Article Text

Statistics from Altmetric.com
The Editor's Choice in this issue of Heart is an important study by Bokma and colleagues. In this study they propose an approach to individualized prediction of pulmonary homograft durability based on data from 1523 tetralogy of Fallot patients who had undergone pulmonic valve replacement (PVR) surgery (at age ≥12 years) (see page 1717). Average freedom from homograft dysfunction was 74% at 10 years (figure 1) with multivariable analysis identifying 3 independent risk factors for homograft dysfunction: an early post-operative PVR gradient ≥20 mm Hg, any degree of pulmonic regurgitation, and surgery at age <18 years. In those with no risk factors, freedom from graft deterioration was 91% at 10 years compared to 25% with those with 2 or 3 risk factors.

Homograft dysfunction and reintervention after PVR. Kaplan–Meier curves displaying freedom from homograft dysfunction (pulmonary stenosis ≥36 mm Hg or moderate pulmonary regurgitation) and freedom from homograft reintervention (redo-PVR, Melody implantation or balloon dilation of homograft) after PVR. PVR, pulmonary valve replacement.
The editorial by Heng, Gatzoulis and Babu-Narayan provides insight into how these findings might change clinical practice (see page 1695). “The risk model presented may aid in appropriately intensifying the frequency and spacing of post-PVR follow-up, particularly in adolescent tetralogy patients with evidence of homograft stenosis or regurgitation. Counselling individual patients about their own relative timeframes for redo-PVR may be better informed by these data.” However, “when making inferences from this study's results, its generalisability should be interpreted with caution” and “much larger scale prospective work addressing the relative durability of different surgical conduit choices is still warranted.”
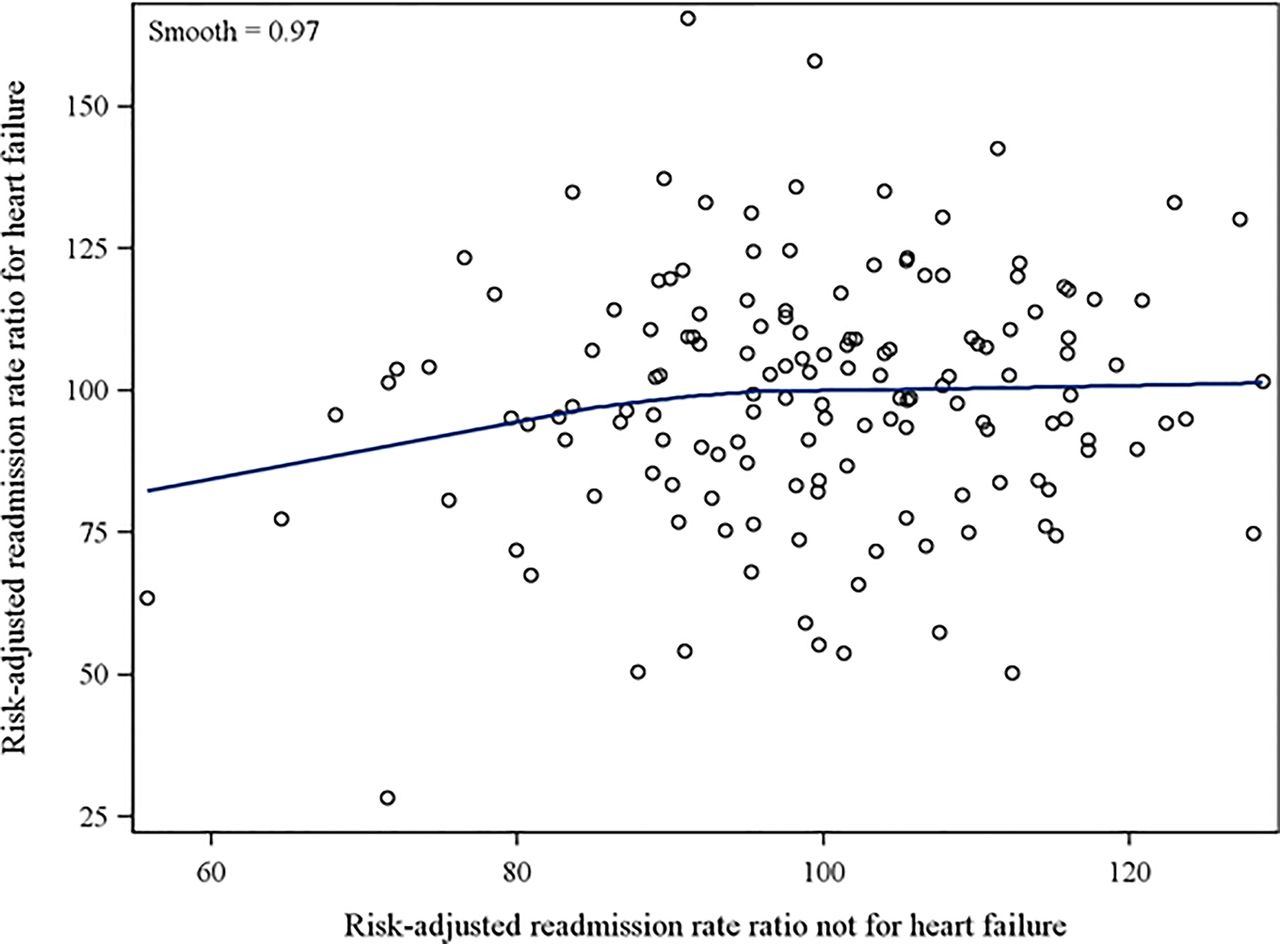
In patients presenting with a new diagnosis of heart failure (HF), hospital readmission rates at 30-days have been used as a measure of the quality of health care delivery, particularly in the USA. However, previous American studies have shown variable results for interventions that attempt to reduce all cause readmission rates. The key process measures studied include treatment with angiotensin converting enzyme inhibitor and beta-blocker medications, diagnostic echocardiography, cardiology consultation, and outpatient cardiology and HF liaison followup. Bottle and colleagues (see page 1704) studied the relationship between these process measures and diagnosis-specific readmission rates in heart failure patients for all acute care hospitals in England over a 3-year period. In these 123,644 patients, mortality during the index hospitalization was 14.7%, with an emergency readmission rate of 6.5% at 7 days and 19.1% at 30 days. Key process measures correlated significantly, but only modestly, with HF readmission rates with a declining effect of these measures over longer followup intervals. In addition, rehospitalization for non-HF causes was common with HF accounting for the emergency readmission in only 1 of 3 patients at 7 days and in only 1 of 5 patients at one year (figure 2). Thus, readmission rates were not just due to recurrent HF but were related to a high prevalence of comorbidities in these HF patients, of whom 88% were aged ≥65 years.

Scatter plot of 30-day heart failure (HF) versus non-HF readmission risk-adjusted rate ratios, all hospitals, with superimposed local smoother.
As DeVore and Hernandez (see page 1691) elegantly expound, these data “suggest that improving outcomes is much harder than checking a box. In other words, the process-outcome link in hospitalised heart failure is complex and there are myriad of decisions or processes of care that go into a patient's outcome”. “Moving forward, there is a greater possibility to improve care through learning healthcare systems that continuously measure processes and outcomes and their associated links. Through the emergence of electronic health records, improved analytics of ‘big-data’, including machine learning, there is large potential to move beyond a few processes of care to improve the quality of heart failure care”.
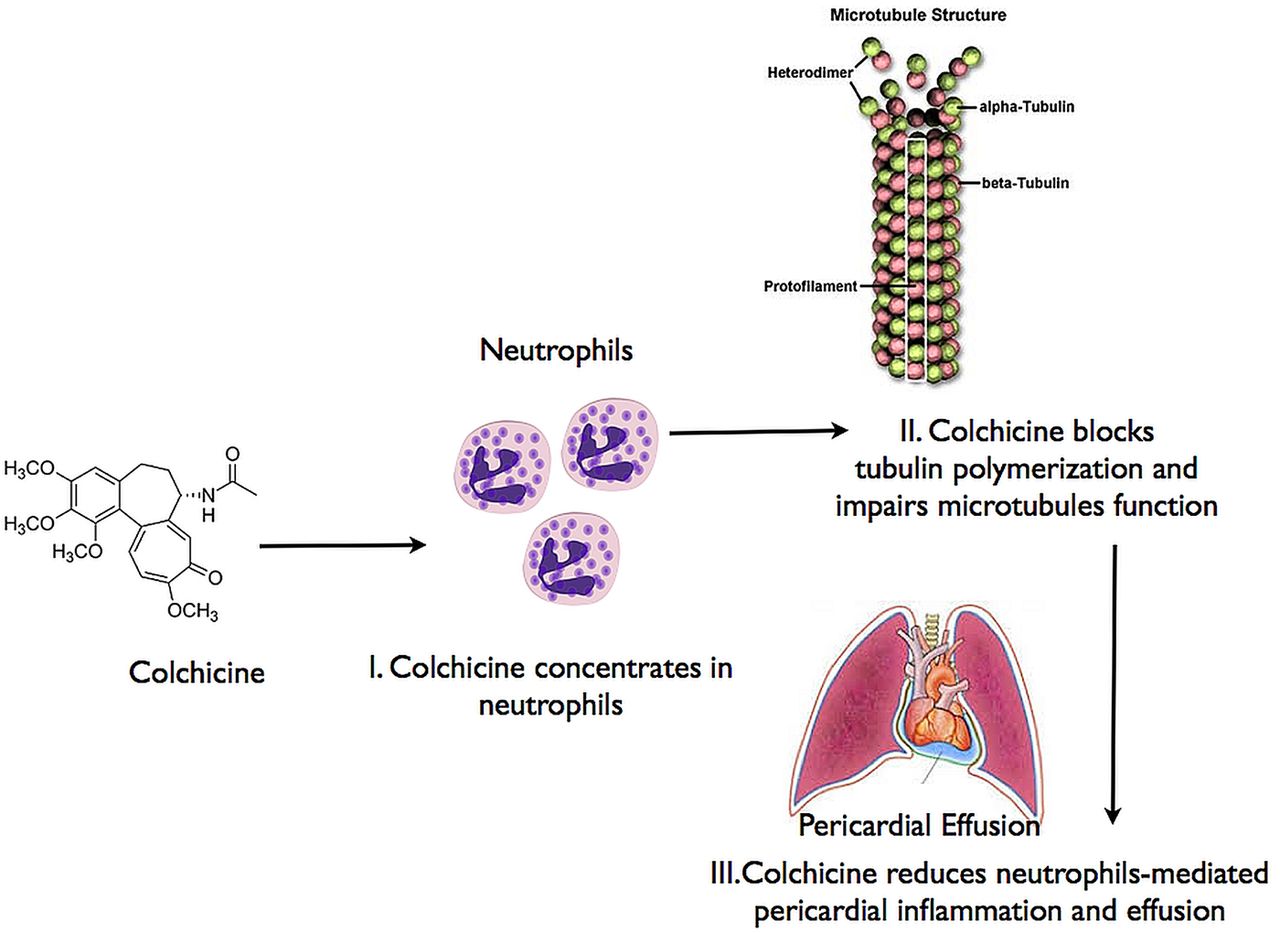
The management of post-operative pericardial effusions remains controversial. Meurin and colleagues (see page 1711) performed a randomized clinical trial of colchicine (1 mg daily) compared to placebo in 197 patients with a moderate to large-sized pericardial effusion on echocardiography at 7 to 30 days after cardiac surgery. There was no difference between treatment groups in baseline effusion size, the change in effusion size, or the occurrence of cardiac tamponade (in 6.6%) over the 14-day treatment period and no difference in the need for pericardial drainage (in 11%) at 6 months. Prespecified subgroups defined by baseline C-reactive protein (CRP) levels or anticoagulant treatment also showed similar outcomes regardless of treatment group (table 1).
Change in pericardial effusion grade** in prespecified subgroups
In an editorial accompanying this article, Imazio and Gaita (see page 1693) remind us that colchicine is effective for inflammatory causes of pericardial effusion (figure 3). However, postoperative pericardial effusions often are related to pericardial bleeding and increased filling pressures, rather than inflammation. They conclude: “At present, there is no reason to use colchicine to treat postoperative effusions in the absence of pericarditis, post-pericardiotomy syndrome or systemic inflammation, as for other non-steroidal anti-inflammatory drugs”.
{kind=link}
{kind=link}
{kind=link}
Main known mechanism of action of colchicine to treat and prevent pericardial effusions.
The Education in Heart article in this issue (see page 1755) summarizes the biology of the vulnerable atherosclerotic plaque including a review of current clinical diagnostic approaches and a discussion of potential new therapeutic targets.
Challenge yourself to interpret pressure tracings in a patient with a moderate pericardial effusion in this week's Image Challenge case (see page 1703). Some of our readers disagree with the diagnosis and have already sent their comments in the correspondence section. What do you think?
Linked Articles
- Education in Heart
- Editorial
- Editorial
- Special populations
- Congenital heart disease
- Editorial
- Image challenge
- Heart failure and cardiomyopathies