Article Text

Statistics from Altmetric.com
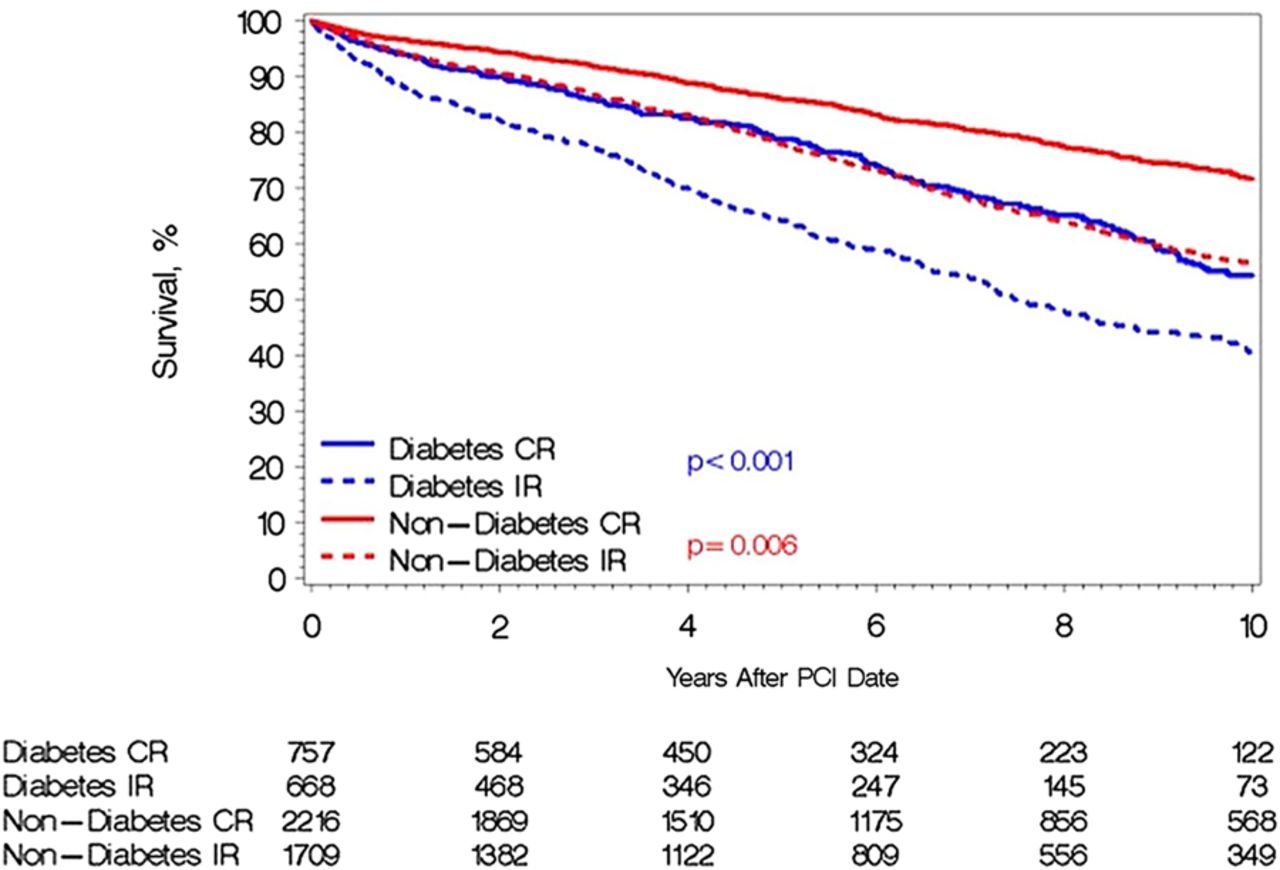
In patients with multivessel coronary artery disease, it remains unclear whether percutaneous coronary intervention (PCI) to relieve obstructions in as many affected coronary arteries as possible (complete revascularization, CR) is more beneficial than incomplete revascularization (IR), typically treating only the lesion causing the acute event. This issue is particularly relevant in diabetic patients given the increasing prevalence of diabetes in many countries and the association of diabetes with multivessel coronary disease. To test the hypothesis that CR provides more benefit than IR in diabetic patients, Jiménez-Navarro and colleagues (see page 1233) compared cardiovascular outcomes in a consecutive series of 5340 patients with multivessel disease undergoing PCI with about 27% having diabetes (figure 1). In both patients with and without diabetes, mortality rates were higher with IR compared to CR, but the absolute risk was higher for patients with diabetes with a 5 year mortality of 21.2% with CR, versus 35.8% with IR.

Unadjusted mortality curves during follow-up for patients with diabetes and patients without diabetes according to complete (CR) or incomplete revascularisation (IR). PCI, percutaneous coronary intervention.
In an accompanying editorial, Sanchez and Villcorta (see page 1176) concur that in patients with coronary artery disease “the prognosis for diabetics is worse, after either PCI or CABG, in comparison with non-diabetics” and that “these data provide a rationale for revascularising diabetics more aggressively. In fact, the authors show that CR is associated with a significant, and higher in magnitude, reduction of 42% in mortality in diabetics compared with 36% in non-diabetics”. They go on to suggest “CR should be the aim of myocardial revascularisation in diabetics with stable and unstable multivessel CAD undergoing PCI”.
Another clinical situation where CR verus IR remains controversial is the patient presenting with an ST-segment elevation myocardial infarction (STEMI) and cardiogenic shock. Starting with a nationwide Korean registry of over 16 thousand patients with STEMI undergoing primary PCI over a 6 year period, Park and colleagues (see page 1225) identified 510 patients with cardiogenic shock. The adjusted risk of in-hospital mortality was lower in the 24% of patients who underwent multivessel CR compared to those having revascularization of only the culprit vessel (2.4 vs 9.3%, HR 0.263, 95% CI 0.149 to 0.462, p<0.001). The beneficial effect of CR on all-cause death was still evident a median follow up of 194 days (4.8% vs 13.1%, HR 0.400, 95% CI 0.264 to 0.606, p<0.001) (figure 2). It is a bit surprising that the survival rate was close to 90% for these patients with STEMI and cardiogenic shock; perhaps this registry included lower risk patients than in previous studies.

The inverse probability of treatment weight-adjusted survival curves free from cardiac death (A), recurrent myocardial infarction (MI; B), any revascularisation (C) and major adverse cardiac events (MACE; D) between culprit vessel (CV) and multivessel (MV) revascularisation.
Henry and Uberoi remind us that “For patients with STEMI presenting without cardiogenic shock, PCI of a non-culprit vessel is currently considered a class III indication, meaning the risk outweighs the benefit and the procedure SHOULD NOT be performed (not helpful and may be harmful). Despite the Class III indication, registries indicate 10–25% of patients with STEMI in fact undergo multivessel PCI”. Recently reported randomized clinical trials, including Complete Versus Lesion-only Primary PCI Trial (CvLPRIT) and PReventive Angioplasty in Myocardial Infarction (PRAMI) that excluded patients with cardiogenic shock, will likely influence future guideline statements. In contrast, current guidelines “state that complete revascularisation in patients with multivessel disease with cardiogenic shock is a class I recommendation, meaning the benefit far outweighs the risk and the procedure SHOULD be performed” despite a paucity of data to support this approach. After discussing the limitations of the registry data in the current study, Henry and Uberoi conclude that the Korean “investigators should be congratulated for increasing our knowledge regarding patients with STEMI with multivessel disease and cardiogenic shock”.
Our knowledge about adult congenital heart disease (ACHD) is rapidly expanding with the increasing number of patients with these conditions surviving to adulthood and the establishment of tertiary ACHD centers with data collection on clinical outcomes. Choudhary and colleagues (see page 1190) add to this knowledge base with a report of outcomes in 151 patients with isolated aortic coarctation followed over 20 years. Although actuarial survival was 89% at 60 years of age, 44% had hypertension and aortic complications were common with recurrent coarctation in 34% and aneurysms of the descending thoracic aorta in 18%.
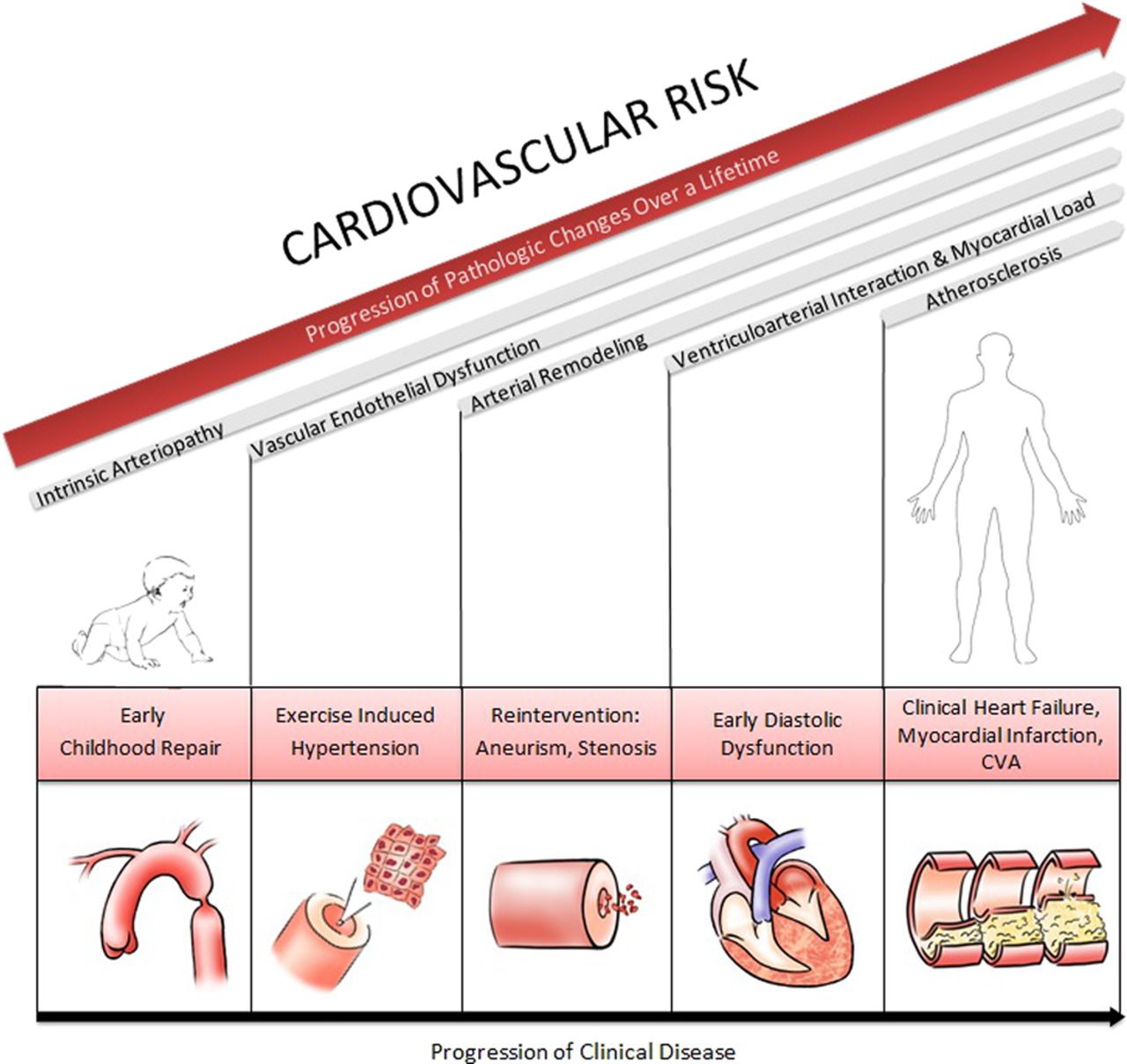
Bhatt and Yeh (see page 1173) graphically summarize the long term cardiovascular risk associated with repaired aortic coarctation (figure 3) emphasizing that “simple or ‘Isolated’ coarctation of the aorta is an example of a disease process requiring us as clinicians to understand the interaction of inherent risk (genetic determinants, intrinsic arteriopathy) with superimposed anatomic (native and intervened aortic), physiological (compliance, blood pressure, flow) and environmental (smoking, overweight, diabetes, sedentary lifestyle) modifiers, in a longitudinal construct”. Further they remind us that “Despite successful repair of aortic coarctation, individuals remain at elevated risk of premature atherosclerosis and early mortality. Coronary artery disease is documented in 25%–37% of cases and remains the most common cause of death”.
{kind=link}
{kind=link}
{kind=link}
Longitudinal outcomes in coarctation. Superimposed pathophysiological changes and related clinical consequences over the lifespan are demonstrated.
In this issue of Heart, Bhatnager and colleagues (see page 1182) summarize data from the 2014 epidemiology of cardiovascular disease (CVD) in the United Kingdom (UK) that will be of interest to clinicians, researchers and health policy experts. Although CVD remains the most common cause of death in women, accounting for 28% of all deaths, cancer is now the most common cause of death in men. Professor Adam Timmis comments “The report provides a timely reminder that in younger women too CVD kills more women than breast cancer. Most of these CVD deaths in young women are caused by myocardial infarction, which is largely preventable through modification of risk factors, and if the national effort put into the detection of breast cancer could be matched in protecting young women against myocardial infarction many more lives would probably be saved. People think that CVD continues to be a problem for men, not women. This perception is wrong when CVD is killing more women than men—and more young women than are dying from breast cancer. These key statistics from the 2014 report need wide dissemination”. We should all heed this advice, not only educating our patients and the public, but also ensuring that women of all ages are screened for CVD risk factors and receive appropriate primary prevention therapy.
The Education in Heart article (see page 1240) in this issue reviews the causes and natural history of noncardiac chest pain and summarizes the approach to diagnosis and management of this common clinical symptom.
The Image Challenge (see page 1232) in this issue will teach you something you probably did not already know about inherited causes of sudden cardiac death.
Linked Articles
- Editorial
- Education in Heart
- Editorial
- Congenital heart disease
- Review
- Coronary artery disease
- Coronary artery disease