Article Text

Abstract
Objective We aimed to describe current characteristics of patients admitted for acute coronary syndrome (ACS) in Western Europe and to analyse whether international in-hospital mortality variations are explained by differences in patients’ baseline characteristics and in clinical management.
Methods We studied a population-based longitudinal cohort conducted in Finland, France, Germany, Greece, Portugal and Spain, and comprising 12 231 consecutive ACS patients admitted in 53 hospitals between 2008 and 2010. Baseline characteristics, clinical management and inhospital outcomes were recorded. Contextual effect of country on death was analysed through multilevel analysis.
Results Of all patients included, 8221 (67.2%) had NSTEMI (non-ST-elevation myocardial infarction), and 4010 (32.8%) had STEMI (ST-elevation myocardial infarction). Inhospital mortality ranged from 15.1% to 4.9% for German and Spanish STEMI patients, and from 6.8% to 1.9% for Finnish and French NSTEMI patients (p<0.001 for both). These international variations were explained by differences in patients’ baseline characteristics (older patients more likely to have cardiogenic shock in Germany) and in clinical management, with differences in rates of thrombolysis (less performed in Germany) and primary percutaneous coronary intervention (high in Germany, low in Greece). A remaining contextual effect of country was identified after extensive adjustment.
Conclusions Inhospital mortality rates of STEMI and NSTEMI patients were two to three times higher in Finland, Germany and Portugal than in Greece and Spain, with intermediate values for France. Differences in baseline characteristics and clinical management partly explain differences in outcome. Our data also suggest an impact of the healthcare system organisation.
Statistics from Altmetric.com
Introduction
During the past three decades, studies have highlighted differences in acute coronary syndrome (ACS) morbidity and mortality between countries throughout the world.1 Differences were identified between industrialised and developing countries,2 but a north-to-south decreasing gradient of ACS morbidity and mortality was also identified within Western European countries.1 ,3 Outcome variation was mainly explained by differences in ACS severity,4 ,5 therapeutic management,6 ,7 and national socioeconomic characteristics.8 To reduce these variations, American and European cardiological associations have published international guidelines on ACS management strategies.9–12 Nevertheless, there is no recent international study reporting their effect on national differences in ACS morbidity and mortality.
We carried out a substudy in the EURHOBOP (European Hospital Benchmarking by Outcomes in ACS Processes) project. The objective was to determine whether the north-to-south mortality gradient was maintained in Western Europe. If international variations in mortality were found, we aimed to identify the determinants explaining these differences in risk of death. We especially examined the impact on mortality of ACS patients’ clinical profiles, management strategies and socioeconomic characteristics in the countries included.
Methods
The analysis was performed within the EURHOBOP study. EURHOBOP is a collaborative study aimed at benchmarking ACS management in Western European hospitals through inhospital mortality. It was conducted between 2008 and 2010 in seven countries (Finland, France, Greece, Germany, Italy, Portugal and Spain). In each country, 8–10 centres representative of the distribution of university, regional and private hospitals within the country's healthcare system were selected. Each institution included about 200 consecutive patients with discharge diagnosis of myocardial infarction (MI) or unstable angina (UA) (defined according to the International Classification of Diseases), treated in the last 3 years. This included ACS patients transferred from a primary care centre to a participating hospital.
Data collection
Demographic, risk factor management and severity characteristics were collected (see detailed description of variable collection and definitions at (http://www.eurhobop.eu/files/DL%202%20Protocols%20and%20forms%20preparation.pdf), pp. 22–38). The clinical diagnosis was obtained from the medical records, and case report forms were completed by a certified data extractor in each participating centre. To ensure quality of data collection, all investigators took part in collective training sessions. For each case, the investigators collected clinical, biological and electrocardiographic data from the medical records. Characteristics of each participant institution and invasive examinations performed during the same hospitalisation were also recorded. When necessary, multiple sources were cross-checked to ensure completeness of the information (review of discharge letters, computerised lists covering the hospital discharge diagnosis, laboratory computerised files and emergency department computer lists and death certificates).
The type of ACS was defined according to ECG findings at admission in agreement with current European guidelines; ACS patients with UA or unclassifiable ECG abnormalities were analysed as non-ST-elevation myocardial infarction (NSTEMI). LVEF was reported when available in medical records. As regards inhospital outcomes, acute pulmonary oedema, cardiogenic shock, reinfarction and death data were collected. Reinfarction was defined as recurrence of chest pain associated with suggestive ECG and re-elevation of troponins. Finally, to complete EURHOBOP data and to take into account the impact of socioeconomic inequalities between countries, we collected the gross domestic product and income Gini coefficient of each country in 2009.13 ,14
The income Gini coefficient is used to measure the inequality of income levels among a nation's residents. A Gini coefficient of zero expresses perfect equality, whereas a value of 1 expresses maximal inequality.
Statistical analysis
All analyses were performed using STATA V.11.2 (STATA, College Station, Texas, USA). ACS patients’ clinical profiles were summarised for each country as mean and SD for continuous variables and as a proportion for categorical variables. In the same way, the characteristics of the participating institutions, clinical practice and inhospital outcomes were evaluated in each country. One country was then removed from analysis because more than three baseline variables required for multivariate analyses were not available, and five hospitals were excluded because they reported unexplained low mortality rates under 1% for global and ST-elevation myocardial infarction (STEMI) mortality. Sensitivity analysis was performed to ensure these exclusions did not affect the reliability of our findings. Among the six remaining countries, missing data were either imputed by absence when clinically relevant (diabetes) or analysed through a ‘missing data’ class when required (hypertension, chronic renal failure, anterior ST-elevation, troponin elevation, LVEF). Analyses included these categories to avoid excluding patients, which could have biased the sample.
First, international differences in patients’ baseline characteristics, clinical management and inhospital outcomes were identified through bivariate analysis. Proportions were compared using the χ² test (or Fisher's exact test when necessary). Mean values of quantitative variables were compared by one-way analysis of variance (ANOVA) using Bartlett's test. When the basic assumptions of the Bartlett test were not met, a non-parametric Kruskal–Wallis test was performed.
Second, the impact of country on ACS mortality was assessed using three-level multivariate logistic regression. We performed a multilevel analysis to take into account potential common characteristics between patients (first level of the hierarchical system) treated in the same hospital (second level) and between hospitals in the same country (third level). Analysis was conducted following the method proposed by Snijders and Bosker15: contextual effects of hospital-level and country-level factors on outcomes were assessed by comparing each of the two-level null models (ie, not containing any independent variables) with the three-level null model (patients at the first level and non-patient factors at higher levels) using the log-likelihood ratio test. A contextual effect was retained for a p value <0.05. Thereafter, we developed nested three-level models successively incorporating patients’ baseline characteristics, reperfusion treatments, institutions and the socioeconomic characteristics of the countries in order to test whether the country effect remained significant despite exhaustive adjustment for individual and collective (hospital) factors. For all tests, p<0.05 was considered significant.
Results
The analyses were performed on the 12 231 ACS patients enrolled through the 53 private and public hospitals participating in the EURHOBOP study. The majority of patients (94.9%) were treated in a structure equipped with an intensive or coronary care unit, and 5416 (44.3%) were admitted to a university hospital. Most participating centres (54.7%) had a 24 h catheterisation laboratory (table 1).
Characteristics of admission hospitals in which ST-elevation myocardial infarction (STEMI) and non-ST-elevation myocardial infarction (NSTEMI) patients were admitted
ACS patients’ clinical profile in Western Europe in 2010
Thirty percent of patients were women (n=3725) and 32.8% (n=4010) of patients were admitted for STEMI. These STEMI patients were younger (age 64±14 vs 69±13 years, p<0.001) and more often current smokers (38.1% vs 22.8%, p<0.001) than NSTEMI patients. Conversely, NSTEMI patients more often had hypertension (65.5% vs 52.5%), diabetes (31.7% vs 22.7%, p<0.001) and a personal history of coronary heart disease (47.1% vs 20.4%, p<0.001) than STEMI patients. With regard to severity of illness, cardiogenic shock was more often recorded at admission in STEMI patients (6.5% vs 2.3%, p<0.001).
Variations between countries
As presented in table 2, differences in patients’ clinical profiles were recorded in the six countries participating in the analysis. ACS patients from Northern Europe (Finland and Germany) tended to be older and they more often had a history of coronary heart disease than patients from southern Europe. By contrast, Greek and French ACS patients were the youngest but were also more likely to be current smokers. The highest prevalence of diabetes was recorded in Spain and in Portugal. As regards clinical presentation on admission, reported rates of patients with STEMI were 37.7% in Spain, 35.3% in Greece, 34.7% in Finland, 31.6% in France, 24% in Portugal and 24.8% in Germany (p<0.001), and heart failure symptoms on admission were significantly less among patients from Portugal and Spain.
STEMI and NSTEMI patient baseline characteristics
Management of ACS patients in Western Europe in 2010
High rates of revascularisation were recorded among STEMI patients (table 3). Primary percutaneous coronary intervention (PCI) was performed in 2139 (53.3%) patients, and thrombolysis was administered in 836 (20.8%) patients. All in all, only 746 (18.6%) STEMI patients did not receive any revascularisation during their hospitalisation. Most NSTEMI patients (70.3%) also underwent invasive coronary assessment, but fewer (n=3712, 45.1%) required percutaneous or surgical revascularisation. Considerable variations between countries were observed in STEMI and NSTEMI management strategies (tables 2 and 3). Thrombolysis was rarely administered in Germany (2.6%), whereas a large proportion of STEMI patients (46.2%) were treated with thrombolysis in Greece. Moreover, thrombolysis was mainly provided before hospital admission in France (84.4%), Germany (53.8%) and Finland (52.4%), whereas, it was generally administered in hospitals in Greece (99.5%), Portugal (98.4%) and Spain (71.1%). The proportion of STEMI patients treated with primary PCI was 84.7% in Germany, 60.4% in France, 57.8% in Spain, 51.5% in Portugal, 41.3% in Finland and 18.4% in Greece (p<0.001). International variations in rates of percutaneous revascularisation were also recorded in NSTEMI patients, who were less often treated during the same hospital stay in Southern European countries: PCI was performed in 66.1% of patients in France, 57.4% of patients in Germany, 44.1% of patients in Finland, 37.3% of patients in Spain, 33.4% of patients in Portugal and 19.6% of patients in Greece (table 4).
ST-elevation myocardial infarction (STEMI) patients management and inhospital outcomes
Non-ST-elevation myocardial infarction (NSTEMI) patient management and inhospital outcomes
Socioeconomic data
In 2009, according to Eurostat publications, the gross national product per inhabitant in Purchasing Power Standards (PPS) and the income Gini coefficient were estimated at 116 PPS and 0.291 in Germany, 114 PPS and 0.259 in Finland, 107 PPS and 0.299 in France, 103 PPS and 0.323 in Spain, 94 PPS and 0.331 in Greece, 80 PPS and 0.354 in Portugal, respectively. After adjustment, these variables were not related to risk of inhospital death (table 5).
Multilevel multivariate analysis of factors associated with inhospital mortality in 58 hospitals treating acute coronary syndrome patients in six European countries
Inhospital outcomes of ACS patients in Western Europe in 2010
During the hospitalisation of STEMI patients, 262 (6.5%) presented with cardiogenic shock, 57 (1.4%) had reinfarction and 339 (8.4%) died. Event rates were slightly lower among NSTEMI patients: cardiogenic shock, reinfarction and death were recorded for 192 (2.3%), 94 (1.1%) and 362 (4.4%) patients, respectively. The incidence of inhospital events (cardiogenic shock, reinfarction and death) differed between the six countries (tables 3 and 4). For both types of ACS the highest rates of events were observed in Germany, Portugal and Finland, whereas Spain and Greece were associated with the lowest rates of inhospital events (table 5). International variability in the risk of death was confirmed by the multilevel model: the contextual effect of ‘country’ level was significant (p<0.001) in the ‘intercept only’ multilevel model, and in the complete multilevel model (p<0.001) after exhaustive adjustment for baseline, clinical and institution characteristics, and for national socioeconomic characteristics (table 5). The contextual impact of country on mortality in ACS patients is shown by residual analysis in figure 1. Despite high rates of revascularisation and exhaustive model adjustment, Germany and Portugal appeared associated with an increased risk of death, whereas risk was lower in Greece. In Finland, France and Spain, international variations were gradually attenuated by incremental adjustment (figure 1).
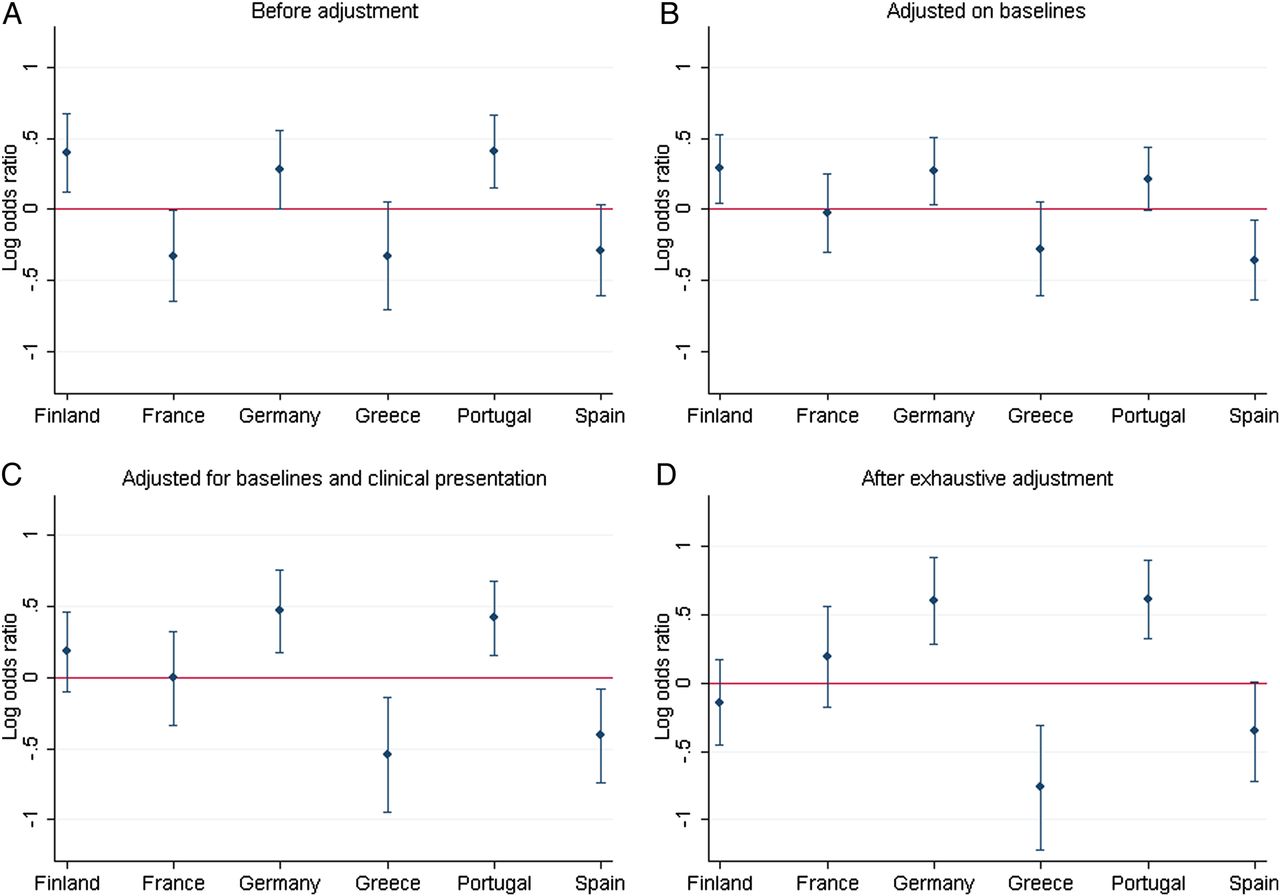
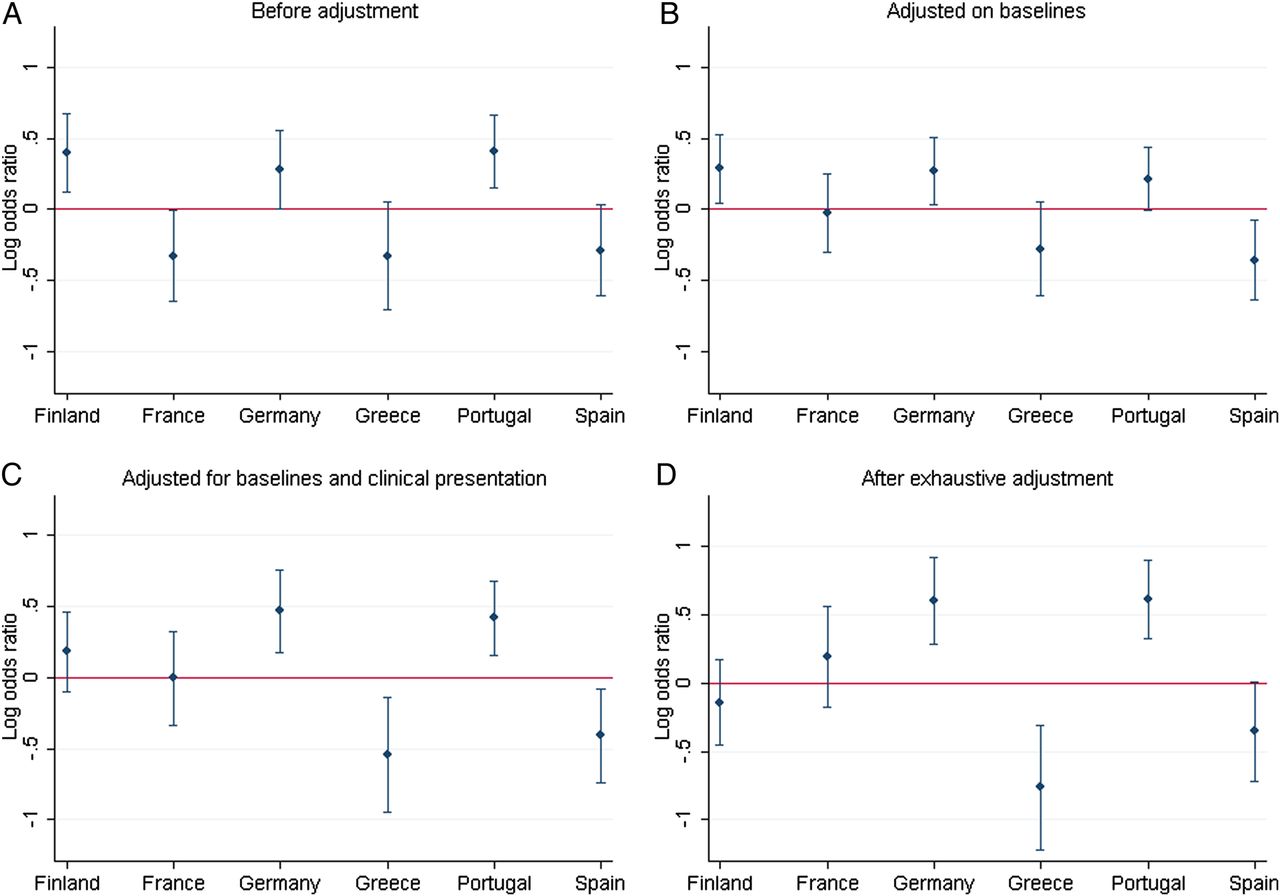{kind=link}
Logarithmic OR and 95% CIs for risk of inhospital death for each country according to multilevel analysis. (A) Without fixed-effect parameters. (B) After adjustment for baseline characteristics (age, gender, diabetes, hypertension, current smoking, obesity and history of coronary artery graft (CABG) surgery). (C) After adjustment for baseline and patients’ clinical presentation (STEMI or non-ST-elevation myocardial infarction (NSTEMI), left ventricular EF, heart failure symptoms on admission). (D) After exhaustive adjustment for (C), management strategy (PCI-revascularisation, type of institution) and socioeconomic characteristics.
Analyses stratified on STEMI and NSTEMI patients brought similar results regarding the link between country and mortality. Detailed results are available as web data supplement (see online supplementary tables S1 and S2). The heterogeneity hypothesis was confirmed using a two-level multivariate analysis considering country as a cofactor variable (see online supplementary table S3).
Discussion
The growing number of population-based, registries and of large cardiovascular clinical trials, has highlighted temporal and international differences in ACS epidemiology and outcomes.5 ,16 ,17 Our study revealed that large variations persisted in the outcomes of ACS patients in Western Europe. The inhospital mortality rates of STEMI and NSTEMI patients were two to three times higher in Finland, Germany and Portugal than in Greece and Spain, with intermediate values for France. We identified international differences in the baseline characteristics and in the clinical management of ACS patients that could partly explain the difference of risk, but unlike previous series, socioeconomic characteristics did not appear to be associated with differences in ACS mortality.8 ,18
Individual determinants of inhospital mortality
Our findings highlight that despite an evolution in ACS epidemiology over the past decade, major determinants of inhospital mortality are still age, diabetes and MI extension. PCI revascularisation appeared as the strongest predictor of improved prognosis in our results. An apparently protective effect of obesity was also identified. Similar findings have been previously reported and related to a decreased risk of haemorrhage associated with higher Body Mass Indexes and to particular neuro-hormonal impregnation.19 ,20 Smoking was also apparently associated with a better prognosis in our study, as it has been previously associated with more successful thrombolysis.21 However, we cannot exclude the possibility of a residual confounding effect, persisting despite adjustment, and due to age, gender or previous history of cardiac disease, which were all related to obesity and smoking.
In sensitivity analysis exploring the impact of missing data, OR for current smoking was equal to 0.69 (95% CI 0.51 to 0.92, p=0.013) when missing data were imputed by absence and 0.83 (95% CI 0.6 to 1.14, p=0.251) when they were not.
International differences in ACS epidemiology and prognosis
International differences in the clinical profile of ACS patients can be extracted from previous national cardiovascular registries (diabetes was recorded in 32% of German patients in 2000–2002, 23.7% of French patients in 2005 and 31% of Greek patients in 2007), but to the best of our knowledge, there is no recent standardised European study comparing risk factors among ACS patients according to geographic distribution.22–24 These differences between countries could be of interest to national cardiovascular societies. Such knowledge could help to define national priorities for cardiovascular prevention. For instance, our results highlight the need to strengthen campaigns against smoking in Greece, France and Spain, and they suggest that intensive efforts with regard to nutritional prevention programmes should be made in Spain, Portugal and Germany to reduce the prevalence of diabetes.
Our findings also point to differences between countries with regard to initial severity of illness. ACS were 30% more likely to be complicated by cardiogenic shock on admission in Germany than in Finland, Portugal or any other participating country. Similar findings have previously emerged from the MONICA registry. One of the proposed explanations was a recruitment bias due to an urban environment: patients living in towns and cities can reach hospital sooner, whereas isolated patients living in rural areas are less likely to reach hospital alive in the event of life-threatening symptoms.4 This hypothesis may explain why we recorded an excess of fatal outcomes in Germany while lower rates of inhospital deaths were recorded in Greece and Spain. Unfortunately, few recent data are available to evaluate prehospital ACS mortality and demonstration that the lower inhospital mortality recorded in Southern European countries is related to higher prehospital mortality is just based on a body of arguments: first, previous results from MONICA support the suggestion that the proportion of prehospital deaths tended to be lower in Germany than in Finland, France and Spain.25 More recently, MONICA registry reported that prehospital ACS fatalities represented 74.4% of 28-day ACS mortality in France in 2006 and 69.7% in Germany between 2009 and 2011 (personal communication from the MONICA/KORA registry).26 Second, taking into account that only 17% of Greek STEMI patients arrived at the hospital by ambulance27) and that broadly 50% of deaths related to ACS occur during the first few hours after symptom onset,26 we have to suspect higher prehospital ACS mortality in Greece than in Germany.
Confirmation of this assumption will require further international studies taking into account prehospital ACS mortality. Nevertheless, we know that the main limitation will be the quality of data collection concerning causes of death.
International differences in ACS clinical management
This European study confirmed recent improvements in STEMI revascularisation: primary reperfusion has risen from 56% in ACS-1 study to 74.1% in the present analysis with increased use of primary PCI, which nowadays appears to be the dominant revascularisation strategy in STEMI.17 ,27 ,28 However, we pointed out that large variations in ACS reperfusion strategies still persist in Western Europe.27 These concern STEMI and NSTEMI patients. In accordance with previous data, our results confirmed that use of PCI was less systematic among Southern European countries (which were less frequently equipped with a catherisation laboratory), but we also reported dramatic increases in rates of STEMI patients treated with primary PCI in Greece, Portugal and France.27 As regards thrombolysis, we showed that its delivery significantly differs between Northern European (Finland, France, Germany) and Southern European countries (Portugal, Greece, Spain), where thrombolysis was mainly administered upon arrival to hospital.
Finally, all these differences between countries are closely related to differences in the organisation of healthcare systems, which are likely to explain the remaining contextual effect of country on ACS mortality. This remains, however, a hypothesis that will have to be confirmed by other data. The possibility of a contextual effect suggests how difficult it might be to harmonise management of ACS patients over a large geographical area, and that a few more years will be required to overcome economical, geographical and epidemiological constraints.
Study characteristics and limitations
The strengths of the present study include a large number of ACS registered in a real-life setting according to a standardised protocol, which enables comparison between the six countries. The centres included are experienced in participating in such studies, and all investigators underwent collective training, guaranteeing the quality of the data. Moreover, for each country, preliminary analyses were performed to check that included data were consistent with published knowledge. The limitations of this study relate to our deliberate exclusion of Italian data for which many adjustment variables were missing and to the exclusion from the EURHOBOP protocol of all patients who died before admission to hospital. This restricts our conclusions to hospitalised ACS patients: our hypothesis that observed differences in inhospital mortality are related to differences in prehospital mortality is just based on the analysis of previously published studies confirming this.
Conclusion
There are still variations in ACS patients’ baseline characteristics and in their clinical management in Western Europe. These differences partly explain the international variations in ACS outcomes. Our findings also suggest that inhospital ACS mortality is highly impacted by differences in prehospital patient management that are directly related to healthcare system organisation.
Key messages
What is already known about this subject?
-
Previous population-based registries and large cardiovascular clinical trials highlighted temporal and international differences in acute coronary syndrome (ACS) epidemiology and outcomes. International guidelines have been published to harmonise clinical practice and reduce these variations.
What this study adds?
-
Despite recent improvements, there are still differences between countries in ACS patients’ presentations and in their clinical management. These lead to significant variations in ACS inhospital mortality, which was paradoxically higher in Northern European countries.
How might this impact on clinical practice?
-
These results highlight the heterogeneity in ACS management that persists between countries. Moreover, our findings reinforce the need to take prehospital mortality into account in further studies on healthcare system efficiency.
Acknowledgments
The authors gratefully acknowledge the collaboration of the hospitals and local researchers who participated in the EURHOBOP study.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
-
Contributors JM and JF supervised the acquisition of the data. RA, VB, JM, and JF wrote the paper. The other co-authors acquired the data and have critically checked the paper.
-
Funding This work was supported by a research grant from the French Federation of Cardiology (AR). The EURHOBOP study was supported by the Executive Agency for Health and Consumers (2008 13 12—EURHOBOP).
-
Competing interests None.
-
Ethics approval Each centre has obtained an ethics committee agreement in each country.
-
Provenance and peer review Not commissioned; externally peer reviewed.