Article Text

Statistics from Altmetric.com
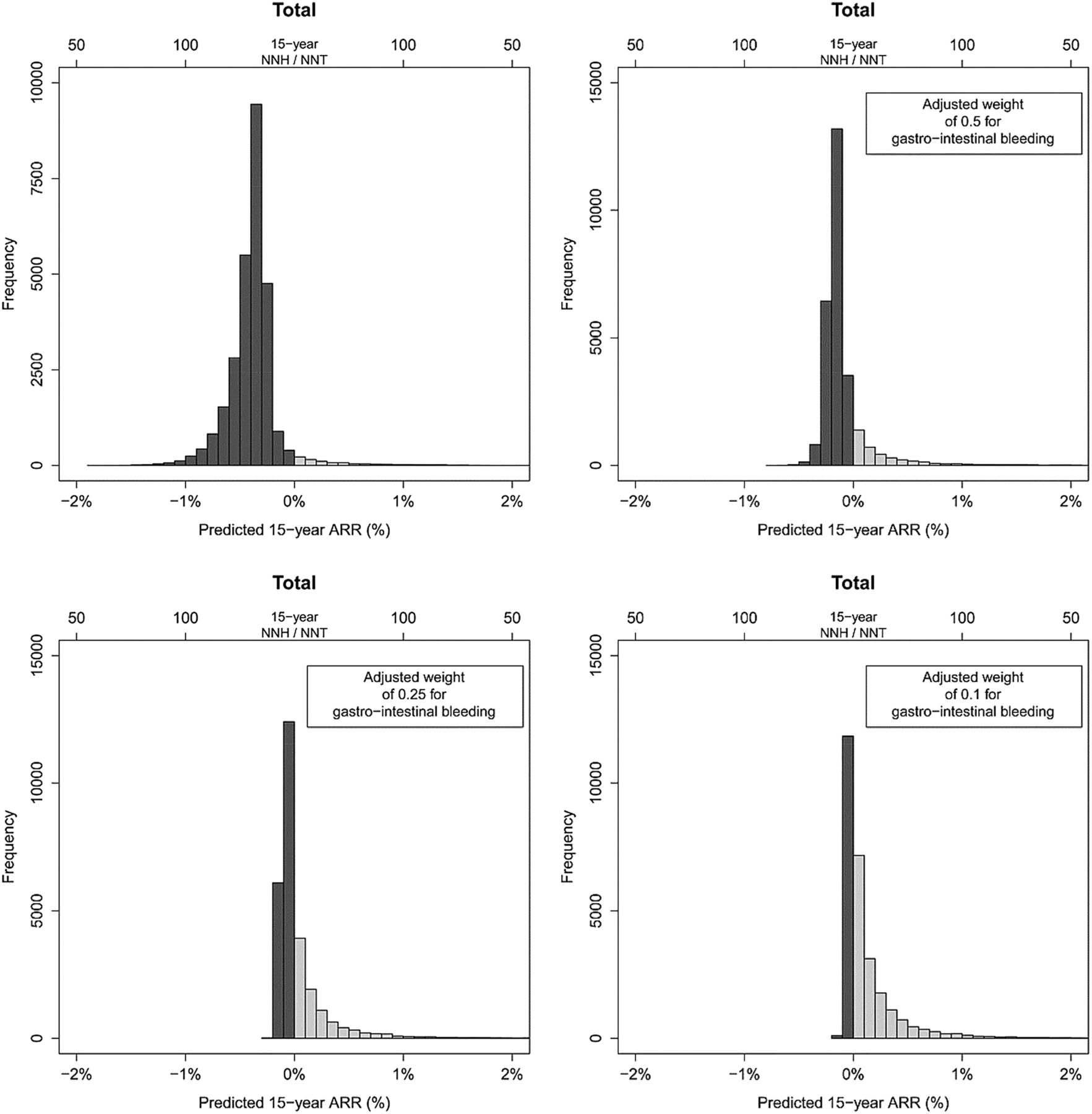
As cardiologists, we tend to consider the potential benefit of aspirin therapy in preventing cardiovascular disease (CVD), balanced against the risk of bleedings events. However, alternate day aspirin also may have a role in primary prevention of cancer and the combined benefit of cancer and CVD prevention is a more relevant metric than either outcome alone. To address the risk-benefit of primary prevention with aspirin in women, Dr. Visseren and colleagues (see page 369) developed a competing risks model based on outcomes in over 27 thousand healthy women in the Women's Health Study (WHS) randomized to 100 mg aspirin or placebo on alternate days. Overall, aspirin therapy had a negative effect on outcomes with an increased risk of gastrointestinal bleeding, despite a modest reduction in CVD and colorectal cancer over 15 years of followup. However, selective treatment of women 65 years of age and older may provide net benefit with an estimated number needed to treat of 29 (95% CI 12 to 102) to prevent one event over 15 years (figure 1).

Distribution of predicted 15-year ARR for the total of all outcomes (major cardiovascular events, colorectal cancer, non-colorectal cancer, and major gastrointestinal bleeding) applying different weights for gastrointestinal bleeding, in participants in the Women's Health Study. ARR, absolute risk reduction; NNT/NNH, number needed to treat/harm.
In the accompanying editorial (see page 335), Professors Ferrario and Veronesi conclude that “when balancing combined long-period ASA benefits on CVD and cancer with its harmful effects, taking into account the individual risk profile for each investigated outcome, these WHS results support no treatment indications with alternate-day low-dose aspirin in healthy women.” They also suggest that improved approaches to risk assessment are needed because: “In women aged 65 years or more, the question becomes whether it is meaningful to treat more than 32 healthy subjects for 15 years at least in order to prevent one combined event during the same time span.”
The goal of translating basic science advances in cell-based therapy for myocardial dysfunction into clinically meaningful improvements in clinical outcomes has been elusive. In the HEBE study, 200 patients with a large first myocardial infraction were randomized to infusion of bone marrow mononuclear cells (BMMCs), peripheral blood mononuclear cells (PBMCs) or standard therapy. In this issue of Heart, Dr. Delewi and colleagues (see page 363) report that cardiac magnetic resonance (CMR) imaging 5 years after the acute event showed a smaller increase in left ventricular (LV) end-diastolic volume index in the BMMC group (3.5±16.9 mL/m2) compared to standard therapy (11.2±19.8 mL/m2, p=0.03). In addition, the combined clinical endpoint of death or hospitalization for recurrent myocardial infarction was not significantly different for the BMMC group compared to standard therapy, although it was higher in the PBMC group (14 patients vs 3 patients, p=0.008). The authors conclude that this data supports the long-term safety of BMMC infusion but that a larger trial is needed to evaluate efficacy.
Professor Kai Wollert (see page 337) notes that “BMMC trial results have been heterogeneous, and the overall effect of BMMCs on LV ejection fraction appears to be rather modest. Still, the available trial evidence appears to provide a signal of therapeutic efficacy and it may be imprudent to disregard this indication.” He suggests we watch for the results of a pan-European phase III trial “that will explore the impact of autologous BMMCs on all-cause mortality in 3000 patients with large STEMI (ClinicalTrials.gov identifier: NCT01569178).”
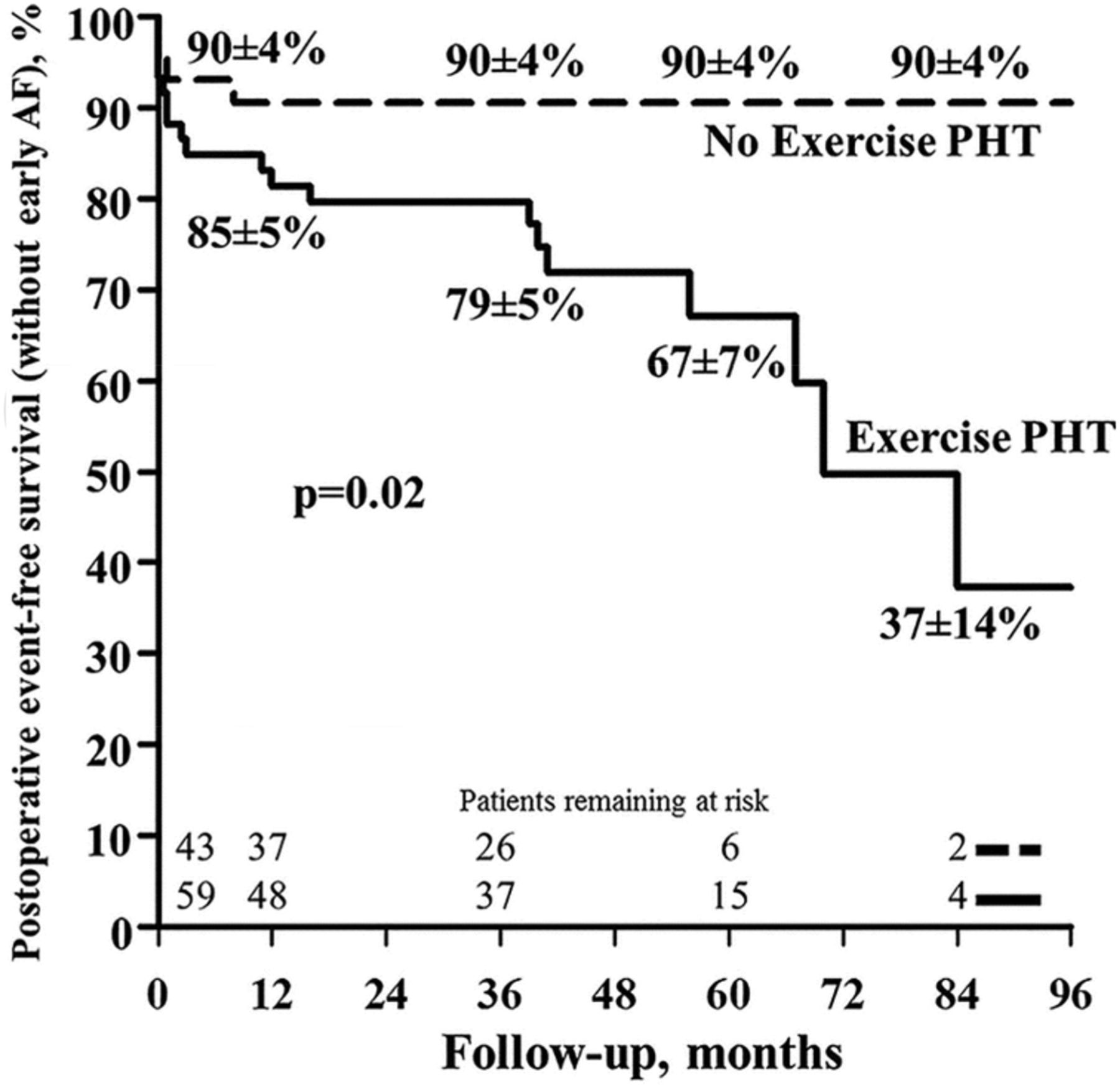
The initial symptoms in patients with chronic valvular heart disease typically occur with exertion so there has been continued interest in the role of stress testing to improve risk stratification. In particular, it has been hypothesized that pulmonary hypertension on exertion might predict outcomes after intervention in patients with chronic primary mitral regurgitation (MR). In study of 110 patients undergoing surgery for primary MR with baseline normal LV size and systolic function, DrMagne and colleagues (see page 391) found that the 59 patients with an exercise pulmonary systolic pressure over 60 mm Hg had more postoperative events, defined as atrial fibrillation, stroke, recurrent hospitalization or death. Exercise pulmonary hypertension remained independently associated with postoperative adverse events, even after accounting for group differences such as older age in the pulmonary hypertension patients (figure 2).

Postoperative event-free survival without early atrial fibrillation (AF) according to the presence or absence of exercise pulmonary hypertension (PHT). Percentages reported are the survival rates at 1-, 3-, 5-, and 7-year of follow-up.
Currently, the European Society of Cardiology 2012 Guidelines for Valvular Heart Disease indicate that mitral valve surgery may be considered in asymptomatic patients with severe primary MR, normal LV function and exertional pulmonary hypertension if there is a high likelihood of a durable surgical repair and a low surgical risk. Although the 2014 American guidelines do not include a separate recommendation related to pulmonary hypertension with exercise, those guidelines do indicate that mitral valve surgery should be considered in all patients with severe primary MR and normal LV systolic function who meet the surgical criteria above, even without the requirement for exercise measurement of pulmonary pressures. Drs. Jellis and Griffin provide a useful framework for the imaging approach to evaluation of MR with stress when appropriate (figure 3, see page 339).

{kind=link}
{kind=link}
{kind=link}
Suggested peak image acquisition protocol for exercise stress echocardiography in the evaluation of severe mitral regurgitation.
The Education in Heart article in this issue by Professor Bax (see page 397) discusses the role of fibrosis imaging in severe valvular heart disease. Key points are that pressure overload LV hypertrophy due to aortic stenosis is associated with more fibrosis than volume overload hypertrophy due to MR and that myocardial fibrosis is associated with poor clinical outcomes. Approaches for direct noninvasive imaging of fibrosis include contrast enhanced CMR, echocardiographic integrated backscatter, and molecular imaging. Indirect measures of myocardial fibrosis include strain and strain rate imaging by tissue Doppler, speckle tracking echocardiography or tagged CMR, as well as perfusion tissue fraction and index with positron emission tomography (PET).
Check out the interesting Doppler findings in the Image Challenge question (see page 390) and see the explanation of the answer in the online supplemental figures and videos. Be sure to go directly to the Heart website (heart.bmj.com) to see the full content of each article, including online supplements, as well as interesting podcasts, video abstracts and the most recent Journal Scan updates on our blog.
Linked Articles
- Cardiac risk factors and prevention
- Valvular heart disease
- Editorial
- Education in Heart
- Coronary artery disease
- Arrhythmias and sudden death
- Editorial
- Editorial