. Excellent flow was confirmed in the native vessel and in the graft, but myocardial contractility did not recover as would be expected, and myocardial stunning was thought to be a factor. The external support was not positioned. Biventricular support was instituted, and after 3–4 days, there was good myocardial recovery, but 5 days after surgery, there was acute onset fixed dilatation of the pupils due to an intracerebral bleed. It should be noted that although current mortality with TRR and VSRR is considered to be low, in the meta-analysis for TRR the mortality was 4.1% (CL 1.9–7.7) and for VSRR 3.2% (CL 0.5–17.9). Furthermore, an unknown proportion of intended VSRR operations were aborted and converted to TRR or other operations, and thus, the results are unreported in the follow-up studies.
PEARS has been the subject of prospective step-wise evaluation, and has undergone formal technology appraisal by the NICE for use in the British National Health Service.7 This is in contrast with the iterative development of TRR and VSRR3 the introduction of which antedated the now more formalised approach to innovation and the introduction of new devices. Evidence to date suggests that PEARS may offer equivalent protection to root replacement with lower early and late risk. A direct comparative study is currently being planned.15 ,28 We propose a prospective comparative study of the three operations available for patients with aortic root aneurysms considered to be at risk of dissection or regurgitation. At present, advice given to patients tends to lead to the form of surgery preferred by the team. The intention of the BARS is to ensure evidence-based advice, uniform data acquisition and the possibility of random allocation when equipoise exists.
Key messages
What is already known about this subject
-
The commonest cause of death among people with Marfan syndrome is acute ascending aortic dissection most frequently seen in young adult life.
-
Current standard management is echocardiographic monitoring with a view to replacement of the ascending aorta, with or without aortic valve replacement.
-
A novel operation using computer aided design to make a personalised external aortic root support is now available, and has had NICE Health Technology Appraisal.
-
The surgery does not require opening the heart or aorta, or any interference with the cerebral or myocardial perfusion, and is usually performed without the need for cardiopulmonary bypass.
What this study adds
-
Clinical results up to 8.8 years for the first 30 consecutive patients are presented.
-
There have been no aortic, cerebral or aortic valve-related events at 133 patient-years of follow-up.
-
This compares favourably with results for valve-sparing root replacement which, on meta-analysis, was associated with 1.9%/year aortic valve-related events.
-
Root replacement with a mechanical valve is followed by a 0.7%/year thromboembolic event rate, a risk avoided with conservation of the patient's aortic valve.
References
Footnotes
-
Contributors TG proposed the concept of CAD modelled external aortic root support and developed it in collaboration with TT and JP; JP performed most of the surgery with other operations being performed by FR, MP and UR; RM and MR were responsible for cardiac imaging, WT developed the computer software and TG was responsible for device manufacture. JJMT, TT and BL collated the data, performed the analyses and prepared the data for publication. TT wrote the first draft and edited all subsequent versions. All authors have approved the manuscript.
-
Funding The Personalised External Aortic Root Support Project (PEARS) has been funded, to date, by Exstent Limited, a private limited liability company registered in the UK in July 2002. No external sponsorship has been involved. Further details can be found at (http://www.exstent.com).
-
Competing interests TG is a shareholder and director of Exstent Ltd, which holds the Intellectual Property in the Personalised External Aortic Root Support project. TG was the originator of the concept and the first recipient of the treatment. WT, as PhD student, worked on software development for CAD modelling (computer aided design), and continues to do this work for Exstent Ltd who manufacture the personalised supports.
-
Ethics approval Royal Brompton Hospital Research Ethics Committee.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement We are willing to share the full dataset on application to Dr Belinda Lees at the Clinical Trials and Evaluation of the Royal Brompton and Imperial College, London.
↵iThere was one late death after completion of this analysis. A patient operated on in December 2008 at the age of 26 with an aortic diameter of 42 mm was found dead in bed in May 2013. The aorta and valve were intact and the external support was closely applied and firmly adherent to the aorta. There was no evidence of dissection. The coronaries were free of disease and without evidence of thrombosis or any other abnormality. The forensic pathologist found no cause of death but presumed this was a sudden cardiac death in the context of Marfan syndrome.