Article Text

Statistics from Altmetric.com
Prevention of atrial fibrillation (AF) would positively impact global health by decreasing stroke, heart failure and cardiovascular mortality, as well as by improving quality of life for many patients. Older age, hypertension, and obesity are associated with an increased risk of AF in patients without underlying valvular heart disease, heart failure or coronary disease. However, the effects of chronic exercise on AF risk are controversial. Studies in men suggest a lower risk of AF in older men engaging in moderate physical activity, but a higher risk of future AF in younger men engaged in frequent, long-term, intense levels of activity.1 ,2 Few studies have examined the relationship between exercise and AF risk in women.
In the Swedish Mammography Cohort of over 36 thousand middle-aged women, with a median age of 60 years, about 8% were diagnosed with new AF during 12 years of followup (see page 1627). Increasing levels of leisure time physical activity at study entry were associated with a lower risk of AF with a relative risk of 0.85 (95% CI 0.75 to 0.95) for ≥4 hours/week versus <1 hour/week. The effect of walking or bicycling for transport was similar with a relative risk of 0.81 (95% CI 0.72 to 0.99) for ≥40 minutes/day versus almost never (figure 1). In this study, a moderate amount of physical activity was adequate to reduce AF risk with no evidence for an adverse effect of high levels of exercise.

Kaplan–Meier survival curves (unadjusted) (ie, free of atrial fibrillation (AF)) for the two extreme groups of leisure-time exercise (A) and walking/bicycling (B) at study entry.
In one of a set of linked editorials, Gjesdal and Grundvold (see page 1605) remind us that: “There are a number of differences between the male and female heart with respect to AF. Women have a higher age of AF onset, a greater risk of embolic stroke, a poorer quality of life, a higher heart rate during AF, more adverse effects to antiarrhythmic drugs, a different pattern of AF trigger localisation and differences in how the autonomic nerve system modulates cardiac electrophysiology. Thus, it is reasonable to assume that also the cardiac response to physical activity may differ between the genders.” In the second editorial, Guasch and Mont (see page 1607) put the current study into the context of the published literature in an elegant figure (figure 2). Both editorials point out that while the data convincingly support the conclusion that moderate exercise in older women is associated with a lower risk of AF, the data on extreme exercise in younger women remains incomplete because societal norms for physical activity have changed dramatically over the lifetime of the women in this study.

Graphical summary of some representative studies assessing exercise-induced atrial fibrillation (AF) risk depending on the gender composition and design of the study. Upper panel: Overall percentage of women included for each type of study, from initial small case–control/cohorts studies (<1000 individuals included) to male/both gender or women-exclusive epidemiological studies (>3000 individuals). Lower panel: Relative risk (RR) or OR of exercise-induced AF (sedentary vs the most intense group) in these studies, represented along their publication year and coloured according to the study design.
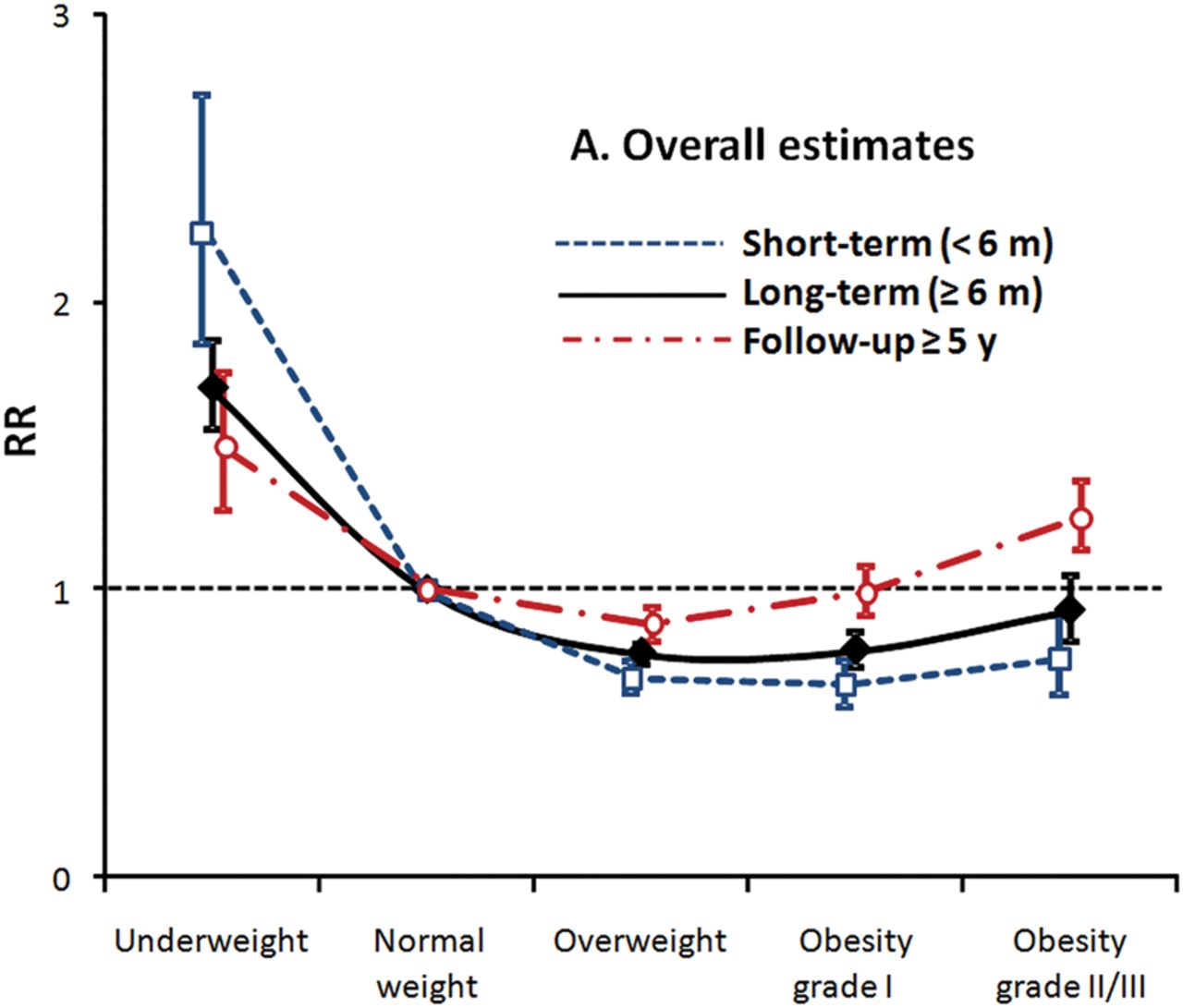
The association between body mass index (BMI) and prognosis in patients with coronary artery disease was examined in a meta-analysis that included over 1.3 million patients from 89 published studies (see page 1631). Long-term mortality (after 5 years) was higher in the most obese patients (BMI ≥35 kg/m2) with a relative risk of 1.25 (CI 1.14 to 1.38) compared to normal weight patients. Somewhat surprisingly, short term (<6 months) mortality was lower in overweight and obese patients with a risk ratio of 0.76 (CI 0.62 to 0.91) for the most obese patients (figure 3). Although a J-shaped relationship between BMI and cardiovascular mortality was seen across different treatment strategies, this inverse association was attenuated on meta-regression analysis over longer followup.
{kind=link}
{kind=link}
{kind=link}
Relative risks of all-cause mortality by BMI categories from all estimates. Separate analyses were performed among studies with short-term estimates (<6 months, blue dotted line), long-term estimates (≥6 months, black solid line) and studies with follow-up ≥5 years (red dashed line). The Y-axis represents the RRs of all-cause mortality for BMI categories using normal weight group as the reference by random effects. RR, relative risk.
In the accompanying editorial, Lavie, Schutter and Milani (see page 1610) summarize the obesity “paradox” – in patients with established heart disease obesity is not associated with a higher risk of short-term adverse outcomes, even though obesity is associated with an increased prevalence of cardiovascular risk factors and thus a higher risk of developing heart disease. The biological basis for the J-shaped relationship between BMI and outcomes is not clear but may relate to increased lean body mass (as well as fat) in obese patients and the confounding effects of cardiorespiratory fitness in patients across the BMI range. The authors conclude: “Certainly, promoting physical activity throughout our healthcare system is urgently needed, and this may go a long way to prevent obesity, especially more severe degrees of obesity, as well as improving cardiorespiratory fitness and prognosis in the primary and secondary prevention of cardiovascular disease, including coronary heart disease”.
Risk stratification of patients being considered for transcatheter aortic valve implantation (TAVI) continues to evolve as TAVI becomes more widely utilized. The impact of concurrent pulmonary hypertension (PH) on outcomes after TAVI was evaluated in 2180 patients with moderate to severe PH in the Placement of Aortic Transcatheter Valves (PARTNER) I randomized study or registry (see page 1656). As with exercise and AF risk, sex differences were seen with an increased mortality hazard in women, but not men, with increasing degrees of PH. On multivariable analysis, clinical factors contributed more than hemodynamics indices to mortality risk after TAVI in these patients. The authors propose a multivariable risk score that separates patients with moderate-severe PH into a group with a 15% versus 59% 1-year mortality after TAVI. The key variables in this model are oxygen-dependent lung disease, inability to perform a 6 minute walk, impaired renal function and a lower aortic valve mean gradient. These data emphasize the need to focus on clinical factors, not just hemodynamics measures, in evaluation of patients being considered for TAVI.
In the Education in Heart article in this issue (see page 1678). Luyckx and Loeys review the genetic conditions associated with an increased risk of thoracic aortic aneurysm. The lucid text and clear illustrations provide a concise update for clinicians and will assist each of us in recognizing these conditions in our patients with aortic dilation of any cause.
The Image Challenge case is quite interesting, asking us to use the coronary angiogram to decide on the next step in management of a 42 year old women who collapses in a park (see page 1626). The angiographic findings for this rare diagnosis are classic and should be recognized by all cardiologists and trainees.
Linked Articles
- Editorial
- Editorial
- Valvular heart disease
- Arrhythmias and sudden death
- Coronary artery disease
- Education in Heart
- Editorial
- Review