Article Text

Abstract
Introduction Primary PCI studies report 3-year mortality rates of 6–7%, but typically lack external validity or are from historical cohorts. To date, no long-term outcome study has accounted for factors other than primary PCI and variables identified at baseline. This is important because long-term survival is more likely to be influenced by factors not associated with the underlying disease or its early management.
In the United Kingdom, continuous whole country PCI data are collected through the British Cardiovascular Intervention Society registry and deaths via the Office for National Statistics, providing a unique opportunity to undertake large scale phenotype and intervention-specific research. In order to address the limitations of previous studies, we utilised the UK national cardiovascular and population databases to report relative survival (RS) and excess mortality after PPCI.
Methods All individuals in England and Wales with STEMI who received PPCI between 1st January 2005 and 31st December 2010 were matched by age, sex, year of procedure and country to English and Welsh population data. Estimates of cumulative relative survival rates (RSRs) and hazard rates were used to calculate expected survival, observed all-cause mortality rate ratios (MRR) and excess mortality rate ratios (EMRR). Crude RS was estimated using the Ederer II method for the whole cohort and cumulative RS estimated by age, sex and biennial year of procedure.
Results There was a total of 50,181 STEMI treated by PPCI from 109 hospitals, (mean age (SD) 63.2 (13.1) years, 25.9% female, (total time at risk 94997.5 person years). 6 month, 1 and 5 year RSRs were 93.1%, 92.6% and 90.9% and approached the background rate for patients <55 years (Figure 1 a and b). There was a temporal trend towards better outcomes (Figure 2). Excess mortality was evident for females and the elderly (Table 1).
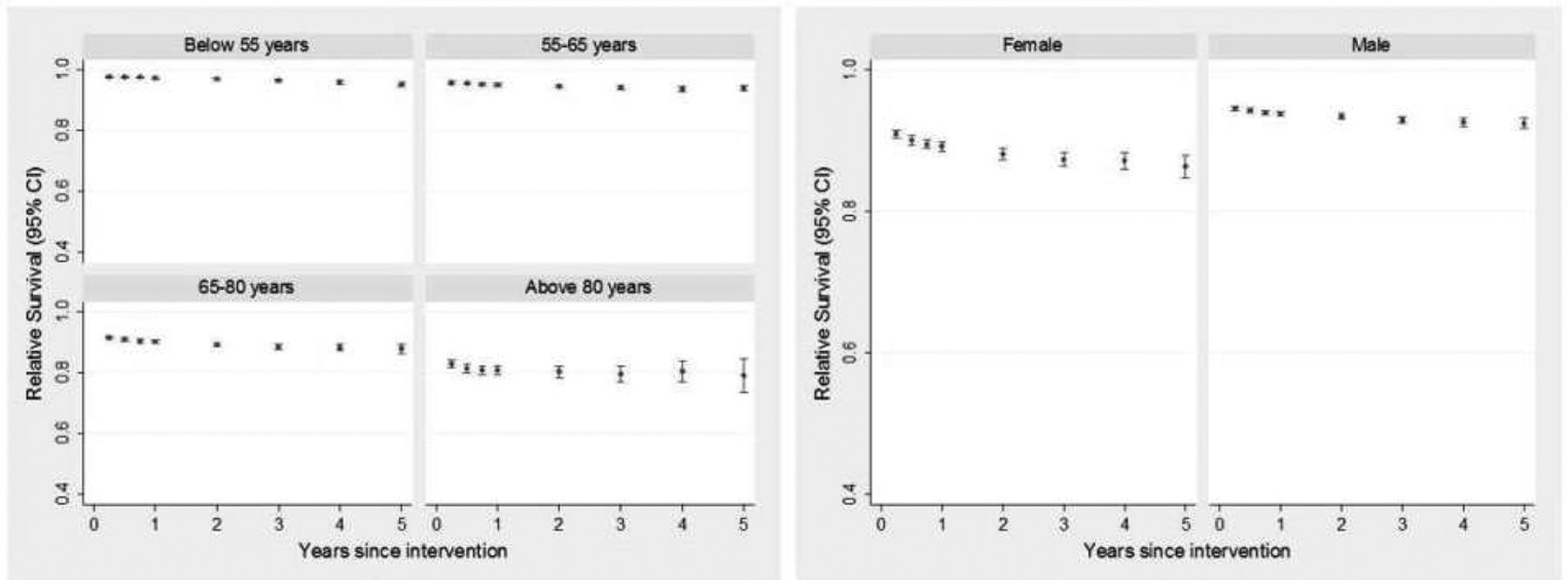
Five year cumulative relative survival stratified by (a) age and (b) gender

{kind=link}
{kind=link}
Five year relative survival stratified by calendar year
Excess mortality and observed all cause mortality rate ratios stratified by age, sex and calendar year (baseline model), 95% confidence intervals with interaction term
Conclusions Survival is excellent for young STEMI who receive PPCI. This study highlights long term excess mortality in the elderly and females who could be further stratified for existing and novel therapies to improve cardiovascular outcomes. Relative survival is an accurate, powerful and underused tool that may help identify opportunities to improve longer term cardiovascular outcomes.
- Survival
- STEMI
- PPCI