Article Text

Statistics from Altmetric.com
In this issue of Heart there are several articles of particular interest to clinicians caring for patients with cardiovascular disease.
Bicuspid Aortic Valve Disease The association of bicuspid aortic valve disease with aortic dilation is now well recognised. However, it has been less clear whether all patients with a bicuspid aortic valve are at risk of progressive aortic dilation and adverse clinical events or whether we can identify a high risk subgroup. In a comparative study of aortic anatomy, Detaint and colleagues (See page 126) found a high prevalence of aortic dilation in adults with a bicuspid aortic valve. Although the average rate of aortic dilation was similar to Marfan syndrome patients, there was marked variability in the rate of progression with many patients with a bicuspid aortic valve having no evidence for progression aortic dilation.
In an accompanying editorial, Professor Della Corte (See page 96) points out that this phenotypic heterogenicity may allow us to stratify patients to focus followup and intervention on the subset of bicuspid valve patients most at risk of progressive aortic dilation or dissection. He also emphasises the need to describe morphologic pattern of leaflet fusion and the anatomic pattern of aortic dilation on imaging studies. He proposes that researchers should agree on a common terminology for precisely describing the bicuspid valve and aortic phenotype.
Risk Models for Heart Failure Based on a meta-analysis of seven studies with 1301 patients, Salah et al (See page 115) propose a risk model for patients discharged after an episode of heart failure that incorporates serum B-natriuretic peptide (BNP) levels in addition to several other clinical factors. This discharge risk score improves prediction of adverse events after hospital discharge.
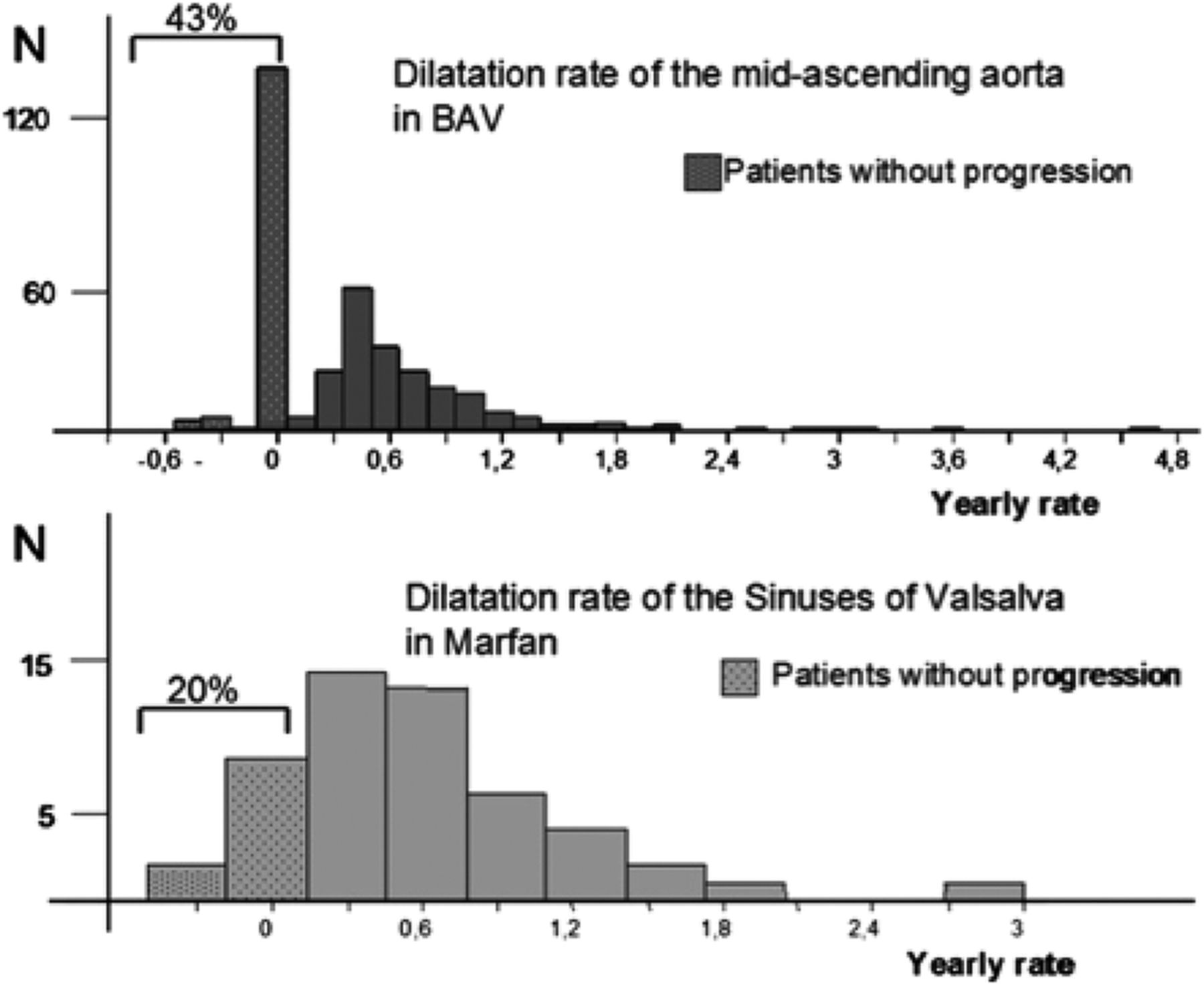
Comparative distribution of the aortic dilatation rate in the segment of the aorta more prone to dilatation. Tubular ascending aorta for patients with bicuspid aortic valve (BAV) and sinuses of Valsalva in patients with Marfan syndrome. Although the mean value is similar (0.42 and 0.49 mm/year respectively), the distribution of the population is very different.

Kaplan-Meier curves for the composite endpoint at 180 days according to ÉLAN-HF Score. Event rates increased significantly as the risk score increased. ÉLAN-HF, European Collaboration on Acute Decompensated Heart Failure.

{kind=link}
{kind=link}
{kind=link}
The number of page views that http://www.syntaxscore.com has received since its introduction. An early peak shortly after the release and the main results from the SYNTAX trial was seen, but since then the number of page views has continuously increased.
Heart Failure Guidelines The NICE guidelines for the use of ivabradine in patients with heart failure are summarised by Professor Suzanna Hardman (See page 93) in a detailed editorial. Recommendations now include rate dependent blockade of the the Na/K inward current, or ‘funny’ channel, by ivabradin, in addition to existing treatments, for selected heart failure patients. Implementation of this recommendation and clinical caveats are discussed.
Ivabradine in CHF NICE guidance
NICE recommends ivabradine as an option for treating patients with stable chronic heart failure who meet the following criteria:
-
Have NYHA class II–IV symptoms with systolic dysfunction
-
Are in sinus rhythm with a heart rate of 75 beats per minute or more after 5 min rest
-
Are already receiving standard therapy with β-blockers, ACE inhibitors and mineralocorticoid antagonists, or when β-blocker therapy is contraindicated or not tolerated
-
With an ejection fraction of 35% or less
Ivabradine should only be initiated under the following circumstances:
-
A stable period of 4 weeks on optimised therapy with ACE inhibitors, β-blockers and mineralocorticoid antagonists
-
By a heart failure specialist* with access to a multidisciplinary heart failure team. Dose titration and monitoring should be carried out by a heart failure specialist or by a general practitioner with special interest in heart failure or a heart failure specialist nurse
Education in Heart The article by Head and colleagues (See page 169) provides a clear understanding of how the SYNTAX score is calculated (http://www.syntaxscore.com). This angiographic score provides a quantitative measure of coronary artery disease severity that predicts death and major adverse cardiac or cerebrovascular events during a 5 year follow up. Interobserver variability in calculation of the SYNTAX score can be reduced by physician training. Clinicians need to be aware of the SYNTAX score because it is used in guidelines to define which patient should undergo percutaneous versus surgical revascularisation for coronary disease.
Footnotes
-
Competing interests None.
-
Provenance and peer review Commissioned; internally peer reviewed.
Linked Articles
- Valvular heart disease
- Editorial
- Heart failure
- Editorial
- Education in Heart