Article Text

Statistics from Altmetric.com
Patients with repaired tetralogy of Fallot (TOF) are increasingly seen in cardiology practice given the success of surgical repair procedures in infancy and childhood. However, many of these patients require reoperation in young adulthood for pulmonic valve regurgitation and they remain at increased risk of ventricular tachycardia and sudden death. In a study of 90 consecutive adults with repaired TOF, compared to 15 age and sex matched control subjects, an elevated serum brain natriuretic peptide (BNP) level was a strong predictor of death (HR 1.16 per 10 pmol/L, 95% CI 1.05 to 1.29; p<0.01). (see page 447). In TOF patients, a BNP≥15 pmol/L (=52 pg/mL) was associated with an absolute mortality of 19% at 5 years compared to 3% in those with a lower BNP level. Dr Babu-Narayan and colleagues conclude that neurohormonal activation in asymptomatic TOF patients should be incorporated into the routine longitudinal assessment of these patients Figure 1.
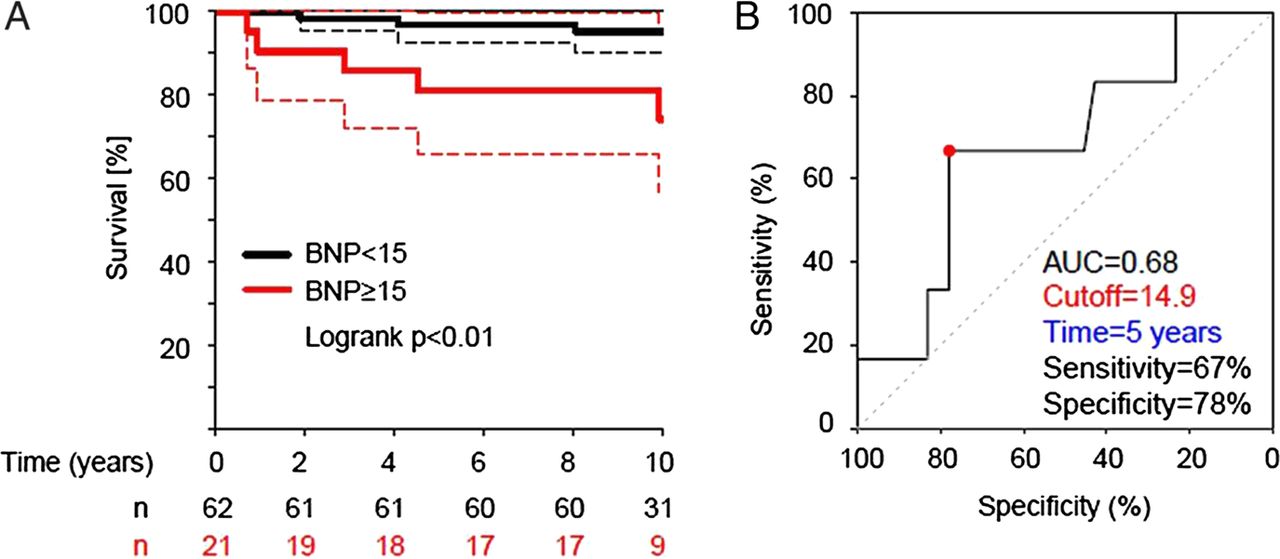
(A) Kaplan–Meier survival curve (dotted lines represent 95% CIs). (B) Receiver operating curve survival analysis for brain natriuretic peptide (BNP) (AUC, area under the curve).
In an editorial, Dr Giannakoulas and colleagues (see page 416) comment that there are several reasons for an elevated BNP in TOF patients including progressive right ventricular (RV) dilation due to pulmonic regurgitation, residual RV outflow obstruction, left ventricular (LV) systolic dysfunction and aortic regurgitation. In addition, about 20% of TOF patients develop atrial arrhythmias, which also are associated with elevated BNP levels. They recommend: “Until data from future studies become available, we should not use BNP as a stand-alone test, but rather continue applying a comprehensive approach in the risk stratification and management of these patients.”
In adults with severe aortic stenosis (AS), concurrent LV systolic dysfunction connotes a poor prognosis, even with aortic valve replacement (AVR), and many of these patients have a high or prohibitive risk for surgery. In an analysis from Cohort B of the Placement of AoRtic TraNscathetER Valves (PARTNER) trial (see page 463), Dr Passeri and colleagues found that a baseline LV ejection fraction <50% (but >20%) did not affect survival after TAVR but was associated with increased cardiac mortality at one year in patients randomized to standard therapy. An absolute increase in LV ejection fraction was seen in only 30.4% of standard therapy patients compared to 48.7% of TAVR patients (p=0.08). Even if LV ejection fraction increased with standard therapy, mortality at 2 years was not improved. The authors conclude that TAVR improves survival in inoperable patients with severe AS and an LV ejection fraction >20% figure 2.⇓

LV functional recovery over time in subjects undergoing standard therapy (A) and transcatheter aortic valve replacement (B).
A study in this issue of Heart suggests that complications of pregnancy be considered in the assessment of the risk for atherosclerotic disease in women. (see page 442) Hypertensive disorders of pregnancy, including pre-eclampsia, are associated with an increased risk of cardiovascular (CV) disease later in life but the association between pre-eclampsia and generalized atherosclerotic disease, including renal as well as CV morbidity, has received less attention. In a population-based study of a cohort of over 96 thousand women followed for a mean of 11.2 years, 8.1% had at least one episode of pre-eclampsia. Pre-eclampsia was associated with an increased risk of complex CV events (OR 2.4; 95% CI 2.2 to 2.8; p=0.001) and renal hospitalisations (OR 3.7; 95% CI 2.2 to 6.0; p=0.001). There also was a “dose–response” association for the risk of future atherosclerotic disease with both the severity and number of episodes of pre-eclampsia and this association remained evident after adjustment for cofounding variables. These findings suggest that more intense surveillance and lifestyle changes may be appropriate in women who experience pre-eclampsia during pregnancy figure 3.⇓⇓

Cumulative incidence of cardiovascular (CV) (A) and renal hospitalisations (B).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Algorithm for assessment of patients with cyanotic congenital heart disease.
Another article addressing cardiovascular disease in pregnancy in this issue is a review by Drs Nishimura and Warnes summarizing the evidence underlying the current recommendations for anticoagulation during pregnancy for women with mechanical prosthetic heart valves. (see page 430) The optimal approach in these patients remains controversial and there continues to be a high rate of adverse maternal and fetal outcomes in this patient group. In this review, practitioners can find a concise summary of the key clinical issues and a list of current recommendations, as well as a detailed table of the published evidence.
Anticoagulation in adults with congenital heart disease is addressed in a detailed review article (see page 424) by Dr Jensen and colleagues, which summarizes our current evidence base. This article also suggests a practical clinical approach, matching the level of anticoagulation to an individualized assessment of thromboembolic risk, ranging from full dose vitamin K antagonist therapy to maintain a therapeutic INR in the patient with a mechanical valve to no therapy in patients with mild valve disease who are in normal sinus rhythm.
In an accompanying editorial (see page 418) Drs Faircloth, Palumbo and Veldtman applaud “this rational, but not yet evidence-based recommendation of anticoagulation only for individuals with risk factors additional to their baseline cyanotic heart disease. These include mechanical prostheses, atrial dysrhythmia, endovascular pacemakers and an elevated CHA2D2-VASc score.” However, they caution that “this review emphasises the need for a larger-scale consensus statement, as well as the crucial need for large clinical trials of existing and emerging anticoagulation strategies.”
The Education in Heart article by Dr Oechslin in this issue focuses on management of adults with cyanotic congenital heart disease (see page 485) including a useful algorithm for patient assessment figure 4.
Try the Image Challenge (see page 484) to make an unusual Doppler echocardiographic diagnosis.
Linked Articles
- Congenital heart disease
- Education in Heart
- Image challenge
- Review
- Editorial
- Review
- Editorial
- Valvular heart disease
- Cardiac risk factors and prevention