Article Text

Abstract
Objective Late gadolinium enhancement (LGE) is not necessarily ideal for detecting diffuse myocardial fibrosis in idiopathic dilated cardiomyopathy (DCM). Since systolic blood pressure response (SBPR) during exercise has been proposed to reflect cardiac pump reserve in patients with heart failure, we wished to determine whether LGE plus SBPR is a better prognostic factor in patients with DCM.
Methods LGE and cardiopulmonary exercise testing results in consecutive 207 patients with DCM were examined. Patients were divided into four groups according to the presence or absence of LGE and the SBPR cut-off value of +40 mm Hg according to receiver operating characteristic curve analysis: LGE-positive+SBPR <40 mm Hg (n=65), LGE-positive+SBPR ≥40 mm Hg (n=40), LGE-negative+SBPR <40 mm Hg (n=33) and LGE-negative+SBPR ≥40 mm Hg (n=69). The composite end point was cardiac death, cardiac transplantation, LV assist device implantation, life-threatening arrhythmia or heart failure.
Results Forty-two (20%) patients developed the composite end point, with rates of 35%, 20%, 21% and 6% in patients with LGE-positive+SBPR <40 mm Hg, LGE-positive+SBPR ≥40 mm Hg, LGE-negative+SBPR <40 mm Hg and LGE-negative+SBPR ≥40 mm Hg status, respectively. Multivariable Cox regression analysis identified LGE-positive and SBPR <40 mm Hg as a significant independent predictor of cardiac events (HR 2.08, 95% CI 1.06 to 4.11, p=0.034). Of note, there was no significant difference in the cardiac event-free survival rate between the LGE-positive+SBPR ≥40 mm Hg and LGE-negative+SBPR <40 mm Hg groups (p=0.736).
Conclusions The combination of LGE and SBPR provides more clinically relevant information for assessing the risk of cardiac events in patients with DCM than LGE status alone.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Introduction
Late gadolinium enhancement (LGE) on cardiac magnetic resonance (CMR) has emerged as a first-line non-invasive modality for investigating the aetiology of myocardial dysfunction1 ,2 and evaluating cardiac prognosis in patients with ischaemic3 ,4 or non-ischaemic cardiomyopathy.5–7 However, since LGE relies on the difference in signal intensity between focal myocardial fibrosis and normal myocardium, it is limited in its ability to detect diffuse interstitial fibrosis, which is commonly found in idiopathic dilated cardiomyopathy (DCM).8 Thus, patients at high risk for cardiac events may have been missed in prior studies that investigated the presence of LGE alone.5–7
Peak oxygen uptake (peak VO2) or the regression slope relating minute ventilation to carbon dioxide output (VE/VCO2 slope) has been used to identify patients with either ischaemic or non-ischaemic cardiomyopathy at high risk for cardiac death or in need of cardiac transplantation.9 ,10 As a simpler and more convenient index, Williams et al11 and Kallistratos et al12 reported that peak systolic blood pressure (SBP) during exercise was associated with all-cause mortality and cardiac mortality in patients with chronic heart failure (HF). Blood pressure response (BPR) during exercise has been proposed as a marker of haemodynamic instability in patients with chronic HF.12–14 Based on these previous studies, systolic BPR (SBPR) during exercise testing may reflect cardiac pump performance reserve, which may correspond to the extent of diffuse interstitial myocardial fibrosis.
We hypothesised that the combination of LGE and SBPR may provide more precise information for risk stratification in patients with DCM than LGE alone. The aim of this study was to evaluate the predictive value of the combination of LGE and SBPR for cardiac outcomes in patients with DCM.
Methods
Study population
We conducted a prospective observational study of 207 consecutive patients with DCM at National Cerebral and Cardiovascular Center, Suita, Japan, between April 2005 and December 2012. The diagnosis of DCM was made based on WHO criteria.15 All patients underwent invasive coronary angiography to exclude significant coronary artery stenosis (>50% diameter stenosis). Myocarditis, hypertrophic cardiomyopathy, secondary cardiomyopathy, valvular heart disease and hypertensive heart disease were excluded. Symptom-limited maximal cardiopulmonary exercise testing (CPX) and CMR were performed while the patient was in a clinically stable, non-congested condition (New York Heart Association (NYHA) functional class ≤II). The median duration between hospital admission and CMR and CPX was 15 days and 25 days, respectively.
CMR protocol
CMR examinations were performed using a 1.5-T system (Magnetom Sonata, Siemens, Erlangen, Germany) with a four-channel surface coil. The procedures used to acquire MR images in this study have been previously described.16 We identified LGE using a segmented inversion-recovery prepared true fast imaging with steady state precession sequence with ECG triggering at 10 min after the administration of 0.15 mmol/kg body weight of gadolinium diethylenetriamine pentaacetic acid. LGE data was obtained during the mid-diastolic phase with an inversion time of 300 ms.16 ,17 Other imaging variables consisted of 65 segments, echo time 1.73 ms, flip angle 60°, field-of-view 340×255 mm, matrix 256×129 and voxel size 1.3×2.0×8.0 mm3. We also acquired cine imaging using a true fast imaging with steady state precession sequence (echo time 1.3 ms, repetition time 2.6 ms, flip angle 60°, slice thickness 8 mm, gaps 2 mm, inplane resolution 4.17×2.73 mm) over multiple breath holds in contiguous short-axis slices encompassing the entire LV and three standard long-axis slices.
LGE analysis
Two experienced radiologists who were blinded to clinical data and outcomes independently determined the presence and location of LGE. LGE was only considered present if it was visible in two orthogonal views. Figure 1 shows representative LGE-positive (A–C) and LGE-negative (D) cases. LGE pattern was characterised as mid-wall (figure 1A), diffuse (figure 1B) or focal (figure 1C). We categorised LGE-positive patients as having a mid-wall (n=52), diffuse (n=34) or focal LGE pattern (n=19), respectively. Interobserver and intraobserver agreement was evaluated for all study patients, and the κ values for interobserver and intraobserver agreement for the presence of LGE were 0.89 and 0.90, respectively. A third blinded reader adjudicated in cases with disagreement (n=10, 4.8%).

Representative examples of short-axis LGE-positive and LGE-negative images. A, B and C are short-axis images from LGE-positive patients. The typical LGE pattern in DCM is mid-wall enhancement in the interventricular septum (A). A diffuse pattern was observed in 34 out of 105 LGE-positive patients (B). Nineteen patients had focal enhancement (C, arrow). Figure 1D is a representative example of a LGE-negative case. DCM, dilated cardiomyopathy; LGE, late gadolinium enhancement.
For quantification of LV volumes and LVEF, we manually traced the LV endocardial contours in end-systolic and end-diastolic frames in cine imaging with a dedicated software program (Argus system, Siemens, Erlangen, Germany).
Exercise testing protocol
CPX was performed on a stationary cycle ergometer (AE-300, Minato; Tokyo, Japan). Blood pressure was measured every 60 s during exercise. SBPR was calculated as the difference in SBP between peak exercise and rest. During CPX, peak VO2 and VE/VCO2 slope were also measured.
Determination of BNP
Blood samples were collected in tubes containing EDTA, and plasma brain natriuretic peptide (BNP) was measured using a validated and commercially available immunoassay kit (Tosoh Co, Tokyo, Japan).
Follow-up and end points
After CMR data were obtained, study patients were followed at 3 months, 6 months, and 12 months and annually thereafter until the occurrence of one of the following cardiac events: cardiac death, cardiac transplantation, LV assist device implantation, appropriate implantable cardioverter-defibrillator discharge for ventricular tachycardia (VT) or ventricular fibrillation (Vf), and rehospitalisation for HF. Independent attending cardiologists blinded to the patient's LGE and SBPR status reviewed charts to determine if hospitalisations and deaths qualified as cardiac events. No patients were lost to follow-up.
Statistical analysis
All continuous variables are presented as means±SD and unpaired t tests were used to compare groups. Analysis of variance was used to compare means across multiple groups. Non-continuous and categorical variables are presented as frequencies or percentages and were compared using the χ2 test. If a four-group comparison was statistically significant, then post hoc pairwise comparisons between each pair were performed to demonstrate which pair was significantly different. The Tukey-Kramer test was used to compare continuous variables and the χ2 test with Bonferroni correction was used for categorical variables. Cumulative event-free survival curves were estimated using the Kaplan-Meier method and compared using the log-rank test. SBPR cut-off values were determined based on receiver operating characteristics (ROC) analysis. Univariable Cox proportional hazards regression models were used to calculate HRs for all cardiac events and 95% CIs. Multivariable Cox regression analysis was performed using covariates that significantly predicted all cardiac events in the univariable analysis, as well as established prognostic risk factors for chronic HF. Stepwise selection with a p value of 0.1 for backward elimination was used to select the best predictive model. All statistical tests were two-sided and p values <0.05 were regarded as statistically significant. Statistical analysis was performed with JMP, V.9.0.2 (SAS Institute, Cary, North Carolina, USA) and STATA, V.12 (StataCorp LP, College Station, Texas, USA).
Results
SBPR cut-off value for predicting the development of cardiac events
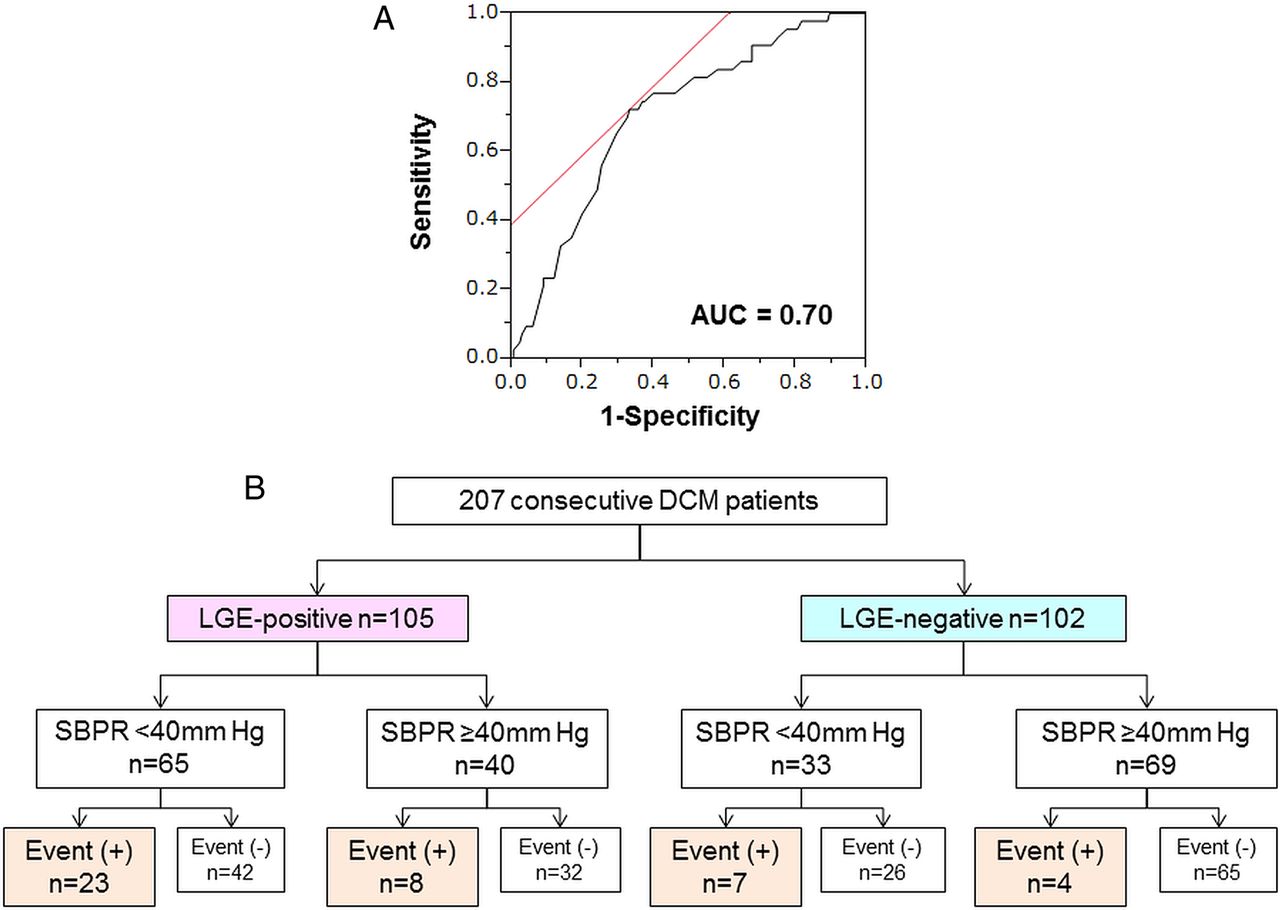
During a median follow-up of 44 months (IQR, 23–62 months), cardiac events were observed in 42 of 207 study patients. The median SBPR elevation for patients with or without cardiac events was significantly different, 32 mm Hg and 46 mm Hg, respectively (p<0.001). Based on ROC curve analysis, the optimal SBPR cut-off value for developing cardiac events was 40 mm Hg. The area under the ROC curve was 0.70 (figure 2A). At this value, the sensitivity and specificity for predicting a cardiac event were 72.1% and 66.8%, respectively. Based on this result, we divided the study patients into four groups according to the presence or absence of LGE and the SBPR cut-off value as follows: LGE-positive+SBPR <40 mm Hg (n=65), LGE-positive+SBPR ≥40 mm Hg (n=40), LGE-negative+SBPR <40 mm Hg (n=33) and LGE-negative+SBPR ≥40 mm Hg (n=69) (figure 2B). Of the 65 LGE-positive+SBPR <40 mm Hg patients, 23 (35%) experienced a cardiac event, whereas eight (20%) events occurred in the LGE-positive+SBPR ≥40 mm Hg group (n=40). On the other hand, 7 (21%) of the 33 LGE-negative+SBPR <40 mm Hg patients experienced a cardiac event. Only 4 (6%) of the 69 LGE-negative+SBPR ≥40 mm Hg patients experienced a cardiac event.

Receiver operating characteristics (ROC) curve analysis for the development of cardiac events and flow chart of study patients on the basis of LGE and SBPR. (A) ROC curve to determine the optimal cut-off value of SBPR for cardiac events. (B) Flow diagram illustrating the number of participants. DCM, dilated cardiomyopathy; LGE, late gadolinium enhancement; ROC, receiver operator characteristics; SBPR, systolic blood pressure response.
Baseline clinical characteristics and cardiac function
Table 1 shows the baseline clinical characteristics of the four groups. The LGE-negative+SBPR ≥40 mm Hg group was significantly younger than the other three groups (p=0.004). Interestingly, among the LGE-positive patients, those with SBPR <40 mm Hg had higher BNP levels and lower peak VO2 than those with SBPR ≥40 mm Hg (p<0.001), even though LV function and volumes were similar. Similarly, within the LGE-negative stratum, the SBPR <40 mm Hg group had higher BNP levels, reduced exercise tolerance, lower LVEF and larger LV volumes compared with the SBPR ≥40 mm Hg group (p<0.001). Importantly, there were no significant differences in BNP levels, exercise tolerance, and LV function and volumes between the LGE-positive+SBPR ≥40 mm Hg and LGE-negative+SBPR <40 mm Hg groups.
Characteristics of the study patients
Prognostic value of the combination of LGE and SBPR
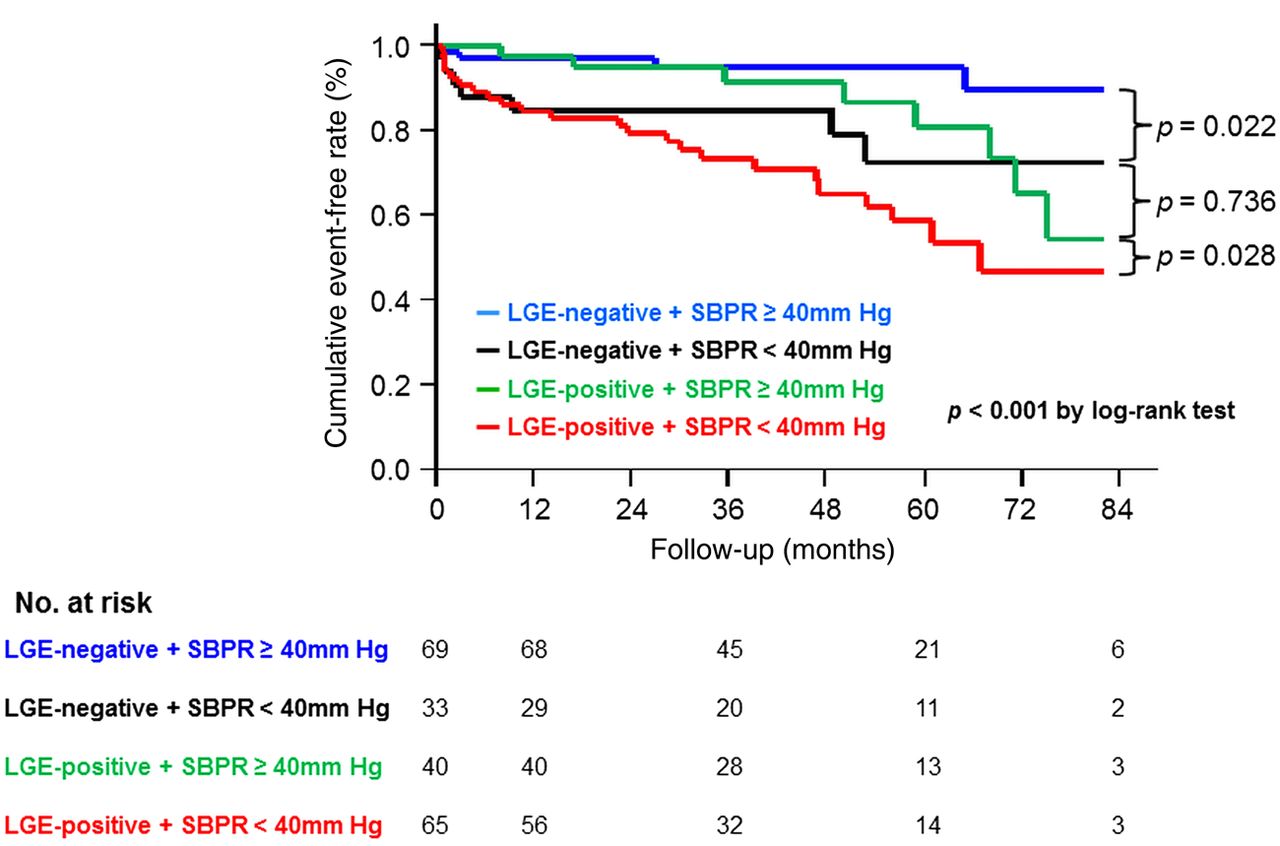
Of the 207 study patients, 27 (13.0%) developed HF, 7 (3.4%) received appropriate implantable cardioverter-defibrillator discharge for VT or Vf, 3 (1.4%) received a LV assist device and 1 (0.5%) underwent heart transplantation during the follow-up period (table 2). There were four cardiac deaths (1.9%); two patients each died of progressive end-stage HF and sudden cardiac death. Among the four groups, LGE-positive+SPBR <40 mm Hg status was associated with a higher rate of reaching the all cardiac events end point (p<0.001). Kaplan-Meier analysis showed that the cardiac event-free survival rate was lowest in the LGE-positive+SBPR <40 mm Hg group and highest in the LGE-negative+SBPR ≥40 mm Hg group (p<0.001 by the log-rank test). Importantly, the all cardiac event rate in the LGE-negative+SBPR <40 mm Hg group was intermediate, but comparable with the rate in the LGE-positive+SBPR ≥40 mm Hg group (p=0.736) (figure 3). Online supplementary figure S2 shows the Kaplan-Meier curves comparing the probability of all cardiac events according to the number of risk factors (LGE-positive status and SBPR <40 mm Hg) present when the two intermediate groups were merged.
Incidence of cardiac events during follow-up

{kind=link}
{kind=link}
{kind=link}
Kaplan-Meier curves comparing the probability of all cardiac events. The LGE-positive+SBPR <40 mm Hg group had the worst prognosis. Importantly, the all cardiac event rate in the LGE-negative+SBPR <40 mm Hg group was intermediate, but comparable with the rate in the LGE-positive+SBPR ≥40 mm Hg group (p=0.736). LGE, late gadolinium enhancement; SBPR, systolic blood pressure response.
Univariable analysis showed that a history of VT or Vf, BNP, serum creatine, QRS duration (per 10 ms increments), QTc interval (per 10 ms increments), heart rate and SBP at rest, SBPR <40 mm Hg, LVEF, LV volumes and presence of LGE were all significant predictors for all cardiac events (p<0.05) (table 3). When these factors were further analysed in a stepwise multivariable Cox model adjusted for factors that were significant in the univariable analysis as well as established risk factors (age, gender, NYHA functional class, peak VO2, VE/VCO2), a history of VT/Vf, LV end-diastolic volume index, presence of LGE and SBPR <40 mm Hg were significant independent predictors for all cardiac events (table 4, Model 1). When SBPR was considered as a continuous variable, it was still a significant predictor of cardiac risk in the univariable and multivariable analyses (see online supplementary table S2). To further investigate whether the combination of the presence of LGE and a SBPR cut-off value of 40 mm Hg is a better cardiac prognostic factor, we performed an alternative multivariable Cox regression analysis (table 4, Model 2). When this combination was used, LGE-positive+SBPR <40 mm Hg was significantly associated with cardiac events (HR 4.05, 95% CI 1.41 to 14.55, p=0.008). Since the number of cardiac events was relatively low in our study population, we demonstrated that the best predictive model adjusted for significant predictors selected in a stepwise Cox regression analysis based on Models 1 and 2. As a result, LGE-positive+SBPR <40 mm Hg (HR 2.08, 95% CI 1.06 to 4.11, p=0.034) remained a significant indicator of future cardiac events (table 4, Model 3).
Univariable Cox regression analysis of risk factors for all cardiac events
Multivariable Cox regression analysis of risk factors for all cardiac events
Discussion
The major finding of this study is that the combination of LGE status and SBPR during exercise is a significant and independent predictor of future cardiac events in patients with DCM. To the best of our knowledge, this is the first clinical study that demonstrates that a combination of structural (LGE) and simple physiological (SBPR on exercise testing) indices is a relevant prognostic marker of cardiac outcomes compared with either the presence of LGE or SBPR alone.
The prognostic impact of the combination of LGE and SBPR in patients with DCM
Myocardial fibrosis is associated with worsening ventricular systolic function, progressive remodelling and increased ventricular stiffness in patients with DCM.18 Recently, Gulati et al19 suggested that mid-wall LGE was independently associated with cardiovascular mortality and cardiac transplantation in the largest cohort of patients with DCM to date. Although many previous studies have suggested the prognostic value of LGE in patients with DCM, Schalla et al20 reported that the presence of fibrosis detected by LGE was not correlated with the amount of interstitial fibrosis detected on endomyocardial biopsy. Therefore, LGE status alone may be an insufficient prognostic indicator in patients with DCM.
To avoid missing patients at high risk for cardiac events who cannot be identified with LGE alone, we added SBPR during exercise testing to create a simple, convenient index for predicting outcomes in patients with DCM. SBP on exercise has been established as an important prognostic marker of cardiac events.21 Kitaoka et al13 reported that postexercise BPR was a simple and useful predictor of adverse cardiac events in patients with DCM. Since SBPR reflects the ability of the heart to increase stroke volume in response to exercise,11–14 ,22 that is, systolic and diastolic performance reserve during exercise, patients with SBPR <40 mm Hg may have underlying myocardial functional impairment that is not detected by morphological assessment such as LGE with CMR. In the present study, SBPR of 40 mm Hg was identified as the best cut-off value for predicting prognosis based on ROC curve analysis (figure 2A). Therefore, we divided the study patients into four groups according to the presence or absence of LGE and the SBPR cut-off. Indeed, the incidence of cardiac events was highest in the LGE-positive+SBPR <40 mm Hg group and lowest in the LGE-negative+SBPR ≥40 mm Hg group. Importantly, the event rate in the LGE-positive+SBPR ≥40 mm Hg and LGE-negative+SBPR <40 mm Hg groups were intermediate (figure 3). Based on the different rates for cardiac events in the four groups, our study demonstrated that the combination of LGE and SBPR provides more detailed risk stratification in patients with DCM than LGE or SBPR alone.
Regarding the combination of CMR and exercise testing for predicting prognosis in patients with DCM, Yamada et al23 reported that LGE-CMR combined with peak VO2-CPX can provide additional prognostic information on cardiac events. However, compared with our study, their study population had clinically mild DCM (prevalence of NYHA functional class I and II; 93% vs 56%). Furthermore, on multivariable analysis, peak VO2 was not an independent predictor of cardiac events in our study. Therefore, since our study population included patients with clinically moderate to severe DCM and there were more cardiac events, our present study provides more comprehensive information for assessing the risk of cardiac events in a broader spectrum of patients with DCM.
Recently, several studies have proposed that the measurement of T1 relaxation time, called T1 mapping, is potentially valuable for quantitative assessment of myocardial tissue composition on a global or regional level24 ,25 and that it is a promising technique for directly quantifying diffuse interstitial fibrosis in chronic HF.26 Furthermore, Dass et al27 suggested that since T1 values determined by T1 mapping are strongly correlated with impaired myocardial energetics, T1 mapping may detect functional changes in the myocardium prior to the development of fibrosis as evaluated by LGE. However, the relationship between T1 mapping and future cardiac events has not been fully elucidated. In addition, associations between myocardial T1 values and known prognostic physiological parameters in patients with DCM remain insufficiently characterised. Therefore, further investigations with larger samples are required to address this important issue.
Study limitations
Several limitations should be mentioned for the present study. First, since this was an observational study, we could not avoid differences in background characteristics among the four groups. Second, this study was limited by the relatively small number of patients examined and the small number of patients who experienced the primary end point during the study. A higher number of events is needed to provide adequate statistical power to fully evaluate whether a novel risk marker contributes additional prognostic information to an established set of risk factors in a multivariable model. Third, although lower glomerular filtration rate has been reported to be a prognostic factor in patients with chronic HF,28 patients with chronic renal insufficiency were excluded due to the risk of nephrogenic systemic fibrosis associated with gadolinium. Finally, the results from the stepwise selection process are potentially biased as a result of overfitting the derivation data set.
Conclusion
This study highlights the utility of the combination of LGE and SBPR during exercise for risk stratification in patients with DCM, and it cautions against overconfidence in risk stratification based on LGE assessment alone.
Key messages
What is already known on this subject?
-
Late gadolinium enhancement (LGE) has been established as a prognostic indicator in non-ischaemic cardiomyopathy. However, it is limited in its ability to detect diffuse interstitial fibrosis, which is commonly found in idiopathic dilated cardiomyopathy (DCM).
What might this study add?
-
To avoid missing patients at high risk for cardiac events by assessing LGE-positive status alone, we added systolic blood pressure response (SBPR) during exercise testing to a simple, convenient index for predicting outcomes in patients with DCM.
How might this impact on clinical practice?
-
The cardiac event rate in the LGE-negative+SBPR <40 mm Hg group was comparable with the rate in the LGE-positive+SBPR ≥40 mm Hg group. This finding cautions against overconfidence in risk stratification based on LGE-positive status alone. This combination of physiological (SBPR) and structural (LGE) indices can be used for risk stratification of cardiac events in patients with DCM.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
-
Contributors ET and TN contributed to the conception and design of the study and wrote this manuscript. YM and NY contributed to analysis of the MRIs. HI-U contributed to histological analysis and its interpretation. KN and YM provided statistical advice. YG and SY critically reviewed and revised the manuscript for intellectual content. TA and HO reviewed the manuscript.
-
Funding The present work was supported in part by the Takeda Science Foundation and the Japan Cardiovascular Research Foundation.
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval The institutional review board and the ethics committees of the National Cerebral and Cardiovascular Center.
-
Provenance and peer review Not commissioned; externally peer reviewed.