Article Text

Abstract
Background Multivessel disease (MVD) is seen in ˜40% of ST-elevation Myocardial Infarctions (STEMI). Revascularisation strategy and chronic total occlusions affect clinical outcomes in MVD. However, there are no published multivariate data on additional predictors of clinical outcomes in patients with MVD undergoing PPCI. We aimed to provide a comprehensive multimodal, multivariate assessment of independent predictors (clinical, bioanthropometric, angiographic and cardiovascular magnetic resonance [CMR]) of medium-term severe left ventricular systolic dysfunction (LVSD) and clinical outcomes in patients with MVD at PPCI.
Methods STEMI patients presenting <12 hr with MVD were prospectively enrolled. Multiparametric contrast-enhanced CMR was undertaken within 48 h of PPCI (‘Acute CMR’) and at 9 months (‘Follow-up CMR’) at 1.5T. LV volumetrics, strain, area-at-risk (AAR) and infarct characteristics were assessed on CMR using SSFP, Feature-Tracking, T2-weighted and late gadolinium imaging. Angiographic predictors included SYNTAX score, Rentrop grade and number of lesions >75% on Quantitative Coronary Angiography (QCA). The primary clinical outcome of 12-month combined MACE comprised all-cause mortality, recurrent MI, heart failure hospitalisation and ischaemia-driven revascularisation. Multivariate logistic regression and log-rank test (Cox regression) assessed independent predictors of severe LVSD (LVEF <35%) at 9-months, and 12-month combined MACE respectively.
Results (a) Severe LVSD (LVEF <35%) at 9-months
Univariate predictors of final LVEF <35% were anterior STEMI, diabetes, peak CK, time to revascularisation and SYNTAX score. Acute CMR predictors included wall-motion score (WMS), LV volumes, LVEF, infarct size (IS), AAR, extent of microvascular obstruction (MVO), myocardial salvage (MSI), and global strain. At stepwise multivariate regression, WMS was the only independent predictor of final LVEF <35%. ROC AUC was 0.965 and the optimal cut-off for predicting LVEF <35% was WMS ≥28 (Table 1).
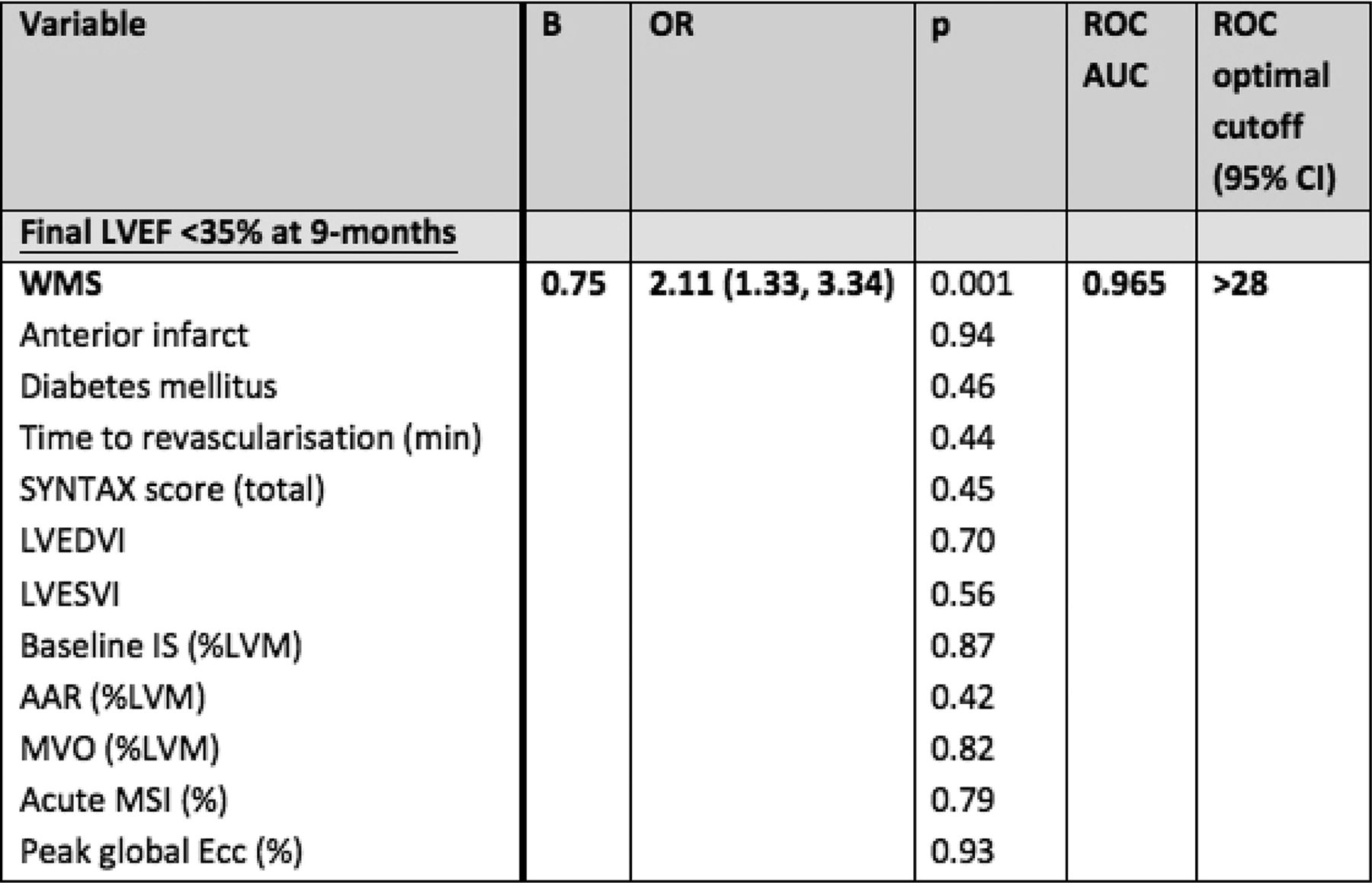
Multivariate predictors of final LVEF <35% at 9-months
(b) Combined MACE at 12-months
Univariate predictors of combined MACE at 12-months included age, peak CK, Rentrop grade, SYNTAX score, number of affected vessels and lesions >75% stenosis on QCA. Acute CMR predictors included WMS, LVEF, LV volumes, IS, AAR, MVO, MSI and global strain. At stepwise multivariate regression, IS at acute CMR was the strongest independent predictor, followed by number of lesions >75% severity on QCA, and revascularisation strategy. AUC for IS was 0.729 and the optimal cut-off for predicting MACE was IS≥16.8% LVM (Table 2).

{kind=link}
{kind=link}
Multivariate predictors of combined first MACE at 12-months
Conclusions In this novel, comprehensive study assessing multiparametric independent predictors of clinical outcomes for MVD at PPCI in STEMI, WMS at acute CMR was the only independent predictor of final LVEF <35%. Acute IS was the strongest independent predictor of 12-month combined MACE, followed by number of lesions >75% on QCA, and revascularisation strategy. Acute CMR surrogate markers are powerful predictors of medium-term clinical outcomes following PPCI for MVD.
- myocardial infarction
- multivessel disease
- prognosis