Article Text

Statistics from Altmetric.com
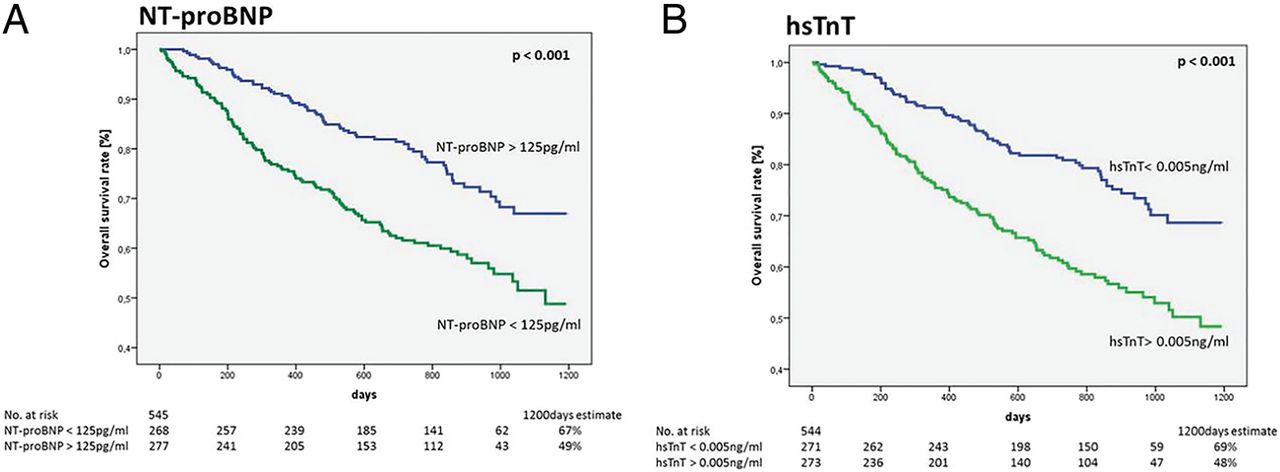
The cardiotoxic effects of some chemotherapeutic regimens are well known and we all recognize the need for periodic cardiac monitoring in patients receiving these agents. The possibility of subclinical myocardial damage associated with cancer itself is less well established. In this issue of Heart (see page 1874), a study by Pavo and colleagues of 555 consecutive oncology patients demonstrated that elevated circulating levels of cardiovascular peptides were present prior to the start of any cancer therapy. In addition, they report the important novel finding that elevated cardiovascular peptide levels were significant predictor of all-cause mortality (34%) at median followup of 25 months. Biomarkers that were independently predictive of mortality included N-terminal pro-B-type natriuretic peptide (HR 1.54, IQR 1.24–1.90), mid-regional pro-adrenomedullin, C-terminal pro-endothelin-1, copeptin, and high sensitivity troponin T (HR 1.21, IQR 1.13–1.32) (figure 1).

Kaplan–Meier estimates of all-cause mortality for (A) N-terminal pro B-type natriuretic peptide (NT-proBNP) with a cut-off value of 125 pg/mL, and (D) hsTnT with a cut-off value of 0.005 ng/mL for patients with newly diagnosed tumour disease (p<0.001 between two groups for NT-proBNP and hsTnT, log-rank test).
In the accompanying editorial, Dr Lyon (see page 1853) points out that this provocative study raises other unanswered questions: Is the source of elevated biomarkers the heart and vasculature or the cancer itself? Is the mortality associated with elevated biomarkers related to cancer activity or cardiovascular disease? Even so, he concludes, “Pavo et al should be congratulated on bringing to our attention the widening complexity of biomarker biology and the potential to identify single biomarkers with the unique properties to predict both cardiovascular and oncology outcomes.
In a prospective multicenter Korean registry (see page 1881) of 1665 patient presenting with acute heart failure (HF), the prognostic value of plasma levels of N-terminal–pro-brain natriuretic peptide (NT-proBNP) in patients with heart failure with reduced ejection fraction (HFrEF) was compared to patients with HF and preserved EF (HFpEF). Although HFpEF patients had lower NT-proBNP levels than HFrEF patients, there was no difference in event free survival (88.4% vs 86.9%; p=0.471) with a similar prognosis for patients a given NT-proBNP level, regardless of ejection fraction.⇓
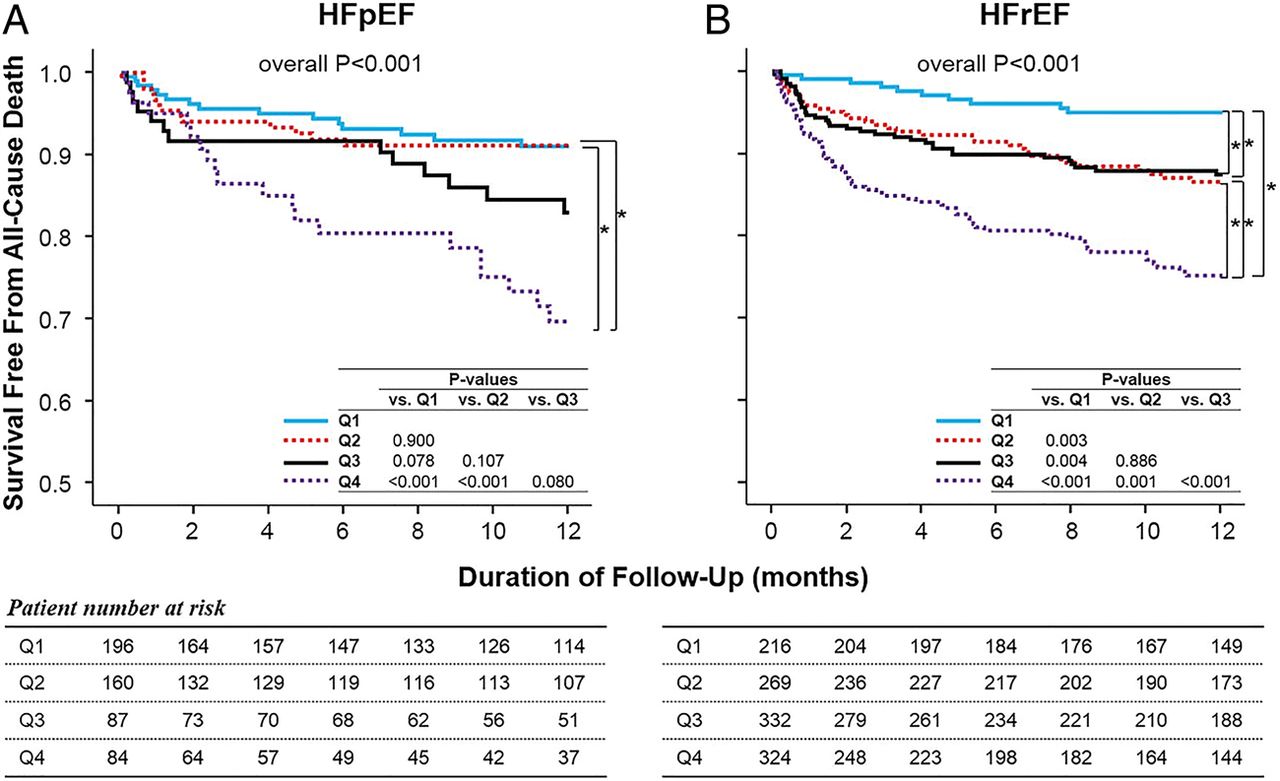
Kaplan–Meier survival curves free from all-cause death in patients according to quartiles of plasma NT-proBNP with (A) heart failure with preserved EF (HFpEF) and in patients with (B) heart failure with reduced EF (HFrEF). p Values are described for each pairwise comparison.
In an editorial, Bosseau, Galli and Donal (see page 1855) point out that the role of natriuretic peptide (NP) level monitoring in management of HF patients remains in flux because there is significant variation in NP levels, the optimal target value remains unknown, and the impact of reducing NP levels on clinical outcomes is not certain. However, the data from the Korean registry do suggest that using NP levels as part of the management strategy is appropriate not only for HFrEF but also in patients with HFpEF (figure 3).

{kind=link}
{kind=link}
{kind=link}
Proposed use of N-terminal-pro B-type natriuretic peptide measurements in the management of patients with heart failure (HF) hospitalised for acute decompensation. LV, left ventricular; NYHA, New York Heart Association.
It is well-known that there is a significant association between lower education level and higher cardiovascular disease (CVD) mortality. Data from a Norwegian cohort of almost 35 thousand adults confirms this association with a sex-adjusted CVD mortality hazard ratio of 2.32 (95% CI 1.93 to 2.80) for the lowest versus highest educational level (see page 1889). However, it has not been established whether this association is due to conventional cardiovascular risk factors or to some other effect of educational level. In this study, adjustment for baseline CVD risk factors reduced the effects of educational level by 48%. Further, when adjusted for repeated risk factor assessment at an interval of 5 years, the effect of educational level was attenuated by 56%, suggesting that a much of the apparent difference simply is due to differences in conventional risk factors. (Table 1).
Risk of cardiovascular disease (CVD) mortality by educational level with adjustment for baseline and repeated measurements of risk factors
In the accompanying editorial, Darden and Berry (see page 1859) discuss the importance of considering the long-term risk of CVD over the patient's lifetime, rather than just short-term (eg 10 year) risk. As the study by Ariansen and colleagues shows, risk factors tend to be relatively stable over time, with a slight decrease in smoking and a gradual increase in blood pressure and cholesterol in patients evenly across the range of educational levels. Darden and Berry conclude: “preventing CVD reflects more what our patients are doing in their 20s than what medications they are taking when they are 50”. “While some of the risk can be modified in middle-age adults, a portion of it cannot, and therefore, for many, it's water under the bridge”.
The Education in Heart article in this issue focuses on patent foramen ovale (PFO) in adults (see page 1916). This comprehensive article reviews the anatomy of the atrial septum, notes that 25% of us have a PFO, and illustrates the diagnostic approach with saline contrast or trans-oesophageal echocardiography. The association between PFO and embolic events is discussed in detail with a concise summary of the 3 randomized trials of PFO closure for prevention of recurrent stroke. All of these trials were negative but were limited by slow recruitment, high rates of off-label device use, and variability in PFO and atrial septal anatomy among the patient populations. Recent longer followup data from one study suggest there might be benefit, indicating that further studies of PFO closure for prevention of recurrent stroke are needed.
Linked Articles
- Cardiac risk factors and prevention
- Editorial
- Heart failure and cardiomyopathies
- Editorial
- Heart failure and cardiomyopathies
- Editorial
- Education in Heart