Article Text

Statistics from Altmetric.com
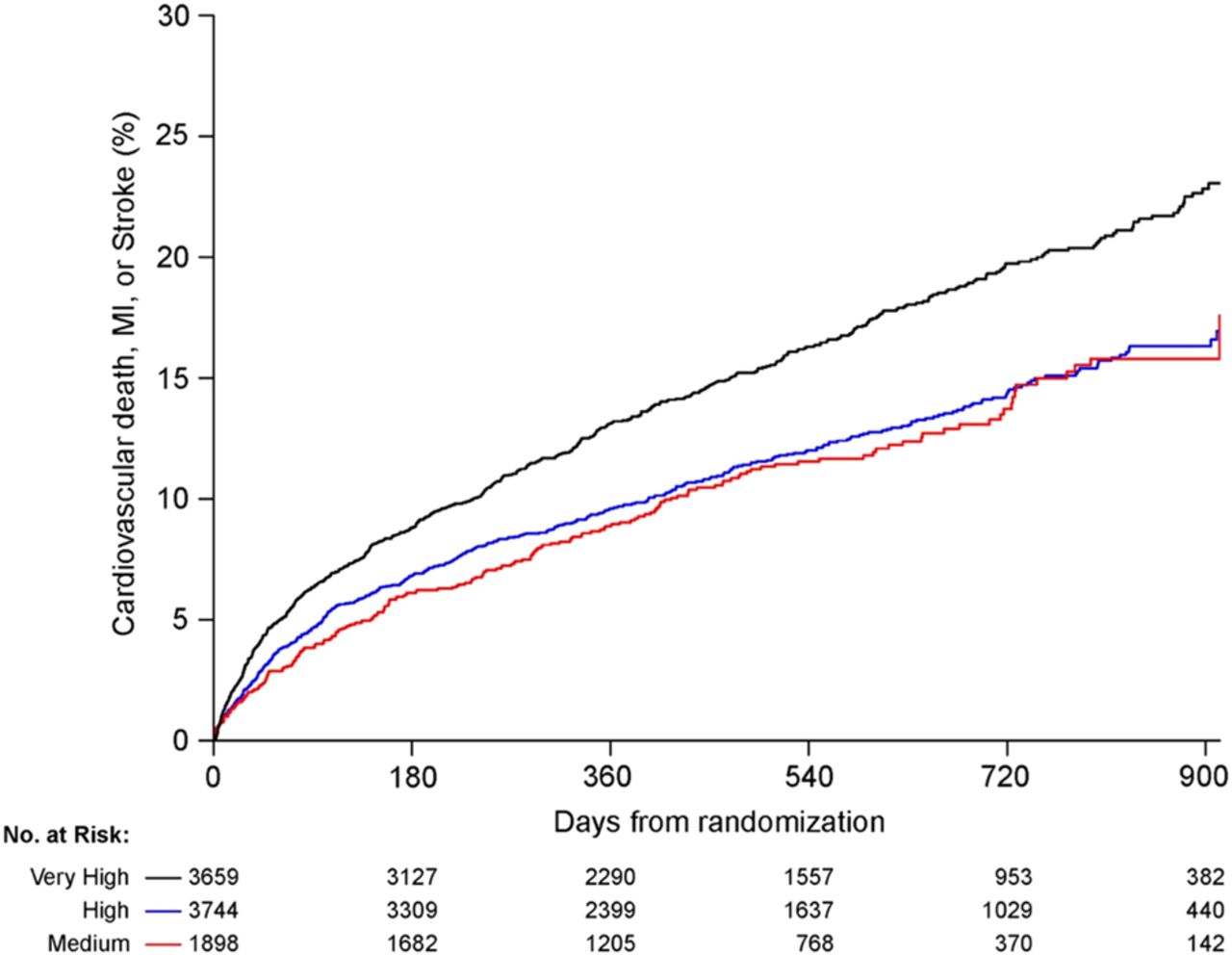
Randomized controlled trials increasingly recruit patients globally to facilitate recruitment and to improve validity and applicability. However, patients from countries with different developmental status may differ in terms of clinical profiles, adherence to prescribed therapy and access to health care facilities. Further, these differences may impact patient outcomes. In this issue of Heart Professor Prabhakaran and colleagues (see page 279) (figure 1) report the influence of developmental status of individual countries, as defined by the United Nations' Human Development Index (HDI), on clinical outcomes of patients with Acute Coronary Syndrome (ACS) in a multinational study, the Trilogy ACS. Despite uniform study eligibility criteria, baseline characteristics differed significantly among patients from different HDI-classified countries. These baseline differences in turn were associated with differential outcomes. The authors conclude that geographical and other country-level factors variations in study populations need to be taken into account when designing, conducting and analyzing trials.
In the companion editorial, Dr Banerjee (see page 245) systematizes how this heterogeneity in developmental status can influence both internal and external validity of a clinical trial. He also opens the discussion to a much broader ethical issue: what is the role of testing new, expensive drugs in countries with low developmental status, where access to other proven and low-cost therapies is frequently absent? (figure 2).
Air pollution is associated with higher rates of cardiovascular morbidity and mortality. In a study from Beijing by Professor Lui and colleagues (see page 257), a clear dose-response relationship between the air concentration of fine particulate matter (PM2.5) and ischemic heart disease mortality was demonstrated over a 2 year period based in a very large ischemic heart disease database. The authors conclude: “Our findings provide a rationale for the urgent need for stringent control of air pollution to reduce PM2.5 concentration” (figure 3).
Dr Pope comments in an editorial (see page 248) that “cohort and related studies that evaluate effects of long-term exposure are also needed to help provide a more complete understanding regarding the shape of the exposure–response relationships across the full range of exposures, including highly polluted areas of the world”. Dr Mike Chin addresses the basic mechanisms for the adverse cardiovascular effects associated with air pollution in a comprehensive review article. (see page 253) Although the pathophysiologic perturbations are complex and incompletely understood, they do include pulmonary and systemic inflammation and increased oxidative stress, autonomic nervous system imbalance and the entry of inhaled toxicants into the circulation (figure 4).
The variation in clinical presentation and outcome in patients the same inherited cardiac condition, such as hypertrophic cardiomyopathy, has been puzzling. Now, the availability of high throughput genetic sequencing promises to help us pinpoint the relationship between a specific genotype and the clinical phenotype. In turn, this information should result in better patient outcomes as we target therapy to individuals at high risk of specific adverse events. In a study of 874 hypertrophic cardiomyopathy patients, Professor Elliott and colleagues (see page 294) found a sarcomere protein variant in 43.5% with ANK2 variants associated with the greatest left ventricular wall thickness. Patients with an identifiable sarcomere protein variant (compared to those without) were younger, had greater increases in LV wall thickness, more often had a family history of hypertrophic cardiomyopathy or sudden cardiac death, and had a higher incidence of cardiovascular death. These findings illustrate how genetics can inform clinical care and point the way to future studies of genotype-phenotype correlations in other cardiac conditions.⇓⇓⇓⇓

Cumulative Kaplan–Meier failure estimates of the composite study endpoint by Human Development Index (HDI) classification during the 30-month follow-up period. Black, very-high HDI; blue, high HDI; red, medium HDI.

From populations to trials and trials to populations.
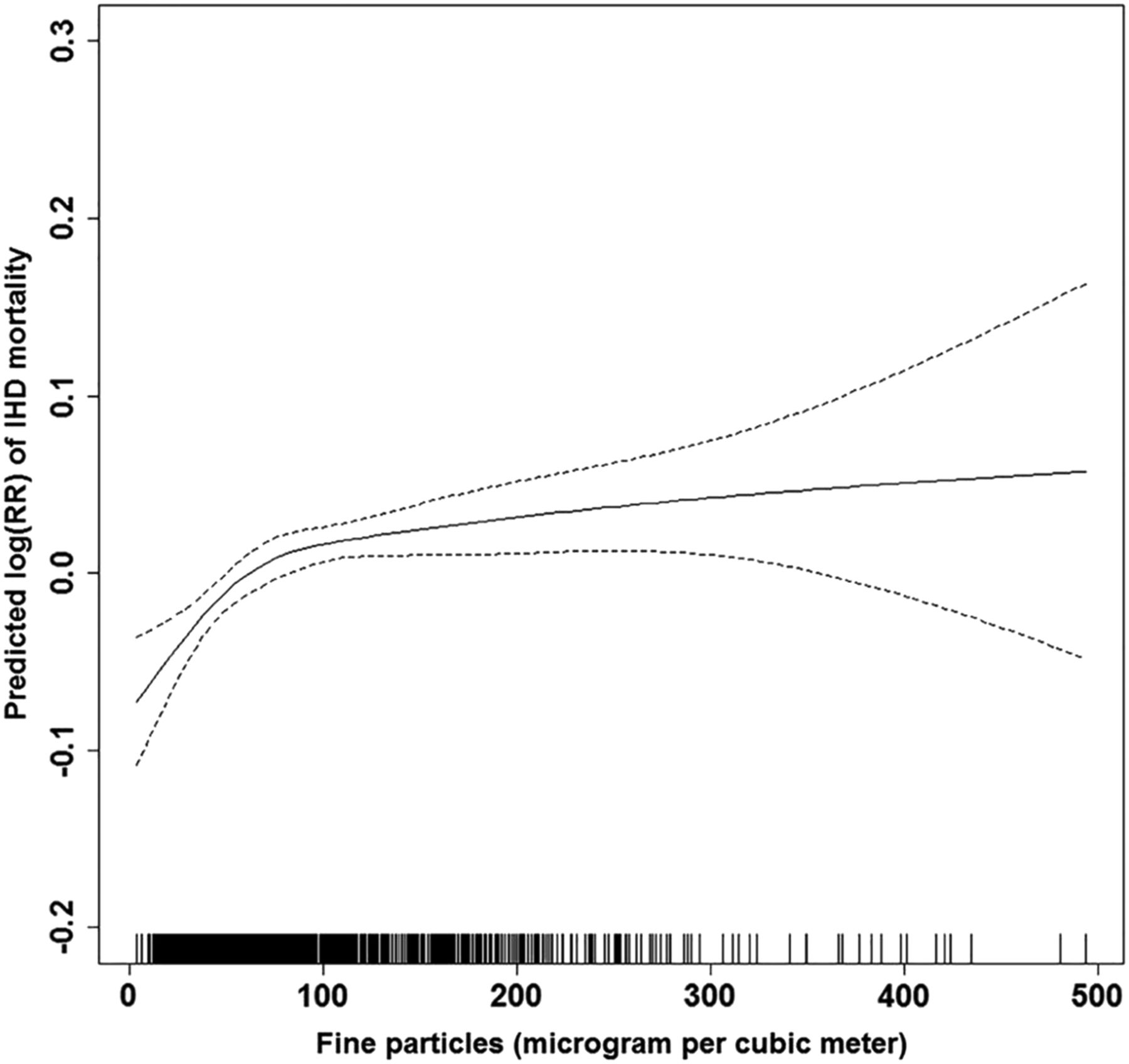
Smoothed plots of concentration of fine particles (degree of freedom=3) against the risk of mortality from ischaemic heart disease (IHD). The X-axis is the current-day (lag 0 day) fine particulate matter (PM2.5) concentrations (µg/m3). Y-axis is the predicted log (relative risk (RR)), after adjusting for calendar time, day of the week, current-day temperature, and dew-point temperature, is shown by the solid line, and the dotted lines represent the 95% CI.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
A working model of how air pollution exposure promotes adverse cardiovascular effects.
The Education in Heart article (see page 311) in this issue discusses primary pulmonary hypertension (PH). As cardiologists, we often see patients with Type 2 PH due to left heart disease, caused by chronically elevated left atrial pressure and an initially passive increase in pulmonary vascular resistance. In contrast, pulmonary arterial hypertension (PAH< Type 1 PH) “is characterised by intrinsic pathological changes in the afferent and capillary pulmonary vasculature that are not present in the other PH groups.” The etiologies of PAH include idiopathic, genetic, drug or toxin induced and those associated with a systemic disease. This review provides a practical and detailed approach to diagnosis and management including flow-charts
Our Image Challenge case (see page 329) asks you to identify the cause of blackouts in a young woman based on the clinical presentation and ECG findings on a loop recorder during a clinical episode.
Linked Articles
- Education in Heart
- Editorial
- Editorial
- Image challenge
- Healthcare delivery, economics and global health
- Heart failure and cardiomyopathies
- Review
- Cardiac risk factors and prevention