Article Text

Abstract
Objective Appropriateness criteria for stress echocardiography (SE) have been published to reduce the rate of inappropriate testing. We sought to investigate the clinical impact and prognostic value of these criteria.
Methods 250 consecutive patients undergoing SE for evaluation of coronary artery disease were classified into appropriate, uncertain and inappropriate categories according to appropriateness criteria. A positive SE was defined as the development of new wall motion abnormalities or a biphasic response. The primary end point was the composite of myocardial infarction and death.
Results Of the 250 SE, 120 (48%) were dobutamine studies and 130 (52%) were exercise studies. 156 (62.4%), 71 (28.4%) and 23 (9.2%) were classified as appropriate, inappropriate and uncertain, respectively. A significantly greater proportion of studies classified as appropriate 71 (45.5%) demonstrated inducible ischaemia compared with inappropriate studies 9 (12.7%) or uncertain studies 4 (17.4%), p<0.0001. During a median follow-up of 12.4 months, events occurred in 18 (11.5%), 2 (2.8%) and 0 patients classified as appropriate, inappropriate and uncertain, respectively. Event-free survival was significantly reduced in patients with a SE demonstrating ischaemia compared with patients without inducible ischaemia, p<0.0001. Kaplan–Meier curves demonstrated reduced event-free survival in patients with whose studies were classified as appropriate compared to inappropriate (p=0.01) or uncertain (p=0.05).
Conclusions Appropriateness criteria differentiate between patients at high risk of ischaemia, subsequent revascularisation/cardiac events (appropriate group) and those at low risk of events (inappropriate group). A large proportion of SE is currently performed in inappropriate patients. Implementation of the criteria in clinical practice would reduce unnecessary testing.
- Coronary Artery Disease
Statistics from Altmetric.com
Background
Stress echocardiography (SE) has emerged as an essential tool to evaluate patients with known or suspected coronary artery disease. The modality provides clinical referrers with diagnostic information identifying the presence and location of myocardial ischaemia, and is able to quantify myocardial viability.1 ,2 A wealth of prognostic data and the desire to avoid invasive investigations (with potential risk to the patient) has fuelled a growth in non-invasive diagnostic imaging.3 Appropriateness criteria have been published in an attempt to limit the use of non-invasive imaging to patients in whom stress testing is likely to provide most clinical benefit.4 These criteria grade the indications for SE into three categories as follows: appropriate, inappropriate or uncertain.
Early studies validating the appropriateness criteria confirmed that a large proportion of SE for evaluation of suspected coronary artery disease was performed for inappropriate reasons according to these criteria.5–7 Despite the publications of these criteria originally over 5 years ago, several investigators have found no real change in referral patterns or the number of inappropriate investigations ordered since their original publication in 2008.8 ,9
Data is sparse regarding the impact of implementation of the appropriateness criteria on subsequent clinical outcomes of patients. The purpose of this study was to investigate the clinical and prognostic value of appropriateness criteria in patients referred for either exercise or pharmacological SE for the investigation of known or suspected coronary artery disease.
Methods
Consecutive patients who underwent SE for evaluation of known or suspected coronary artery disease in the echocardiography laboratory at our institution between October 2010 and September 2011 were evaluated. Patients who underwent SE for concomitant significant valvular heart disease and cardiomyopathy were excluded. The study was approved by the institutional review board.
Ischaemia protocols
Patients either underwent treadmill or pharmacological SE at the discretion of the cardiologist performing the test.
For exercise SE, resting images were obtained of the parasternal long-axis, short-axis and apical four-chamber, two-chamber, and three-chamber views. A treadmill exercise test was performed using the Bruce protocol. The test was symptom-limited. Postexercise images were obtained within 60 s of termination of exercise.
For dobutamine SE, dobutamine was infused via a peripheral cannula starting at 10 mcg/kg/min. The dose was increased at 3 min intervals in 10 mcg/kg/min increments up to a maximum of 40 mcg/kg/min. If 85% of target heart rate was not achieved despite maximum dose of dobutamine, atropine was administered in 0.3 mg aliquots up to a maximum of 1.2 mg. The test end-points were the achievement of 85% of age-predicted maximum heart rate, or the development of new regional wall motion abnormalities. Images in the same views as for exercise SE were obtained at baseline and peak dose. For both methods, if >2 myocardial segments were poorly visualised, intravenous contrast agents were administered using a bolus injection of 0.3–0.4 mL at baseline and peak stress. The test was reported by a staff cardiologist and reviewed by an expert reader. Ischaemia was defined as the development of a new or worsening of existing wall motion abnormality or a biphasic response in segments with baseline wall motion abnormalities. Moderate or severe ischaemia was defined as ≥3/16 segments with stress-induced hypokinesis/akinesis. 10
Pretest and outcome data
Demographics, coronary risk factors, past medical history, medication, SE test indications and test results were prospectively collected at the time of SE. Follow-up and outcome data were derived from the hospital electronic patient records which document outpatient and inpatient encounters. The referring hospital was contacted if the patient was not followed-up at our centre. Follow-up time was calculated from the initial test date to either the date of a cardiac event or the date of last contact with the patient.
We classified indications for SE as appropriate, inappropriate or uncertain according to guidelines. Each patient was categorised by two independent reviewers of the data. In cases where the classification was not consistent between the two reviewers, a consensus between the two reviewers was obtained. The term dyspnoea on exertion was assumed to be an angina equivalent if the requesting physician wished to identify ischaemia as a cause of the symptom.
Statistics
Data were expressed as median and IQR, or number and percentage. The χ2 test was used to compare categorical variables. Continuous variables were compared using analysis of variance ANOVA. When the number of categorical variables was less than five, the Fisher Exact Test was used. The primary end-point was death or myocardial infarction. Univariate logistic regression was used to identify predictors of a positive stress echocardiogram. Multivariable Cox regression analysis was used to identify predictors of survival. The Kaplan–Meier method was used for event-free survival analysis. The log-rank test was used to compare differences between survival curves. All tests of significance were two-sided. A probability value (p) of <0.05 was considered statistically significant. Statistical analysis was performed using StatsDirect V.2.5.7 (StatsDirect, UK).
Results
A total of 250 consecutive patients undergoing SE for the assessment of coronary artery disease were included in the study. Treadmill exercise studies were performed in 120 (48%) patients, and dobutamine in the remaining 130 (52%). A total of 35 different physicians referred patients to our laboratory. The study population had a typical distribution of cardiovascular risk factors.
Overall, 156 (62.4%), 71 (28.4%) and 23 (9.2%) were classified as appropriate, inappropriate and uncertain referrals for SE, respectively. Of the 120 patients undergoing dobutamine SE, 80 (66.7%), 32 (26.7%) and 8 (6.7%) were classified as appropriate, inappropriate and uncertain, respectively. Of the 130 patients undergoing exercise SE, 76 (58.5%), 39 (30%) and 15 (11.5%) were classified as appropriate, inappropriate and uncertain, respectively.
A comparison of the baseline demographics of inappropriate, appropriate and uncertain referrals is given in table 1. Studies classified as appropriate had older patients, an increased prevalence of diabetes and lower LVEF with a tendency towards a higher prevalence of hypertension. Exact agreement between graders was obtained in 219 cases (87.6%). In 31 (12.4%) cases a consensus opinion was reached.
Prevalence of myocardial ischaemia
Overall, 84 (33.6%) patients demonstrated inducible ischaemia. A significantly greater proportion of studies classified as appropriate 71 (45.5%) demonstrated inducible ischaemia compared to inappropriate studies 9 (12.7%) or uncertain studies 4 (17.4%), p<0.0001. Five of the nine inappropriate studies with ischaemia were asymptomatic. Moderate or severe ischaemia was identified in 23 (32.3%) patients with ischaemia. All these patients were appropriate and none were inappropriate or uncertain (p=0.06).
Baseline demographics
Of the 120 patients undergoing dobutamine SE, a significantly greater proportion of studies classified as appropriate 34 (42.5%) demonstrated inducible ischaemia compared to inappropriate studies 4 (12.5%) or uncertain studies 2 (25%), p=0. 01. Of the 130 patients undergoing exercise SE, a significantly greater proportion of studies classified as appropriate 37 (48.7%) demonstrated inducible ischaemia compared to inappropriate studies 5 (12.8%) or uncertain studies 2 (13.3%), p=0.03.
Logistic regression analysis showed that an inappropriate indication for SE (OR 0.37 (CI 0.19 to 0.74) predicted a negative stress echocardiogram (table 2).
Predictors of a stress echocardiogram positive for ischaemia
Revascularisation
A total of 56 (22%) of the 250 patients underwent revascularisation following SE. Of these, 51 patients (91%) demonstrated myocardial ischaemia by SE. Of the five patients with no demonstrable ischaemia, two patients had undergone SE primarily for viability assessment, and the other three had known coronary artery disease. Of the 156 patients in the appropriate group, 52 (33.3%) patients underwent revascularisation compared with 2 out of 71 patients (2.8%) patients in the inappropriate group, and 2 out of 23 (8.7%) patients in the uncertain group, (p=0.02).
Of the 71 patients with appropriate studies and ischaemia, 47 (66.2%) patients underwent coronary revascularisation (8 patients underwent coronary artery bypass grafting (CABG) and 44 patients underwent percutaneous coronary intervention (PCI)) compared with 2 (22.2%) out of 9 patients with inappropriate studies and ischaemia. Of the four patients with uncertain studies and ischaemia, two (50%) underwent PCI.
Cardiac events
Overall events
Of a total of 250 patients, 20 cardiac events (13 deaths and seven myocardial infarctions) occurred during a median follow-up of 12.4 months (IQR 10.6–16.3 months). Predictors of cardiac events were a positive stress echocardiogram (HR 5.39, 95% CI 1.64 to 17.72) and LVEF (HR 0.95, 95% CI 0.91 to 0.98), table 3.
Predictors of survival
Effect of ischaemia
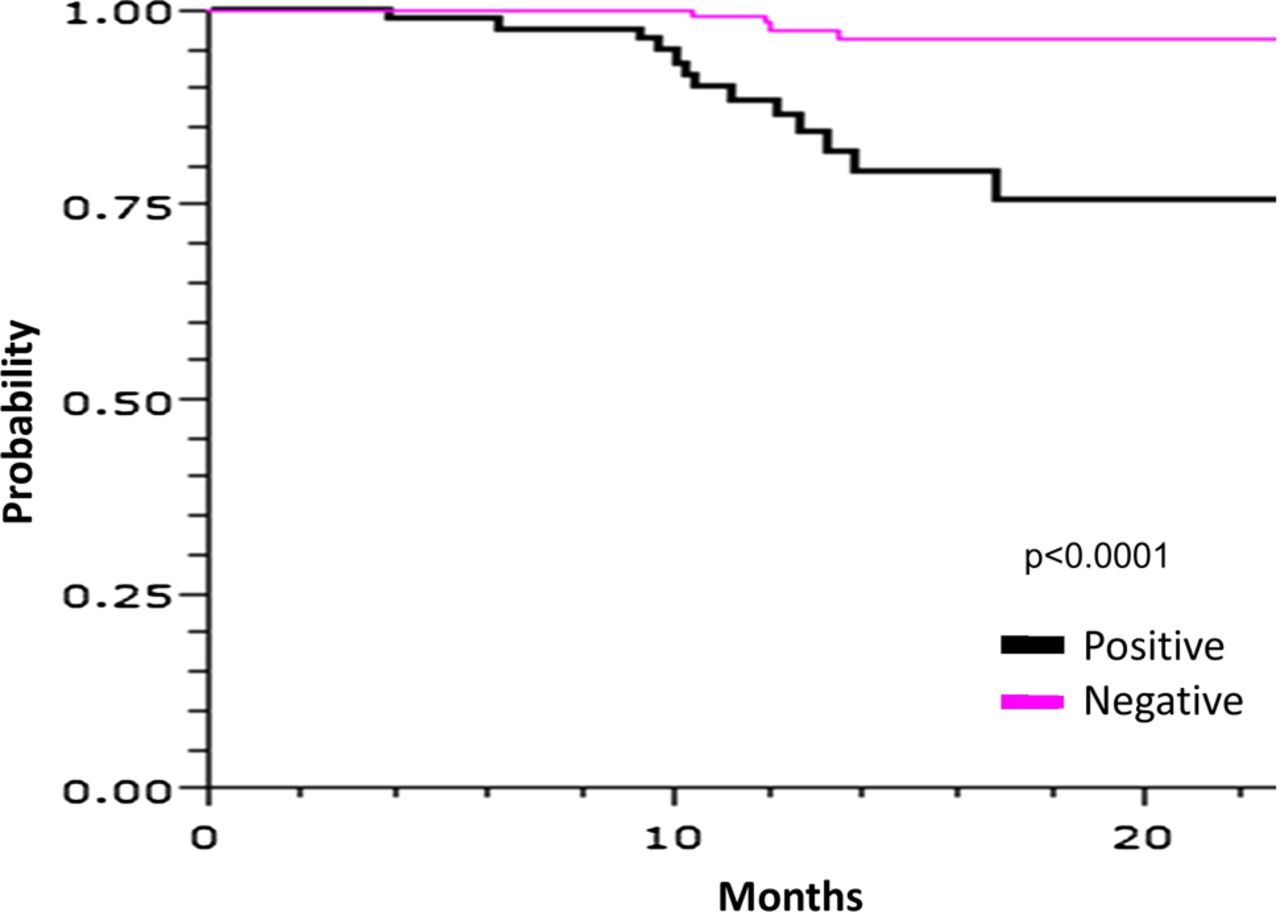
Cardiac events occurred in 15 out of the 84 (17.9%) patients with ischaemia, and 5 out of the 166 (3%) patients without ischaemia. Event-free survival was significantly reduced in patients with a stress echocardiogram demonstrating ischaemia compared to patients without inducible ischaemia, p<0.0001 (figure 1). When patients with significantly reduced LVEF (<50%) were excluded, cardiac events occurred in 14 out of 197 patients: 13 (16.5%) out of the 79 patients with ischaemia and 1 (0.9%) out of the 118 patients without ischaemia (p<0.0001). Cardiac events occurred in 5 out of the 23 (21.7%) patients with moderate or severe ischaemia compared to 10 out of 64 (15.6%) patients with mild ischaemia, p=0.52.

Kaplan–Meier survival curves comparing survival in patients with a stress echocardiogram demonstrating ischaemia to patients without inducible ischaemia.
Effect of appropriateness criteria
Cardiac events occurred in 18 (11.5%), 2 (2.8%) and 0 patients classified as appropriate, inappropriate and uncertain, respectively. In patients with dobutamine, SE cardiac events occurred in 8 (10%) appropriate and 2 (6.3%) inappropriate patients. In patients with exercise SE, all the cardiac events occurred in 10 (13.2%) appropriate patients only.
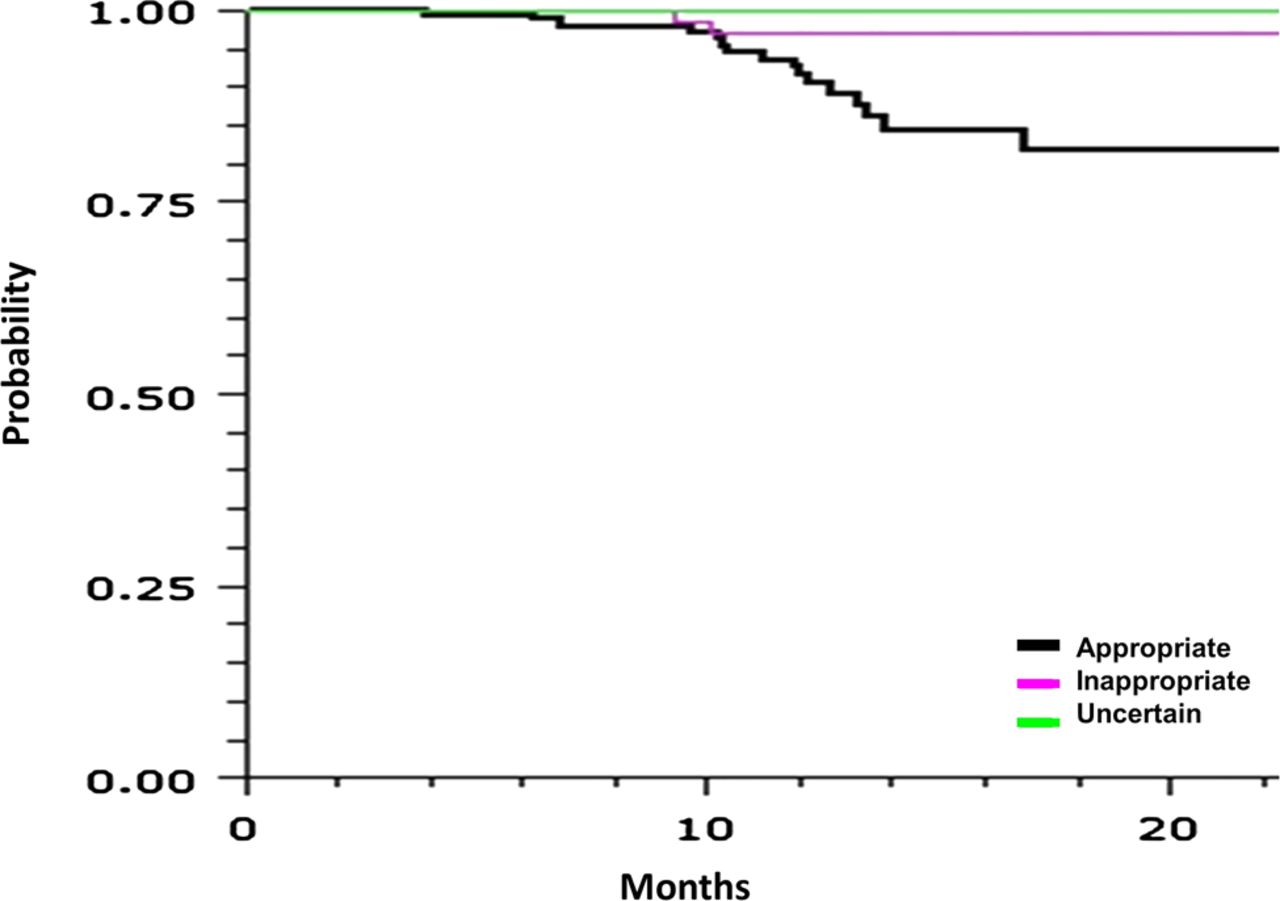
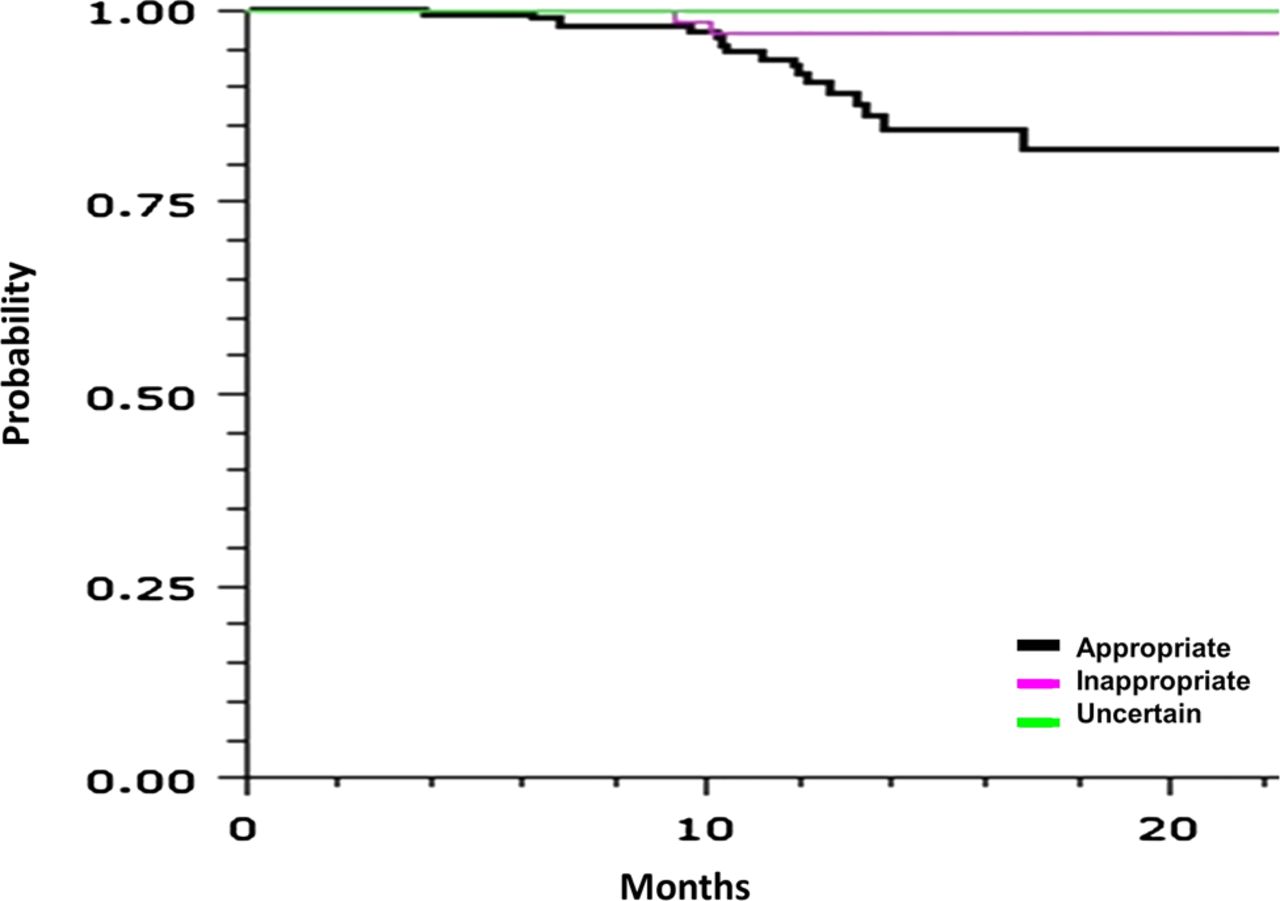
Of the 13 deaths, 12 occurred in (7.7%) appropriate studies and the remaining death occurred in 1 (1.4%) inappropriate study. In patients without LV dysfunction, cardiac events occurred in 14 (9.9%) patients classified as appropriate and no patients classified as inappropriate or uncertain. Kaplan–Meier curves (figure 2) demonstrated reduced event-free survival in patients whose studies were classified as appropriate compared with inappropriate (p=0.01) or uncertain (p=0.05). There was no difference in event-free survival between those classified as uncertain or inappropriate (p=0.48).
{kind=link}
{kind=link}
Kaplan–Meier survival curves comparing survival in patients whose indication for stress echocardiography was classified as appropriate, uncertain or inappropriate.
Predictive value of appropriateness criteria
The positive predictive values of an appropriate, inappropriate and uncertain test for a cardiac event were 11.5%, 2.8% and 0%, respectively. The negative predictive values of an appropriate, inappropriate and uncertain test for a cardiac event were 88.5%, 97.2% and 100%, respectively.
Discussion
This study has identified the clinical impact and prognostic value of applying the appropriateness criteria for SE to a patient population. In this study, a large proportion (almost a third) of currently requested stress echocardiograms was inappropriate according to the guidelines. These patients have a relatively low risk with an overall event rate in patients with inappropriate indications of less than 3%, specifically, mortality was 1.4%. The appropriateness guidelines were originally being published in 2008 with a refinement in 2011. 4 The aim of the criteria was to reduce unnecessary investigation. Several investigators have shown no change in the proportion of inappropriate studies over this time period.8 ,9 The reluctance to adopt these criteria into clinical algorithms may, in part, be due to concern about the lack of outcomes data among other variables. In order to implement the criteria and not perform testing in patients classified as inappropriate it would be important to show they have a relative low risk of cardiac events. Our study shows the mortality rate is low in patients classified as inappropriate.
Cortigiani et al7 identified that inappropriate studies were associated with a lower event rate than appropriate studies in patients undergoing dipyridamole or dobutamine SE. However, this study may have limited applicability to clinical practice in many countries. The American Society of Echocardiography recommend exercise SE as the first-line modality, reserving pharmacological methods only for those unable to exercise adequately.11 The technique has similar accuracy and outcome data to pharmacological SE but with the added information of exercise capacity which has prognostic value.12 In our study, we examined the prognostic value of these criteria incorporating pharmacological and exercise SE. For dobutamine and exercise studies, the prevalence of ischaemia and cardiac events was far higher in patients classified as appropriate compared to those classified as inappropriate or uncertain. Our event rate was higher than that reported by Cortigiani et al,7 and this is likely to be due to a higher prevalence of ischaemia in our cohort. Additionally, there is our cohort which had a significant proportion of patients with LV impairment.
Ideally, a cardiovascular imaging test should alter outcome and patient management. Our data showed that myocardial ischaemia was observed in almost half the appropriately referred patients (fivefold higher than the inappropriate group). Moreover, one-third of appropriately referred patients underwent revascularisation (approximately 10-fold higher than the inappropriate group) and the overall event rate in this group was around 12% (fourfold higher than the inappropriate group). Therefore, application of these criteria in routine clinical practice could reduce unnecessary testing which is currently being performed (inappropriate patients with a low risk of ischaemia, revascularisation and cardiac events), and concentrate testing on those patients where the result of the test is more likely to have an impact on patient management and outcome. The impact of this strategy on healthcare costs and downstream investigation is not known.
The overall cardiac event rate of patients deemed inappropriate was 3% but reduced to 0% in inappropriate patients with normal LVEF. The cardiac event rate in patients with a normal SE and normal LVEF was <1%. This is broadly in line with the cardiac events reported from a negative stress echocardiogram which are largely in patients with normal resting LV function.13 The majority of patients with inappropriate indications were for asymptomatic patients or patients with a low pretest probability/risk of coronary artery disease. However, a significant proportion of our patients (>20%) have low LVEF which is typical of a specialist hospital with predominant referrals from secondary care and, therefore, conferred a high risk even in patients with negative and inappropriate SE. The appropriateness criteria, while useful in guiding diagnostic testing, should be applied in the clinical context, taking account individual cardiovascular risk, such as LV function, in guiding optimal patient management.
The study also highlights the complexities in deciding the investigative pathway and management strategy in patients with coronary artery disease. SE has sensitivity for detection of significant coronary artery disease of between 70% and 90%.2 There will be a false negative rate of about 10%. Therefore, clinical judgment in addition to the result of the test is required to make informed management decisions. In this study, three patients with no ischaemia on SE underwent revascularisation. In patients with SE demonstrating inducible ischaemia, the options are to manage the patient with optimal medical therapy or perform revascularisation. In this study, about a third of patients were medically managed initially, and that is probably because these patients had a combination of mild ischaemia and higher associated risk of procedure which may have impacted on the final decision. Indeed, the COURGAE and BARI studies showed no difference in mortality between patients managed with optimal medical therapy and those who underwent revascularisation.14 ,15 However, long-term follow-up would be required to see if there is a crossover and subsequent revascularisation in the future.
The majority of inappropriate studies were performed in asymptomatic patients or patients with stable symptoms with prior revascularisation (CABG within 5 years or PCI within 2 years), perioperative risk assessment in patients undergoing low or intermediate risk surgery, or low-risk patients with stable symptoms and previous stress imaging less than 2 years ago. Physician education is now required to educate referrers about the indications for SE which are likely to alter patient management/changes in patient outcomes. Approximately a third of patients with appropriate tests demonstrated inducible ischaemia. Further research is required to see if refinement of the appropriateness criteria to target testing on patients where the test is likely to be positive, and thereby, focus testing on patients where it may change management.
Limitations
This study was observational with a relatively small size. The classification of studies into the three categories was based on available data. In some borderline cases it is possible that classification may have been different by other graders. The median follow-up was relatively short, and further studies with long-term follow-up would be warranted.
Conclusions
Implementation of the SE appropriateness criteria for evaluation of coronary artery disease would reduce the number of inappropriate investigations currently being undertaken and concentrate tests on patients where they are more likely to lead to change in management. The criteria differentiates between higher-risk patients who should undergo stress testing and lower-risk patients who may not require stress testing.
What is already known on this subject
-
There has been a growth in the use of cardiovascular imaging over the past decade. Appropriateness criteria have been published to limit the use of non-invasive imaging to patients in whom stress testing is likely to provide most clinical benefit, change patient management or outcome.
What this study adds
-
This study demonstrates that a large proportion of stress echocardiography investigations are classified as inappropriate. These patients have a low likelihood of a positive test and have a good prognosis. By contrast, patients whose indication for stress echocardiography is classified as appropriate have a high rate of positive tests, subsequent revascularisation and a poorer prognosis.
References
Footnotes
-
Contributors Each author substantially contributed to the research. SB, VK, RK and RS thought of the concept and designed the study. SB, VK, BS, NC, WL, IR, RK and RS performed the data collection, analysis and interpretation. SB, VK, RK and RS drafted and revised the manuscript. All authors read and approved the final version of the manuscript. RS has overall responsibility for the content and acts as guarantor.
-
Competing interests None.
-
Ethics approval Royal Brompton.
-
Provenance and peer review Not commissioned; externally peer reviewed.