Article Text

Abstract
This Almanac summarises important congenital heart disease articles published between 2012 and 2014 in Heart and other major cardiac journals. It highlights what the authors perceive to be highly relevant articles in the field. While the aim was to provide a comprehensive overview of the area, a focus on certain areas of interest was required. The selection is, therefore, by necessity a subjective one.
- review
Statistics from Altmetric.com
Epidemiology and foetal cardiology
The prevalence of congenital heart disease (CHD) at birth is estimated to be between 75 and 90 per 10 000 for live births and total pregnancies with subgroup analyses showing rates of termination of pregnancy up to 76% for foetuses with complex anatomy or univentricular hearts (table 1).1 A UK study also highlighted the significant variation in prenatal detection rates of CHD based on National Institute for Cardiovascular Outcome Research data and provided recommendations for how to improve screening performance and audit maternity data.2 ,3 Additional research is required to delineate prognosis and comorbidities, especially for relatively infrequent prenatal findings such as isolated right aortic arch, in order to improve parent counselling.4 The prevalence of CHD in adults is now estimated to be between 3 and 6.1 per 1000 based on data from the Quebec CHD database and on a systematic review of the literature, respectively.5 ,6 However, this is a dynamic population and an increase in the number of adult patients with CHD, with single ventricle physiology for example, by around 60% is predicted over the next decade. This is likely to require increased investment in human and physical capital so that patients with CHD reach their full life potential.7 ,8
Total and live birth prevalence of congenital heart defects: the EPICARD
The single ventricle
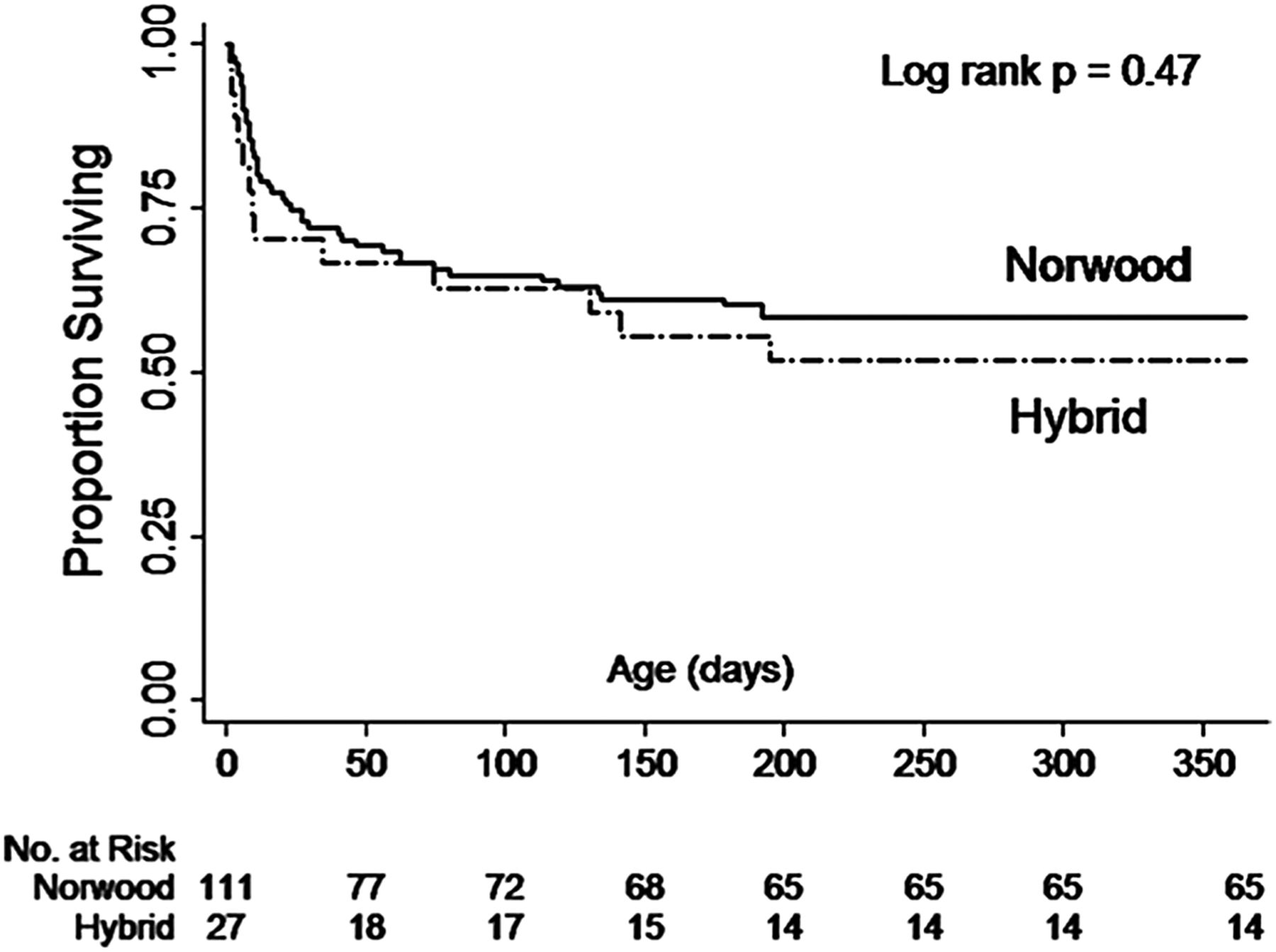
Currently, there are several approaches for palliation of patients with hypoplastic left heart syndrome and related RV anomalies. Surgical procedures include the ‘Hybrid approach’, Norwood and the Sano procedure, all of which serve to ultimately transition the patient to a complete Fontan anatomy.9 While it has been reported that the choice of palliation strategy may not affect mortality in this patient group,10–13 the optimal approach remains elusive with differences seen in specific subgroups. As an example, comparison of early and mid-term results of the ‘hybrid approach’ demonstrated no mortality difference despite significantly higher surgical (Aristotle) risk scores in the ‘hybrid group’ (see figure 1).14

Interstage survival after the Norwood and Hybrid procedures. Retrospective analysis of survival data from the UK. Kaplan-Meier curve demonstrates no difference in survival despite significantly different Aristotle’s scores between the two groups. Adapted from Lloyd et al.14
Advanced imaging modalities may eventually pave the way to optimising surgical strategies and improving long-term outcomes in these challenging patients. Cardiac MRI allows visualisation of the flow dynamics in patients with a total cavopulmonary connection.15 Power loss in the Fontan tunnel—which has been suspected to be the major determinant of reduced exercise capacity in Fontan—was significantly lower in patients with an intra-atrial lateral tunnel compared with extracardiac tunnels. Although power loss increased exponentially with increasing cardiac index during dobutamine stress testing, no correlation between power loss and exercise capacity on cardiopulmonary exercise testing was demonstrated.
Although the overall mortality after the Fontan operation has decreased substantially over the last decades,16 ,17 postoperative effusions, protein-losing enteropathy (PLE) and liver dysfunction remain significant challenges. In a retrospective study of 42 patients with PLE, current mortality was lower than in historic reports.18 Nevertheless, PLE remains difficult to treat and atrial arrhythmias occur in 67% of patients. This article may be of particular relevance to the clinician as it provides a detailed treatment plan for patients with PLE after the Fontan operation. Liver and renal dysfunction—common late complications of Fontan patients—may help to predict adverse late outcomes in Fontan patients.19 Consistent with expectations, increased Model for Endstage Live Disease - eXcluding INR (MELD-XI) scores—a tool to estimate renal and hepatic function—correlate with an increased risk of cardiac death or transplantation.20 Implementation of the MELD-XI score into clinical practice may be useful in predicting mid-term and long-term outcomes in this growing patient population.
Patients after the Fontan operation also have reduced skeletal muscle mass, associated with markedly impaired peak exercise capacity.21 Based on the finding of significantly decreased postexercise phosphocreatine resynthesis, the authors hypothesise the existence of a ‘Fontan myopathy’, which needs to be investigated in further detail. This finding is of particular relevance as the contribution of a competent muscle pump is essential to augment stroke volume and cardiac index during exercise in Fontan patients.22
Surgery
Supravalvular pulmonary stenosis (SVPS) is a major problem after the arterial switch operation for transposition of the great arteries (TGAs), with a prevalence as high as 55% in historic studies. Recently, mid-term results from 120 patients undergoing a modified version of the arterial switch operation—with a higher transection of the neopulmonic root and excision of the coronary ostia as limited ‘O’-shaped buttons—show a lower rate of SVPS beyond 5 years of follow-up. Freedom from reoperation for SVPS was 97.1% at 14.75 years.23 The authors attribute these outcomes to their technique that leaves the transected edge of the neopulmonic artery intact, but caution that future research is required to validate these findings.
Long-term follow-up data on >1700 adults after Ross procedure in the Netherlands and Germany demonstrated good durability of the pulmonary conduits with a rate of freedom from regurgitation grade ≥2+ of 95% after 14 years, and freedom from reintervention of 80% at 15 years follow-up.24
New data from the randomised Safe Paediatric Euglycemia After Cardiac Surgery trial demonstrated that patients >60 days of age benefited from tight postoperative glycaemic control with lower rate of infections, In contrast, younger patients showed an increased incidence of postoperative infections.25 Further trials are required to investigate the exact conditions under which tight glycaemic control may be advisable.
Two subjects of continuing discussion between surgeons and interventionalists are congenital aortic stenosis and ventricular septal defects.26 Recently, mid-term follow-up at a mean duration of 10±7 years after primary aortic stenosis treatment during the 1st year of life showed increased rate of reintervention in patients with balloon valvuloplasty (HR 4.0, p=0.001).27 In a prospective randomised controlled trial, 229 children with perimembranous ventricular septal defect were assigned to surgical or interventional defect closure. In this study, interventional closure was associated with less myocardial injury (lower Creatine Kinase -MB (CK-MB) and cTnI levels), shorter hospital stays, reduced medical costs and faster recovery times.28 The authors state that interventional closure appears to be the method of choice. However, at 2 years of follow-up there was no difference in closure rate, adverse events, and complications between groups and the issue of late atrioventricular block remains to be addressed.
Innovatively, postoperative support of families with videoconferencing has been demonstrated to be feasible and to reduce rehospitalisations of infants with CHD.29 Computerised techniques have also been shown to help surgeons monitor their risk-adjusted inhospital outcomes and compare it to over-regional benchmarks.30–32
Tetralogy of Fallot
In the last decades the operative treatment has dramatically improved with very low early mortality and morbidity. Therefore, the focus of attention is shifting to improving late outcomes of patients with Tetralogy of Fallot (ToF) from their third decade of life onwards. In a study from the UK, long-term outcome of patients with ToF was characterised with a duration of follow-up up to 45 years.33 The authors demonstrate that the annual probability of death remains fourfold higher than that of the general population throughout the first five decades of life. In a large multinational study (International Multicentre TOF Registry; INdiCaTOR), 873 adults with ToF were screened for risk factors that are predictive of death or sustained ventricular tachycardia.34 ,35 Based on cardiac MRI measurements, the authors identified RV and LVEF, RV mass index, RV mass-to-volume ratio and history of atrial arrhythmias as novel risk factors for late adverse outcome (see figure 2). Exercise capacity and LV function appear to be maintained in adult patients with ToF with increased RV end-diastolic volume index (>150 mL/m2)36 and are not useful to predicting the degree of RV dysfunction. Pulmonic valve regurgitation is one of the main causes of decreased RV function in patients with ToF, although it may be tolerated for decades in some individuals.37 A recent meta-analysis of outcomes after pulmonary valve replacement (PVR) including the data from more than 3100 patients, demonstrated that pooled 30-day mortality was 0.87% and 5-year mortality was 2.2%.38 The risk for re-PVR was estimated to be 4.9% after 5 years. Although publication biases are a major limitation of these findings, PVR appears to be a safe treatment option. Given this low risk, increasing numbers of asymptomatic patients now undergo PVR, although optimal timing remains uncertain.39
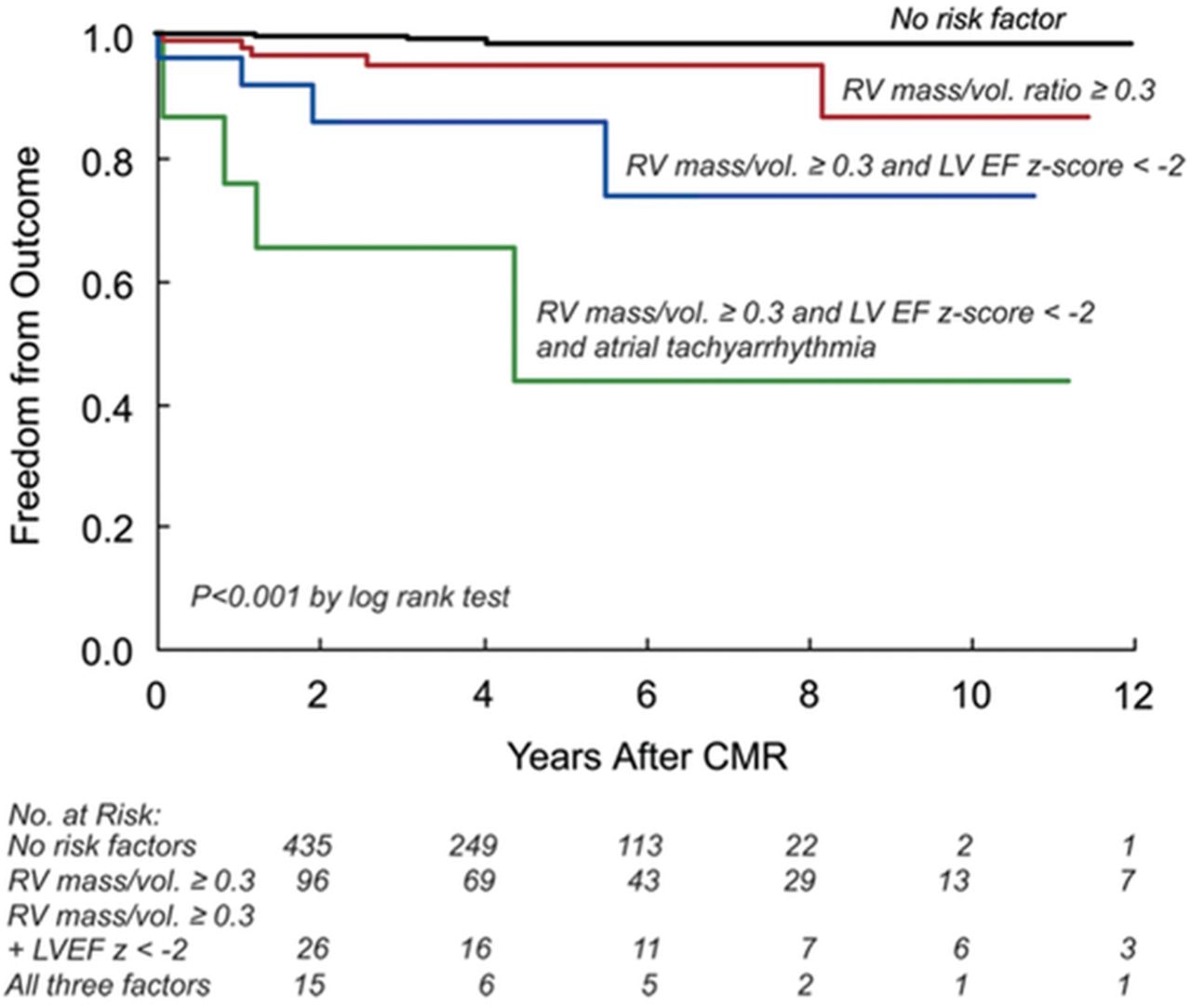
Predictors of death and sustained VT in patients with repaired tetralogy of Fallot (ToF). Data from the INDICATOR cohort demonstrate that RV mass/volume ratio ≥0.3, LVEF z-score <−2 and atrial tachyarrhythmias are most predictive of negative outcome in contemporary patients with repaired ToF. Adapted from Valente et al.34 CMR, Cardiac Magnetic Resonance Imaging; VT, Ventricular Tachycardia.
Research has also focused on delineating the role of the LV in determining long-term outcome in patients with ToF. In a sample of 413 adult patients with ToF, decreased LV function as assessed by transthoracic echocardiography correlated with a greater risk of sudden cardiac death or life-threatening ventricular arrhythmias.40 This finding was independent of QRS prolongation and appears to be an additional risk predictor for this patient population.
In a large multicentre study, echocardiographic screening of 474 adults with repaired ToF41 showed that only 6.6% of patients had an increased aortic diameter based on an observed-to-expected ratio >1.5. This relatively small proportion of patients is reassuring as previous estimates from smaller studies were much higher. Although it has previously been argued that immediate ToF repair in infancy may reduce the dilatation of the aortic root, no correlation between the duration of systemic-to-pulmonary shunt and the aortic diameter could be identified. Similarly, right aortic arch and aortic regurgitation were not predictive of increased aortic root diameter.
Transposition of the great arteries
Long-term follow-up data on 400 patients operated with atrial switch operation for D-Transposition of the Great Arteries (D-TGA) between 1983 and 1999 (median follow-up time 18.7 years) was recently published from a single North American centre.42 The investigators found that overall and arrhythmia-free survival at 25 years was around 97% in those patients that survived the immediate perioperative period. These results compare favourably with the much higher arrhythmia burden and incidence of sudden death previously reported in patients with atrial switch operation (Mustard, Senning). Freedom from any adverse events at 25 years was estimated to be 92.9%. At latest follow-up, LV function was excellent in most cases and 97% of patients presented in NYHA class I. The few deaths reported in this publication were presumably related to myocardial infarction or presumed arrhythmic aetiology.
Despite the beneficial effects of renin-angiotensin-inhibition for patients with LV dysfunction, previous small trials in patients with a systemic RV did not demonstrate a similar effect in this patient population. The lack of benefit of renin-angiotensin inhibition for a systemic RV is now corroborated by a larger multicentre, double-blind, parallel, randomised controlled trial involving 88 adults with transposition of TGA.43 In this study, no effects of valsartan 160 mg twice daily on RV EF or exercise capacity could be demonstrated at 3 years of follow-up.
In a prospective study, RV end-diastolic volume index >150 mL/m2 and peak systolic blood pressure below 180 mm Hg during exercise testing were associated with adverse cardiac events based on a combined end point including death, ventricular tachycardia, transient ischaemic attack, myocardial infarction, increase in NYHA functional class or hospitalisation for worsening symptoms of heart failure (HF).44 Patients with these characteristics had a 20-fold higher annual event rate. Classical parameters from ECG and transthoracic echocardiography were found to be less predictive and, thus, MRI and exercise test were recommended to be implemented as additional components of standard follow-up in these patients.
In a study of 91 consecutive patients that underwent Mustard operation before 1980 (median follow-up 35 years), cumulative survival was 80% after 20 years, 77% after 30 years and 68% after 39 years.45 Although exercise capacity remained relatively stable during the most recent 10 years of follow-up in this cohort, RV function decreases steadily while the prevalence of arrhythmias and HF increase significantly.
Pulmonary hypertension
In a large cohort of contemporary patients with Eisenmenger syndrome, echocardiographic parameters associated with mortality included46 indices of RV function (tricuspid annular plane systolic excursion, the ratio of RV effective systolic to diastolic duration) and right atrial area. Application of a novel score combining these predictors may help to risk stratify patients with Eisenmenger syndrome, particularly when assessment of functional class is otherwise difficult. In addition, brain-natriuretic peptide (BNP) levels have been shown to be related to outcome in this population.47 Observational data from a large adult CHD centre in the UK demonstrated that 6 min walking distance and baseline oxygen-saturations were strong predictors of death in 210 adult patients with Eisenmenger syndrome,48 while traditional markers of adverse outcome like functional class or peak exercise oxygen-saturations did not correlate with death. The authors state that patients who do not reach a 6 min walk distance ≥350 m or with baseline oxygen-saturations <85% have a threefold increased risk of mortality.
In the paediatric pulmonary arterial hypertension (PAH) population, sildenafil add-on therapy appears to be a viable option when bosentan monotherapy fails.49 Preliminary data on outcomes in paediatric patients with PAH from large multinational registries show that overall survival has significantly improved in comparison to historic samples, but there are discrepancies between the reports in reported survival rates of PAH related to CHD versus idiopathic/familial PAH.50 ,51 Further research will be necessary to investigate these differences with regard to survival, risk predictors and optimal treatment in further detail.
Arterial abnormalities in congenital heart disease
Research in the last decade has demonstrated that patients with repaired Coarctation of the Aorta (CoA) have a higher risk of mortality than the general population or patients with other forms of coronary artery disease (CAD),52 which has been attributed predominantly to an increased prevalence of CAD in this cohort. Now, in a large sample of adult patients with CoA from Canada (n=756), the diagnosis of CoA was not found to be an independent predictor for CAD development after adjustment for traditional CAD risk factors52 and this finding is supported by recent evidence of no clinically significant difference in endothelial function between adult patients with CoA and healthy controls.53
Adult congenital heart disease management
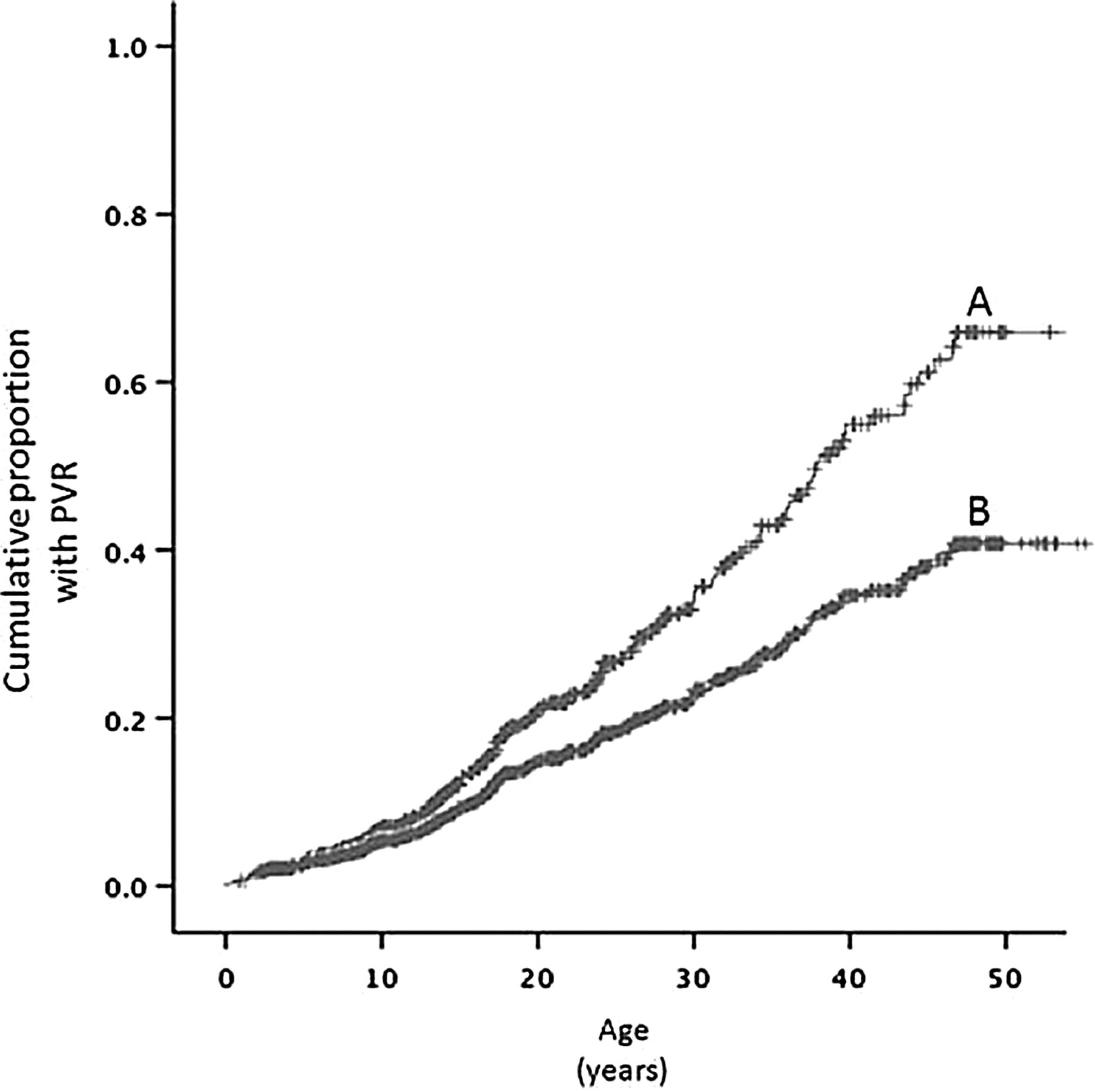
Along with the improvements in the care of CHD during the last decades, an increasing number of patients with CHD have the erroneous impression of being cured. This leads to a large number of patients lost to follow-up, which have an increased risk of developing adverse outcomes, including increased late mortality, compared with patients under specialised adult CHD (ACHD) follow-up (see figure 3).54 ,55
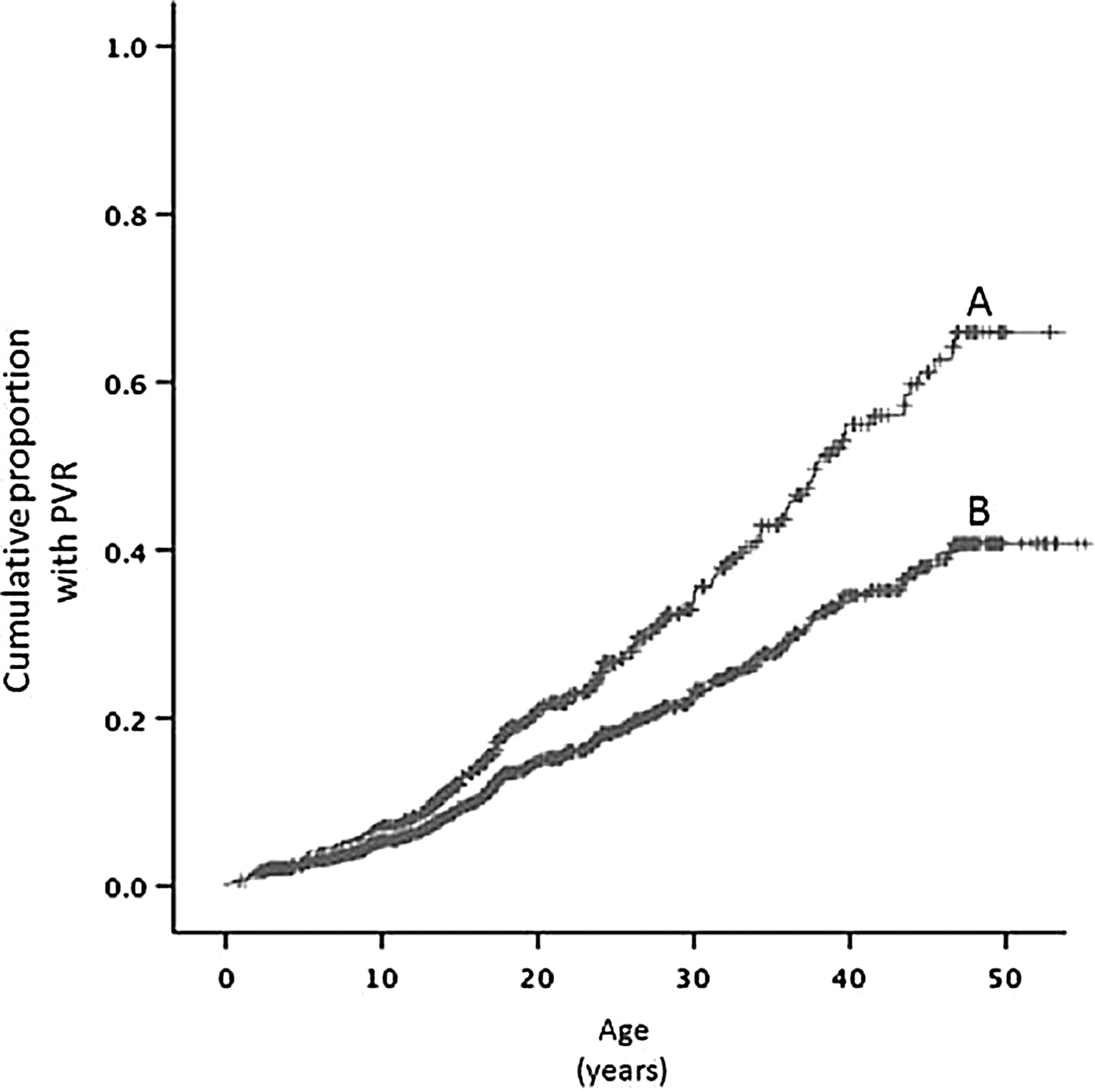
Prevalence of pulmonary valve replacement (PVR) stratified by quality of follow-up. Data from a UK cohort study demonstrates that the prevalence of PVRs in patients that are followed up under specialised care (A) is significantly higher than in patients without such care. Adapted from Wray et al.54
Identification of risk predictors for late adverse events in the growing population of patients with ACHD is one of the major goals in current CHD research. Recent studies show that moderate to severe impairment of lung function is an independent predictor of mortality, with an at least 1.6-fold increased risk of death compared with patients with normal lung function.56 In the same study, reduced peak oxygen uptake and heart rate reserve on cardiopulmonary exercise testing were additional predictors of mortality.57 A first set of reference values for the adult CHD population, stratified by CHD-subtype and gender, has recently been published.58 Also, patients with ACHD who are physically more active, tend to perform better on exercise testing.59 Twenty-four weeks of structured aerobic exercise training of adult patients with TGA significantly improves cardiopulmonary exercise testing parameters and reduces HF symptoms without a negative impact on the systemic RV.60 The benefits of a structured exercise programme combined with psychological training for improving overall activity in adolescents with CHD has also recently been demonstrated.61
In a study based on two large ACHD registries (including almost 40 000 patients between 1996 and 2005), 30-day inhospital mortality was lower in female than in male patients.62 Male gender, along with pacemaker implantation, was also highly predictive of 3-year mortality after admission for HF in the Dutch CONgenital CORvitia (CONCOR) registry.63 Intriguingly, women with a pregnancy history had the lowest overall mortality, which did not correlate with a higher utilisation of health services in this population.62
Survival data from a large cohort of elderly patients with ACHD (>60 years of age, n=375) during 5 years of follow-up at a tertiary ACHD centre demonstrated a significantly higher mortality compared with younger patients with ACHD or the normal population.64 Strongest prognostic predictors were the presence of CAD or congestive HF, NYHA class and systemic ventricular dysfunction. Healthcare providers should anticipate a substantial increase in the number of elderly patients with ACHD over the next few decades and be prepared to meet their special problems and needs.
Pregnancy and congenital heart disease
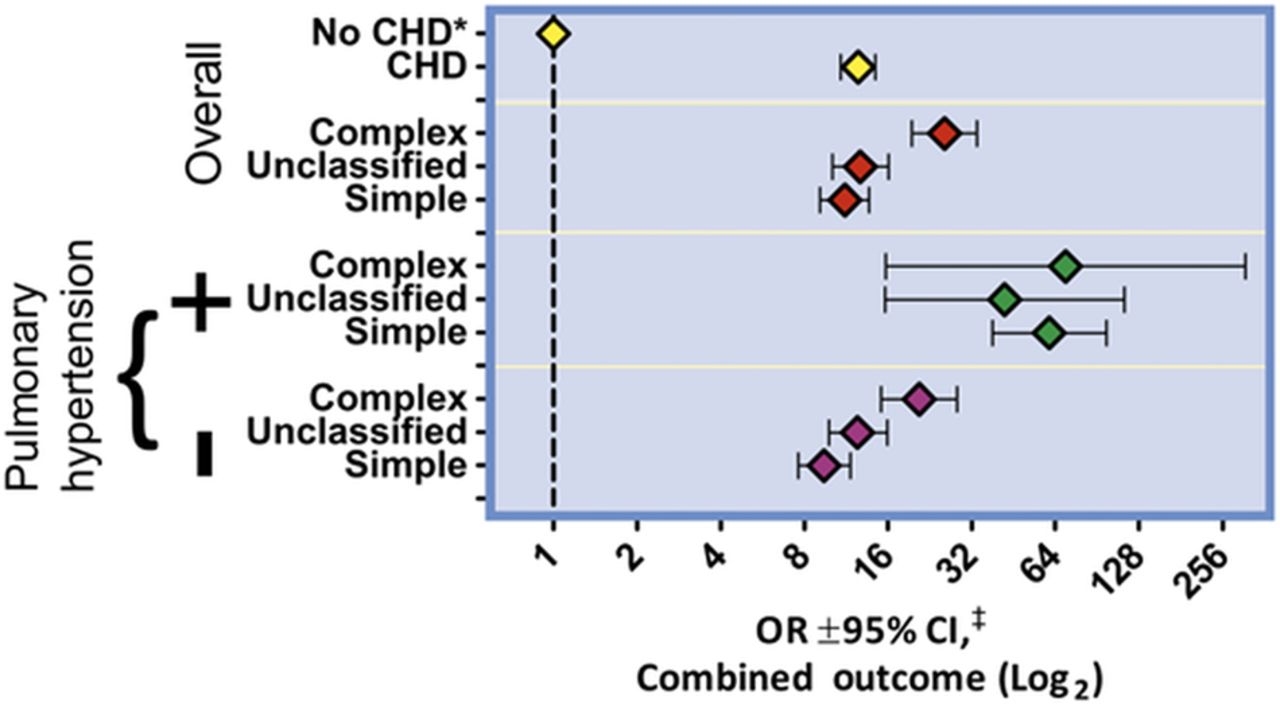
During the last 2 years, pregnancy-related outcomes in patients with CHD have been published from large trials or registries.65 Data from the Registry On Pregnancy And Cardiac disease demonstrated that HF is a common complication in pregnant patients with cardiac disease (13%, of more than 1300 participants).66 While the highest incidence of HF was found to be at the end of the second trimester or during childbirth, prevalence of HF was strongly associated with pre-eclampsia, premature birth and maternal and foetal mortality. However, patients with CHD had a relatively lower risk of developing HF compared with patients with valvular heart disease, ischaemic heart disease or cardiomyopathy. Nevertheless, the risk of cardiovascular events during pregnancy, particularly arrhythmias and death, is significantly elevated in patients with CHD (see figure 4),67 ,68 the rate of caesarean section is higher than background (13% vs 8%) and offspring are more likely to have low birth weight.67 Importantly, patients with complex CHD were found to have a higher risk of adverse cardiovascular outcomes than patients with simple CHD.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Adverse cardiovascular outcome during pregnancy, stratified by congenital heart disease (CHD) complexity and presence of pulmonary hypertension. Data from the largest US hospital discharge database demonstrates increased odds for adverse cardiovascular events (arrhythmias, cerebrovascular accidents, embolism, heart failure, death or a combined outcome) in patients with CHD compared with women who do not have CHD. OR±95% CI OR±95% CI on multivariate analysis; Adapted from Opotowsky et al.68
ZAHARA II, a prospective multicentre cohort study of more than 200 pregnant women with CHD demonstrated suboptimal uteroplacental Doppler blood flow patterns in comparison with controls.69 On multivariate analysis, preconception tricuspid annular plane systolic excursion (a measure of RV systolic function), high precursor of B-type natriuretic peptide cTnI - cardiac Troponin I (NT-pro-BNP), as well as mitral and tricuspid regurgitation were predictors of a decreased umbilical artery resistance index, which is known to be associated with adverse obstetric and offspring events. Affected women were more likely to develop pre-eclampsia and deliver small for gestational age babies (both fourfold increase). Based on these findings, preconception tricuspid annular plane systolic excursion as well as NT-pro-BNP may become helpful adjuncts in the risk assessment for women with CHD. The negative predictive value of a NT-pro-BNP <128 pg/mL at 20-week gestation was estimated to be 96.9%.70
Further details of current principles of care for pregnant patients with CHD with special sections on many CHD subtypes have recently been summarised in an excellent review article.71
Global burden of cardiovascular disease
Large efforts have been made to improve the outcome of patients with CHD or rheumatic heart disease (RHD) in the developing world and progress can be identified in several aspects as excellently reviewed for the African continent.72–74 In their review, Zühlke et al72 point out that establishing comprehensive prevention programmes as well as efficient screening for subclinical RHD has highest priority, as RHD remains to be the leading cause of cardiac disease in children of low-income countries. Along these lines, a new evidence-based guideline was published by the World Heart Federation in 2012 with the intention to standardise RHD criteria on the basis of 2D and Doppler echocardiography.75 These new guidelines have been found to be highly sensitive and specific in a prospective study of a high-risk population (Australian Indigenous population).76 The increasing availability of small and portable echocardiography scanners may further help to transfer these guidelines into clinical practice even in the most resource-constrained settings, as successfully demonstrated by a group from Uganda.77 Strategies like this should help to reduce the incidence of RHD related complications, including significant mitral stenosis and tricuspid regurgitation. A group from Korea demonstrated long-term follow-up data on patients after successful percutaneous mitral valvuloplasty for rheumatic mitral stenosis (299 patients for up to 12 years) and found that the incidence for developing tricuspid regurgitation increases even years after successful percutaneous mitral commissurotomy.78 If mitral valve replacement is performed for mitral stenosis, patients also benefit from concomitant tricuspid valve replacement if they have mild–moderate tricuspid regurgitation at the time of surgery.79
On the other hand, the diagnosis of CHD is also often delayed in low-income countries, which is associated with significant additional burden. Thus, earlier detection of CHD on a population-wide level is the most important criterion to reduce the lifelong burden of CHD in low-income countries. In a very large prospective trial involving more than 120 000 newborns in China, an example of successful implementation of pulse oximetry in low-income countries has been established,80 which helps to identify patients with major CHD that are not diagnosed on clinical investigation alone. Further advantages of this technique, as opposed to widespread implementation of echocardiography, are the low workload, the short screening time and the simplicity of its performance. In their study, the false negative rate for pulse oximetry was 0.3%, while without pulse oximetry, three times more babies with critical CHDs and two times more babies with other major CHDs would have left the hospital undiagnosed.
Images and case reports of congenital heart disease
Case reports and images constitute a significant proportion of publications on congenital heart defects. For the clinician, they provide an additional educational source and are especially important to illustrate innovative techniques in interventional paediatric cardiology37 ,81–85 and to raise the awareness for very rare congenital pathologies.86–88 In concert with educational articles on specific topics in CHD,89 ,90 they provide an excellent adjunct to keep all of us in paediatric cardiology curious and up-to-date.
References
Footnotes
-
Contributors PCK and G-PD carried out the literature review. PCK wrote the first draft of the manuscript, which was revised and approved by both authors.
-
Competing interests None.
-
Provenance and peer review Commissioned; internally peer reviewed.