Article Text

Abstract
Background Interhospital transfer of patients admitted with an acute myocardial infarction for specialised care is common and costly. However, the long-term mortality of transferred patients compared with patients solely treated at the presenting hospital has not been evaluated. Here, we assess the long-term mortality of patients who undergo interhospital transfer during their acute myocardial infarction admission.
Methods We evaluated 40 482 patients with a ICD10-AM diagnosis of acute myocardial infarction admitted to hospitals in New South Wales, Australia, from 2004 to 2008, of whom 10 107 (25%) were transferred. We compared in-hospital and mortality up to 5.5 years postdischarge among transferred and non-transferred patients. We created a 1:1 propensity score matched cohort (n=16 854; 8427 per group) to account for selection bias.
Results In the matched cohort, transferred patients were more likely to undergo revascularisation (55.6% vs 13.7%, RR 4.05; 95% CI 3.83 to 4.29) and had lower mortality at 30 days (3.5% vs 5.7%, HR 0.60; 95% CI 0.52 to 0.70), 1 year (7.5% vs 12.6%, HR 0.58; 95% CI 0.52 to 0.64) and at the end of follow-up (15.3% vs 22.5%, HR 0.65; 95% CI 0.61 to 0.70) than patients treated in presenting hospitals. With the exception of transfers originating from revascularisation capable hospitals, these findings were consistent across a range of subgroups, including patients of all ages, ST-elevation myocardial infarction and non ST-elevation myocardial infarction patients, and transfers originating from hospitals in regional and major city areas. Sensitivity analyses showed that these findings are unlikely to be due to survival bias or to confounding by unmeasured variables.
Conclusions Patients hospitalised for an acute myocardial infarction who are transferred to one or more hospitals for specialised care have higher rates of coronary revascularisation and experience lower long-term mortality.
Statistics from Altmetric.com
Introduction
Interhospital transfer (IHT) of patients hospitalised for acute myocardial infarction (AMI) is common in contemporary AMI care. Indeed, 28%–45% of patients hospitalised for AMI are now transferred to another hospital during their AMI event1–4 with practice driven by clinical guidelines5 ,6 that suggest patients with AMI benefit from highly specialised services and interventions, most notably early coronary angiography and revascularisation by percutaneous coronary intervention (PCI). These specialised services are not universally available among hospitals, and IHT is the primary means for accessing these services for many hospitalised patients with AMI.
Recent observations, however, have questioned whether IHT leads to improved patient outcomes. Prior studies have shown that transferred AMI patients have a lower risk profile compared with non-transferred patients.2 ,3 ,7 This observation has raised concerns that patients who undergo IHT may not necessarily have improved outcomes from such intervention because high risk patients generally derive greater benefit from specialized care such as PCI.5 ,6 However, the absolute risk profile and outcomes of transferred patients have not been previously described. Furthermore, a recent US study showed no difference in hospital level, risk-standardised 30-day mortality between hospitals with a high versus low transfer rate for patients with AMI.8 While this was a hospital-level rather than a patient-level analysis, it nevertheless suggested that transfer was not beneficial as an intervention in AMI care to improve patient outcomes.
Existing observational studies of transferred patients with AMI have limited ability to address these concerns. Although many studies have evaluated emergent transfer of ST-elevation myocardial infarction (STEMI) patients, relatively few have evaluated transfer of admitted patients, most of whom have a non-ST-elevation myocardial infarction (NSTEMI), and who are further along in their illness. The few studies that have evaluated admitted patients report lower 30-day mortality among transferred patients, yet these studies are often from selected populations and rarely report risk-adjusted outcomes.1 ,2 ,7 Most importantly, prior studies have not reported long-term patient mortality.
Accordingly, we assessed whether hospitalised patients with AMI who are transferred for specialised care during their AMI event have lower long-term mortality compared with similar patients solely treated at the presenting hospital using data from a large population cohort from Australia. We specifically sought to assess patient mortality based on the risk profile of transferred patients and the consistency of findings among various population subgroups.
Method
Study population
The study population was derived from New South Wales (NSW), the most populous state of Australia. NSW has 7.24 million residents who are covered by national health insurance, with a proportion having supplementary private insurance. All hospitalisations and deaths are recorded within the NSW Admitted Patient Data Collection (APDC) and the linked Register of Births, Deaths and Marriages, respectively.9 Diagnostic and procedural coding within the APDC is based on the International Classification of Disease 10 Australian Modification (ICD10-AM). Reported coding accuracy of Australian hospital admissions data sets is 85% with the coding of cardiac diagnoses having a high correlation with chart extracted data.10
We included all patients with a principal diagnosis of AMI as defined by ICD10-AM codes I21.0-I21.3 (STEMI) and I21.4 (NSTEMI) with a hospitalisation between 1 July 2004 and 30 June 2008. For patients with multiple AMI admissions during this study period, only the first admission contributed to the analysis. We excluded patients with a length of stay ≤1 day unless the patient died or was transferred to another hospital as these admissions were unlikely to represent an AMI admission. Patients were stratified into those who were solely treated at their presenting hospital and those who required IHT to one or more acute care hospitals. We excluded episodes of transfers to or from non-acute care facilities such as aged-care facilities.
Outcome measure
The primary outcome was all cause mortality assessed in-hospital and at 30 days, 1 year and long term. Long-term mortality was defined as any death occurring during the overall follow-up period from the index admission. Vital status was confirmed up to 1 January 2010 for all patients providing a follow-up period of up to 5.5 years (median 3.5 years). The secondary outcomes were in-hospital receipt of coronary angiography, PCI or coronary artery bypass grafting (CABG) at any time during the AMI event.
Statistical analysis
Data are summarised as frequencies and percentages for categorical variables. Continuous variables are presented as mean±SD or median and IQR. The χ2 statistic and Student's t test were used to compare those who did and did not undergo IHT as appropriate.
Propensity score analysis
We used propensity matching to account for differences in baseline characteristics arising from non-random assignment of transfer status. We developed a propensity score, indicating the conditional probability that any individual patient would undergo IHT, using a non-parsimonious logistic regression model. Patient demographic characteristics, diagnosis (STEMI/NSTEMI), cardiac history, comorbidities and acute complications were included in the model. Cardiac history and comorbidities were derived from the secondary diagnosis and procedure codes from the index hospitalisation and the principal and secondary codes from all hospitalisations in the preceding 12 months. These ICD10-AM codes were grouped into condition categories used in prior studies11–13 after cross-walking from ICD9 to ICD10-AM. Acute complications were derived solely from the secondary diagnosis and procedure codes from the index hospitalisation. Additionally, presentation hospital characteristics including hospital region, revascularisation (PCI and CABG) capability, and hospital type were included in the propensity score model. Selected variables from the propensity score model are displayed in table 1 (complete list of included variables are provided in the online supplementary appendix).
Selected patient characteristics at presentation*
Transferred patients were then matched 1:1 without replacement to the closest non-transferred patients based on the propensity score using published algorithms14 to derive a propensity score matched (PSM) cohort. Significance testing in the PSM cohort was performed using McNemar's test for categorical variables and paired t test for continuous variables. Non time-to-event outcomes were compared using relative risk (RR) estimate with 95% CI for the PSM cohort derived as described by Agresti et al15 Unadjusted event free survival curves were generated using Kaplan–Meier estimates and compared using the log-rank test. Adjusted survival curves were estimated using a marginal survival model with robust SEs. All time-to-event outcomes (30 days, 1 year and long-term mortality) were reported as HRs and 95% CI.
Subgroup analysis
To assess patient outcomes based on the patient risk profile at presentation, we assessed outcomes by patient's predicted risk at presentation. Patient's predicted risk strata were derived from a logistic regression analysis using baseline characteristics to predict 30-day mortality using published methods12 and stratifying patients to quartiles of risk.
Due to the potential heterogeneity of transferred patients, we evaluated the outcomes in prespecified subgroups. Specifically, we performed prespecified subgroup analyses of mortality by age, gender, diagnosis, presence of private medical insurance, hospital revascularisation capacity and the region of the presenting hospital. For example, we compared the outcomes of patients undergoing IHT from non-revascularisation capable hospitals and from revascularisation capable hospitals because reasons for IHTs occurring in the former situation (primarily for coronary angiography and revascularisation) may be distinctly different from transfers occurring from revascularisation capable hospitals.
Sensitivity analysis
Sensitivity analyses were performed to evaluate the robustness of the parameter estimates. Since survival bias resulting from the death of patients without the opportunity for transfer is a possible confounder, we repeated the analysis excluding patients who died in hospital. Since clinical variables that may influence IHT such as pathology results and clinical examination findings are not recorded in the APDC, a sensitivity analysis was conducted to explore the effects of potential unmeasured confounders using published methods.16 Lastly, to derive an estimate the effect of transfer status on mortality using data from the entire cohort, we performed a propensity analysis using stabilised inverse probability treatment weights.17 A p value of <0.05 was used as a cut-off for statistical significance. All analyses were performed using SAS V.9.2 (SAS Institute, Cary, North Carolina, USA).
The NSW Population Health Research Ethics Committee provided ethical approval for the study.
Results
Characteristics of the overall study cohort
The final study cohort consisted of 40 482 patients from 161 hospitals that met the study inclusion and exclusion criteria (figure 1 and table 1). IHT to one or more acute hospitals occurred for 10 107 (25.0%) patients while 30 375 (75.0%) patients received care solely at the presenting hospital. Overall, transferred patients were younger and more likely to be male, had private health insurance, and had a diagnosis of STEMI. Transferred patients also had fewer cardiovascular risk factors, comorbidities, and acute complications at presentation (all p values <0.05 with the exception of prior CABG).
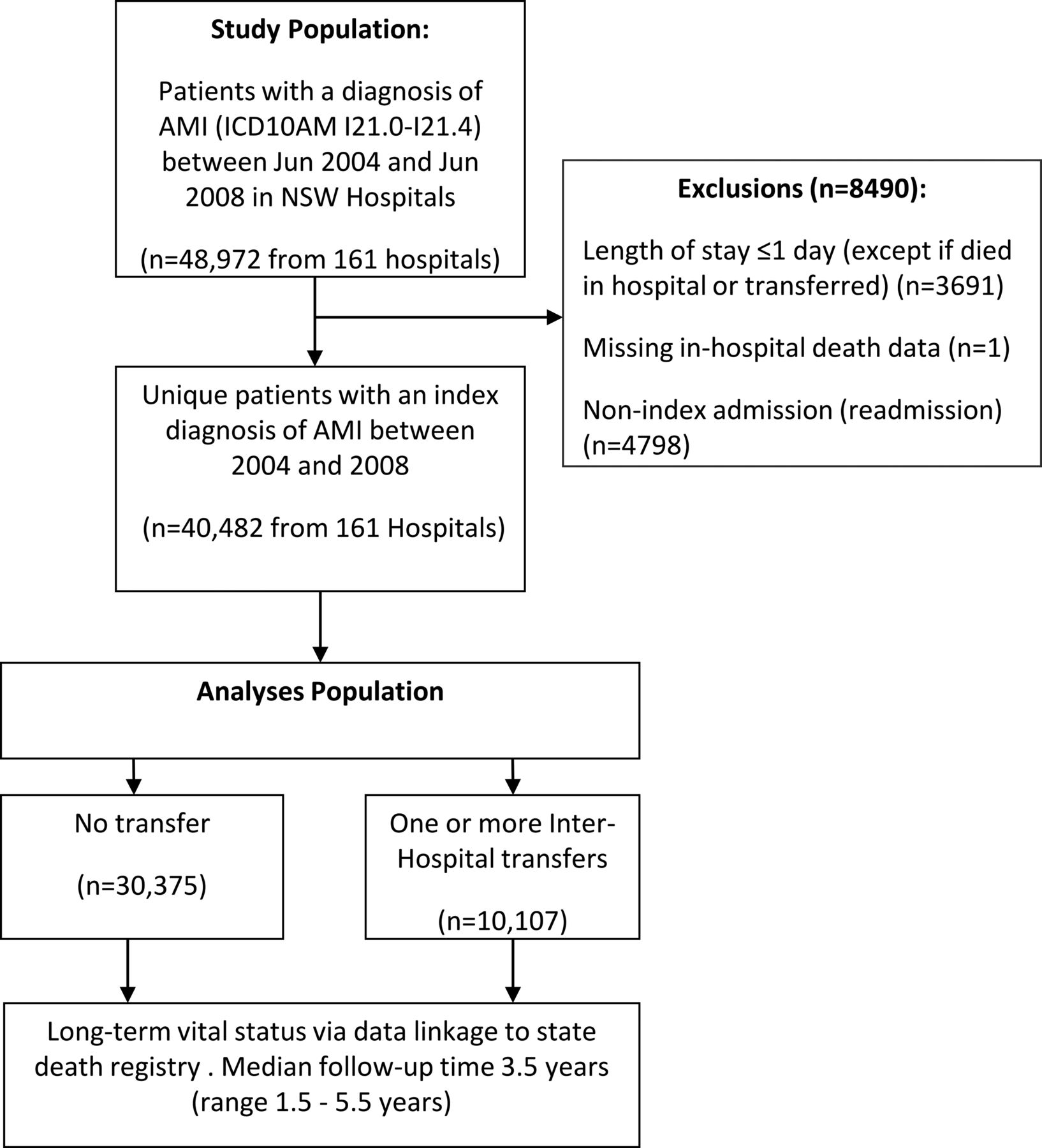
Patient selection flow diagram. Abbreviations are as described within the manuscript.
Transferred patients were more likely to present to hospitals in regional and remote areas and to a hospital without revascularisation capability. The first transfer mainly occurred to hospitals located in major cities (92.0%) with revascularisation capabilities (94.3%) and these were mainly public principal referral (64.9%) or private (32.8%) hospitals.
PSM cohort
A propensity score model with a good discriminatory capacity (c statistic 0.79) was derived using 72 measured baseline variables. The propensity score distributions for transferred and non-transferred patients showed good overlap (see online supplementary appendix figure 1). Based on 1:1 matching, 8427 matched pairs were derived (n=16 854). Covariate balance was achieved post matching as shown by a lack of a difference between groups for 71/72 variables (all p>0.05 except valvular heart disease, see table 1) and a reduction in the absolute standardised difference to negligible levels (median standardised difference at baseline of 8.31 (IQR 4.2–16.0) vs 0.74 (IQR 0.28–1.42) postmatching, p<0.01).
Outcomes
Coronary angiography and revascularisation
Overall, an invasive cardiac procedure (coronary angiography, PCI or CABG) was performed in 23 202 (57%) of patients with 13 805 (34%) undergoing revascularisation (PCI or CABG) during their AMI event. An invasive cardiac procedure was performed in 90% of transferred patients. Once matched for baseline characteristics, transferred patients were more likely to receive a cardiac procedure (PSM 89.2% vs 30.4%, RR 2.93; 95% CI 2.84 to 3.04) and in-hospital revascularisation (PSM 55.6% vs 13.7%, RR 4.05; 95% CI 3.83 to 4.29) compared with non-transferred patients (table 2).
Patient outcomes
All-cause mortality
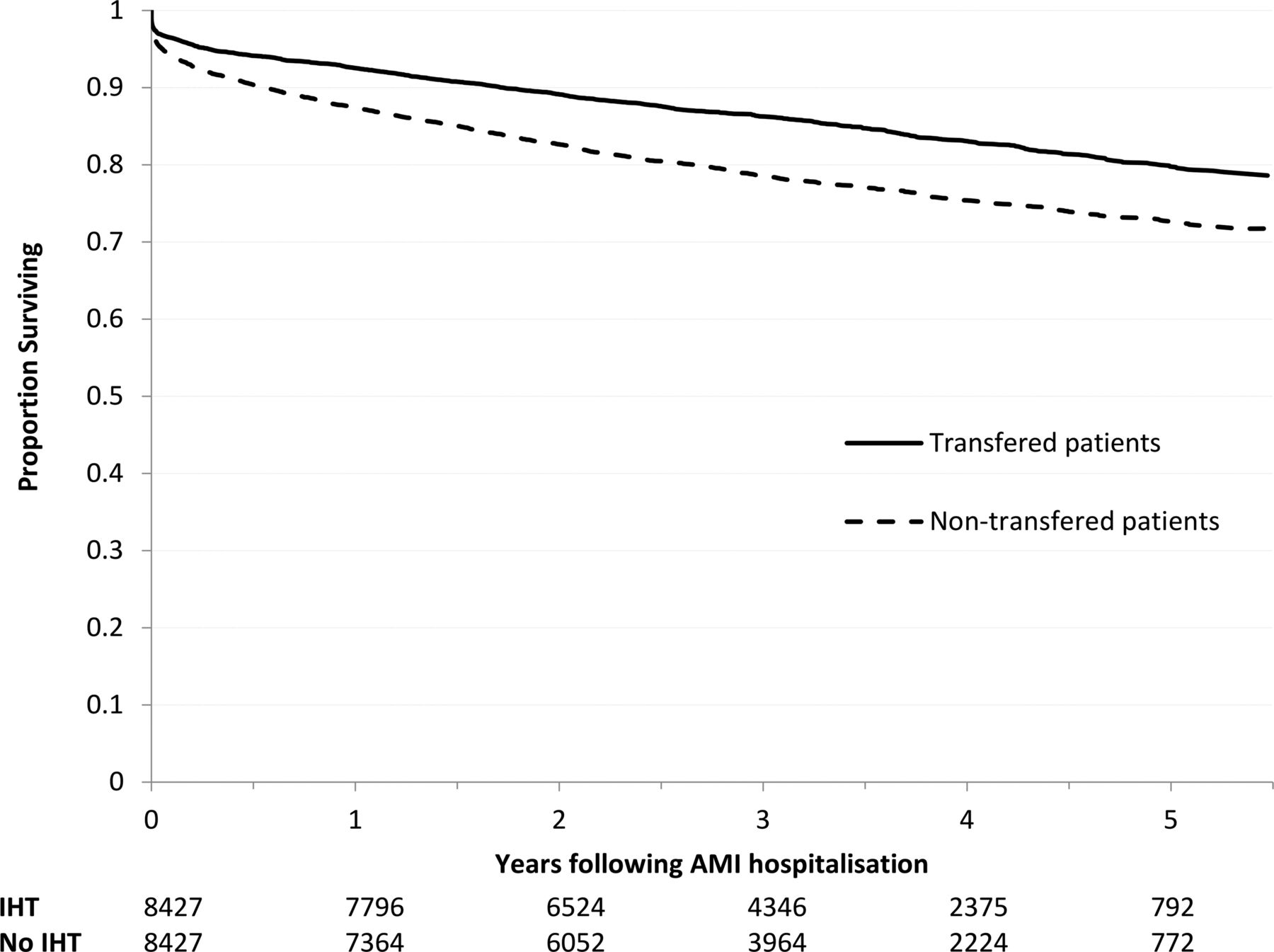
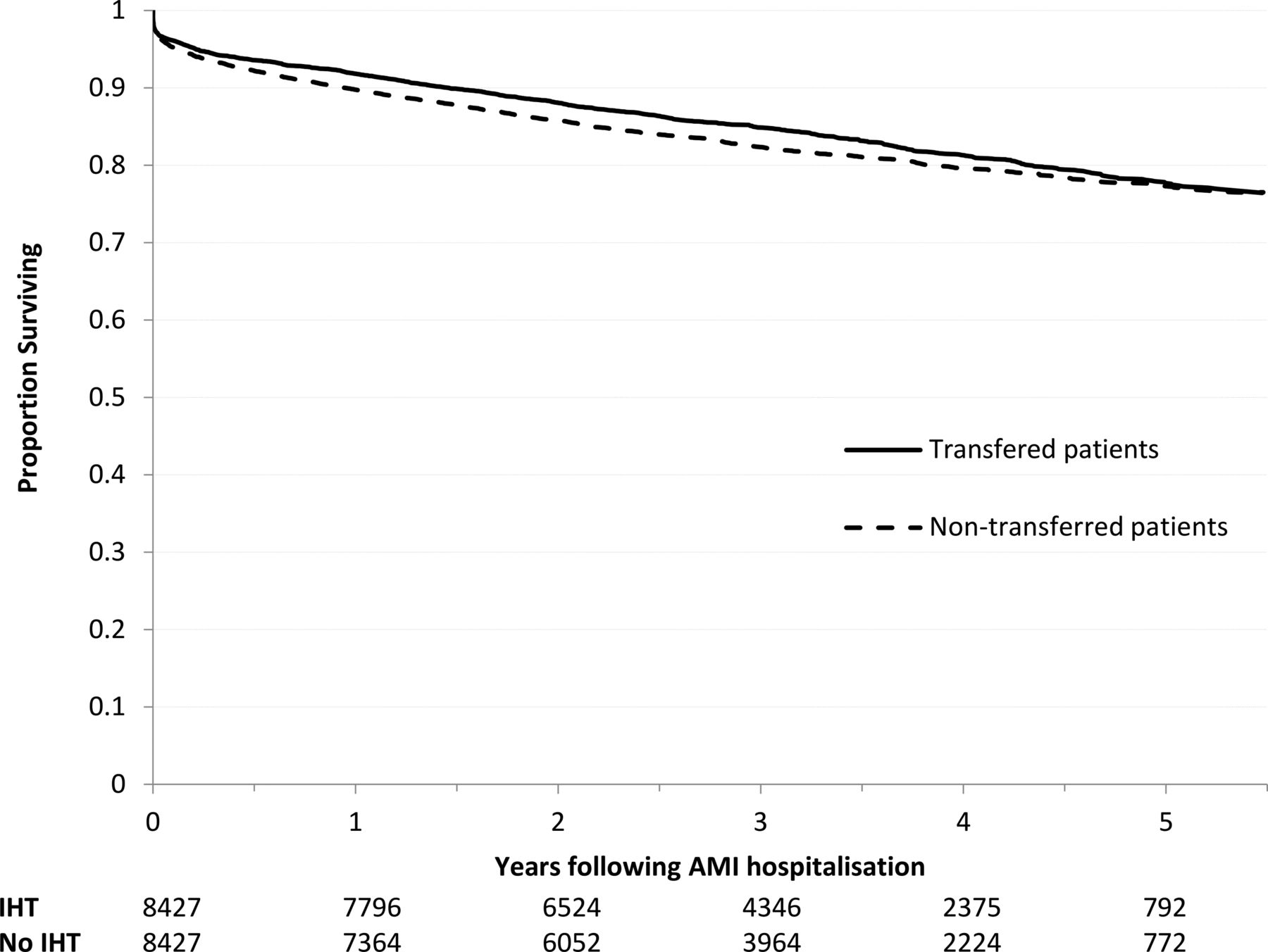
In the overall cohort, 10 759 (26.6%) patients had died at the end of the follow-up period with a lower crude mortality rate among transferred patients (table 2, figure 2). Once PSM for baseline patient characteristics, transferred patients had lower in-hospital mortality (PSM 2.9% vs 4.2%, RR 0.67; 95% CI 0.57 to 0.79), 30-day mortality (PSM 3.5% vs 5.7%, HR 0.60; 95% CI 0.52 to 0.70), 1-year mortality (PSM 7.5% vs 12.6%, HR 0.58; 95% CI 0.52 to 0.64) and long-term mortality (PSM 15.3% vs 22.5%, HR 0.65; 95% CI 0.61 to 0.70, figure 3).

Kaplan–Meier survival curves indicating unadjusted rates of survival in the transferred and non-transferred patients in the overall cohort. AMI, acute myocardial infarction; IHT, interhospital transfer.

Kaplan–Meier survival curves indicating rates of survival in the transferred and non-transferred patients in the propensity score matched cohort. AMI, acute myocardial infarction; IHT, interhospital transfer.
The 30-day and long-term mortality benefit of IHT was reduced, but remained significant following adjustment for receipt of in-hospital revascularisation in the PSM cohort (adjusted PSM HR for 30-day mortality 0.81; 95% CI 0.70 to 0.95, adjusted PSM HR for long-term mortality 0.89; 95% CI 0.83 to 0.96, figure 4).

Rates of survival in the transferred and non-transferred patients in propensity score matched cohort adjusted for difference in receipt of in-hospital revascularisation. AMI, acute myocardial infarction; IHT, interhospital transfer.
Subgroup analyses
Stratifying patients in the PSM cohort into risk strata, based on predicted mortality at presentation, appropriately stratified patients into quartiles of actual 30-day and long-term mortality (table 3). Our results show most transferred patients (75% or top 3 quartiles of risk) have an absolute risk profile indicative of moderate-to-high patient risk as indicated by an actual mortality within quartiles ≥1.3% at 30-days and ≥8.7% at the end of follow-up. Within each risk strata, transferred patients also had lower mortality compared with patients treated solely at the presenting hospital.
Mortality in the propensity score matched cohort by risk-strata (quartiles) at presentation
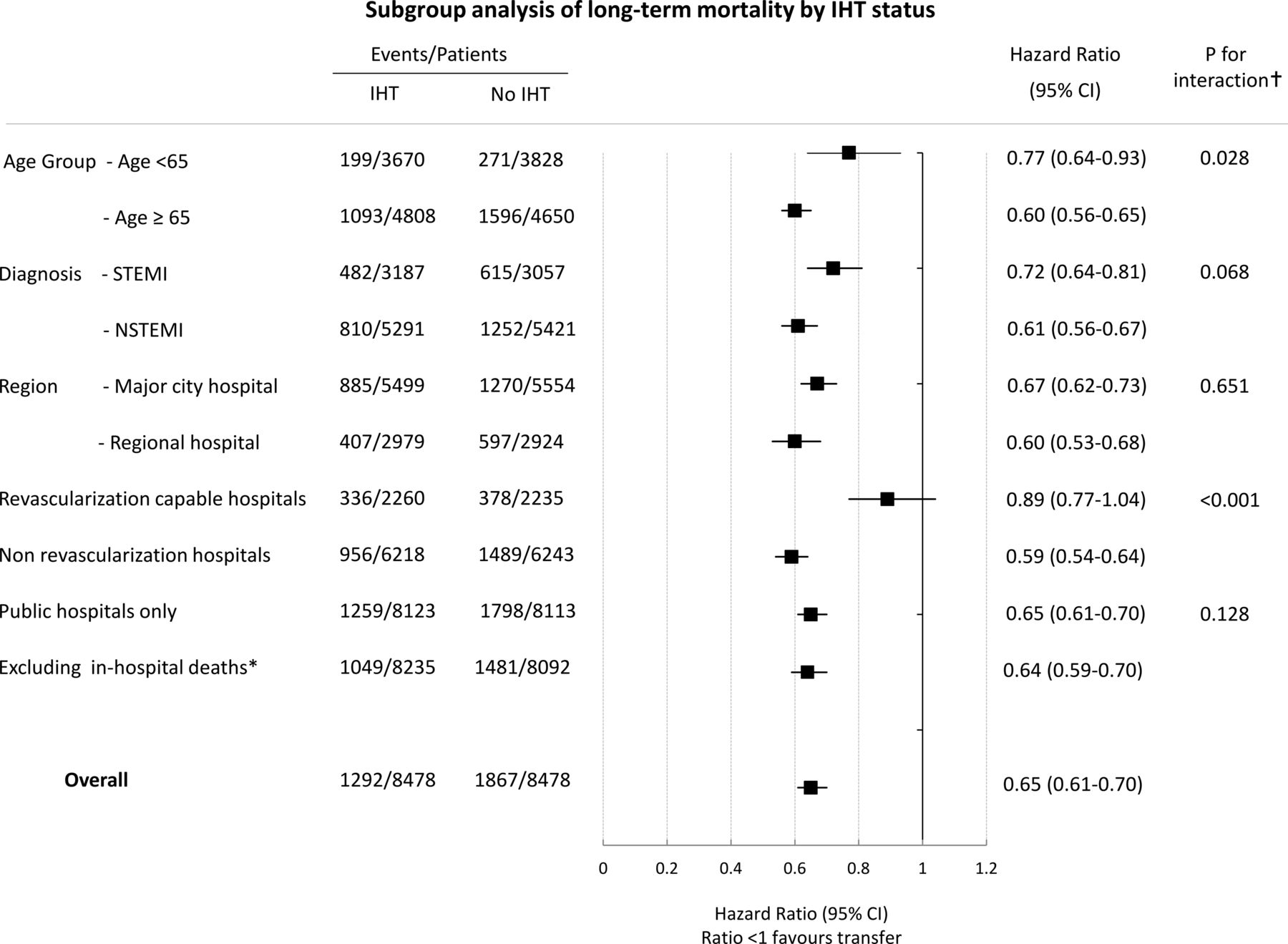
Further subgroup analysis showed that transferred patients had lower 30-day and 1-year mortality in all subgroups except in patients transferred from revascularisation capable hospitals where IHT was not associated with a lower mortality (p for interaction <0.001, figure 5 and see online supplementary appendix figure 2). Patients aged ≥65 years may have a greater long-term benefit from IHT as indicated by weak effect modification (p for interaction 0.028). Subgroup analysis conducted by stratifying the overall cohort by the type of AMI (STEMI vs NSTEMI) and performing propensity score matching within each strata to derive a matched cohort for STEMI and NSTEMI respectively yielded results that were similar to the overall analyses (see online supplementary appendix).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Subgroup analysis of long-term mortality between transferred and non-transferred patients. †P for statistical interaction with IHT, *No interaction term calculated as in-hospital death directly affects long-term mortality. AMI, acute myocardial infarction; IHT, interhospital transfer; STEMI, ST-elevation myocardial infarction; NSTEMI, non-ST-elevation myocardial infarction.
Sensitivity analyses
The lower mortality among transferred patients persisted with the exclusion of in-hospital deaths (30-day mortality HR 0.41; 95% CI 0.30 to 0.56; long-term mortality HR 0.64; 95% CI 0.59 to 0.70). This suggests that survivorship bias is unlikely to explain the mortality difference observed.
Our results show that for a single independent unmeasured binary confounder, present prior to transfer, to explain the observed lower mortality with IHT, the confounder would require a markedly higher (1.6-fold to 20.0-fold) prevalence among the non-transferred patients with an accompanying increase in mortality with HR varying between 1.5 (if the confounder is common) to 6.0 (if the confounder is uncommon) (see online supplementary appendix figure 3). These large imbalances would have to occur despite matching for other measurable characteristics. Lastly, analysis using inverse probability treatment weights showed that IHT continued to be associated with lower mortality although the effect size was reduced compared with the analysis (HR for long-term mortality 0.76, 95% CI 0.74 to 0.79, see online supplementary appendix).
Discussion
In this study, we show that a quarter of hospitalised patients with AMI undergo transfer to another acute care hospital during their AMI event. These transferred patients have higher rates of coronary revascularisation and experience lower long-term mortality than similar patients treated solely at the presenting hospital. With the exception of transfers originating from procedural hospitals, these findings were consistent across a range of subgroups, including patients younger and older than 65 years of age, STEMI and NSTEMI patients, and transfers originating from hospitals in regional and major city areas. Sensitivity analyses showed that these findings are robust and unlikely to be due to survival bias or to confounding by unmeasured variables.
We report outcomes for large groups of transferred patients that have not been previously studied, and our findings show for the first time that transferred patients with AMI have lower long-term mortality. IHT has been evaluated only in a randomised manner for emergent transfer in STEMI.18–22 In contrast, the transfer of admitted patients, most of whom have an NSTEMI, and who are further along in their illness, stems from generalisation of trials of routine invasive management.23–25 This is reasonable given many of these trials included transferred patients and were in the absence of randomised trials of IHT as an intervention in NSTEMI. Prior observation studies of IHT have focused on selected populations such as Medicare beneficiaries aged ≥65 years, and transfers originating from rural, community or non-procedural hospital.1–3 ,7 This is, in part, because IHT is thought to occur mainly in these populations. However, we show that 37.6% of transferred patients are among patients aged ≤65 years, 66.8% of transfers originate from major cities, 57.2% from tertiary hospitals and 22.5% originate from revascularisation capable hospitals; large groups of transferred patients with AMI who had been hitherto unstudied. Of the existing observational studies of IHT, three have reported lower crude 30-day mortality among transferred patients with AMI (crude OR/RR 0.32–0.57)1 ,2 ,7 with one study reporting a 20% lower adjusted 30-day mortality,1 comparable with the lower 30-day mortality among transferred patients in our study. We extend these prior observations by showing for the first time that transferred patients with AMI experience lower long-term mortality.
Our findings suggest that many patients who undergo IHT have an intermediate-to-high absolute risk of mortality. Although transferred patients do have a lower baseline risk profile compared with non-transferred patients consistent with prior studies,1–3 ,7 our results show that most transferred patients have an absolute risk profile considered as intermediate-to-high risk when compared with clinical risk models.26 ,27 For example, 75% of transferred patients had an absolute mortality of at least 1.3% at 30 days and 8.7% long term (table 3). This provides reassurance that patients who are transferred are likely to derive benefit from invasive therapy and other specialised care, given that intermediate-to-high risk patients are known to derive the greatest benefits from contemporary AMI therapies.5 ,6
Our observations show that the lower mortality among transferred patients is explained only partially by greater access to revascularisation. Benefits of IHT are often perceived to be solely due to increased access to invasive coronary procedures. However, we hypothesise that important differences in other aspects of care such as greater use of evidence-based treatments among transferred patients are likely to also contribute to the lower mortality among transferred patients. Our study did not measure these treatments as they are not recorded in the NSW APDC. However, our reasoning stems from prior studies that have shown transferred patients are more likely to receive evidence-based therapies such as antiplatelet and antithrombotic agents,1 ,2 are more likely to be cared for under a cardiology service, and are more likely to undergo prognostically significant evaluations such as stress testing or assessment of LV function.3 Higher rates of these beneficial therapies may explain the residual difference in mortality following adjustment for receipt of revascularisation. Our hypothesis is further supported by our observation that a significant difference in mortality was not observed for transfers originating from revascularisation capable hospitals. This may reflect the lack of a treatment differential between groups at these better resourced feeder hospitals. These observations are important because improving medical care at acute hospitals without specialised cardiac services may improve outcomes for patients with an AMI.
Our analysis has strengths and limitations. Hospital administrative data sets vary in accuracy and may underestimate the prevalence of risk factors and comorbidities. However, the accuracy of Australian hospital administrative data sets is only marginally inferior to accuracy reported in registry data sets.28 The effect of selection bias on our findings is further minimised by propensity score matching with minimal residual confounding. Propensity score matching is accepted as the optimal posthoc statistical method to derive an unbiased estimate of the treatment effect when subjects are not randomly assigned to treatment groups.29 APDC is an administrative database and does not contain clinical variables such as receipt of medical therapy including thrombolysis for STEMI patients that may influence the decision to transfer. However, our sensitivity analysis suggested the lower mortality observed among transferred patients unlikely to be negated by the presence of an unmeasured confounder. Nevertheless, residual bias due to unmeasured confounding is not completely excluded due to the observational nature of the study. Lastly, our time-to-event analysis does not take into consideration clustering of patients within hospitals, which may affect the estimate of effect size associated with IHT.
Key messages
What is already known on this subject?
Interhospital transfer of patients hospitalised for acute myocardial infarction (AMI) is exceedingly common in contemporary AMI care.
However, this practice is not supported by a wealth of data and there is concern that many transferred patients with AMI in clinical practice may not experience improved long-term outcomes.
What might this study add?
Most patients with an AMI transferred to one or more hospitals for specialised care are at moderate to high risk of long-term mortality.
Transferred patients have higher rates of coronary revascularisation (55.6% vs 13.7%, RR 4.05; 95% CI 3.83 to 4.29) and experience lower long-term mortality (15.3% vs 22.5%, HR 0.65; 95% CI 0.61 to 0.70) compared with patients treated solely at the presenting hospital.
How might this impact on clinical practice?
These findings support interhospital transfer of hospitalised AMI patients as an effective intervention for gaining access to specialised services and may improve long-term outcomes for appropriate patients with AMI.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
Twitter Follow Isuru Ranasinghe at @isranasinghe
Contributors IR: conceived the study, analysed the data, and wrote the draft manuscript. FB: assisted with statistical analysis and contributed to the preparation of the manuscript. DB: contributed to the critical review of the manuscript. MG: obtained the data and the ethical approval for the study and contributed to the critical review of the manuscript.
Funding IR is supported by an early career fellowship co-funded by the National Health and Medical Research Council and the National Heart Foundation of Australia (Grant ID 1054353).
Competing interests None.
Ethics approval The NSW Population Health Research Ethics Committee.
Provenance and peer review Not commissioned; externally peer reviewed.