Article Text

Statistics from Altmetric.com
The availability of small inexpensive ultrasound devices is a potentially transformative technology. Echocardiography performed at the point-of-care (POC echo) by non-experts might improve diagnosis and management of patients in many clinical settings; examples include evaluation of dyspnea or chest pain in the outpatient clinic, optimization of heart failure therapy in the inpatient setting, and screening large groups of patients in the community such as athletes or those at risk of heart disease. Many cardiology specialists are not supportive of these approaches with the concern that a diagnosis may be missed or incorrect due to suboptimal image acquisition or interpretation. However, POC echo is such a powerful tool that the doubts of cardiovascular specialists will not impede its rapid integration into patient care in every clinical setting. Instead of reacting negatively (and being ignored) to the expansion of echocardiography, we need to actively participate in setting the standards for appropriate training, credentialing, scope-of-practice and quality control for POC echo.
In this issue of Heart, a study by Ploutz and colleagues (see page 35), evaluated the utility of POC echo screening for rheumatic heart disease (RHD) in 956 school children in Uganda. Training in POC echo and a simplified screening protocol for RHD were provided to non-experts in a 4 hour session, followed by 2 days of intensive hands-on experience. Compared to standard imaging by an expert, the sensitivity of non-expert POC echo was about 74% with a specificity of 79% for a borderline or definite diagnosis of RHD. As might be expected, diagnostic errors were most often related to identification and interpretation of the color Doppler mitral regurgitant jet.
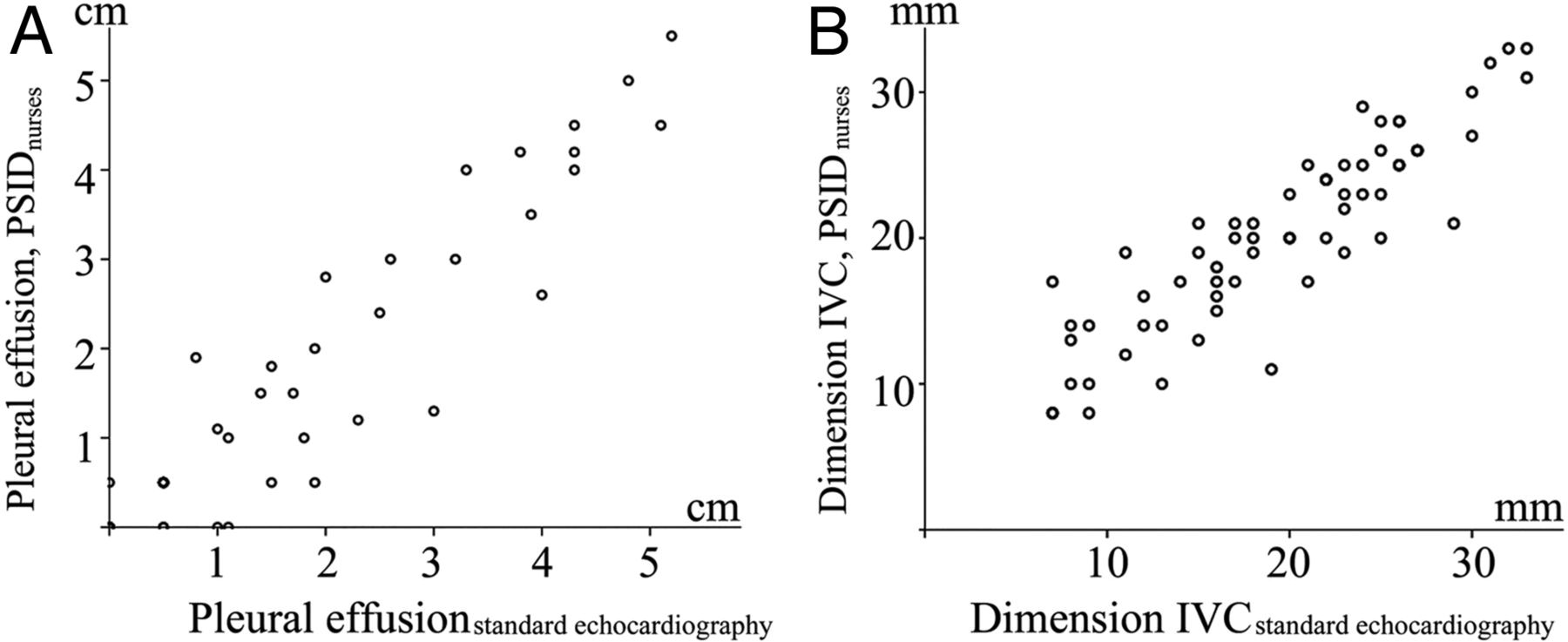
In another study using POC echo, heart failure patients in a nurse-led outpatient clinic were randomized to standard clinical care with or without POC ultrasound to assess volume status. (see page 29) There was a close correlation between ultrasound measurements made by nurses with limited training, compared to standard ultrasound, for pleural effusion size and inferior vena cava diameter (figure 1). Changes in diuretic dose during follow-up were better predicted by ultrasound determined volume status, even when clinical symptoms, physical examination, and laboratory data were considered in the analysis.

Correlation of ultrasound indices to assess volume status by nurses with reference. The figure shows correlation of: (A) quantification of pleural effusion measured as the dimension of fluid between the diaphragm and the lung surface with patients in sitting position; and (B) end-expiratory dimension of the inferior vena cava (IVC) by pocket-size imaging device (PSID) examinations performed by nurses plotted against similar measurements by reference echocardiography. In (A) no effusion measured by both the nurse and reference is shown as the dot at 0; 0 and the dot at 0.5; 0.5 refers to effusion in the costodiaphragmatic recess only measured by both users.
An editorial by Barbosa and Nunes (see page 3) further elaborates on the use of POC echo by non-experts to improve diagnosis and patient care. Although echocardiography detects 4 times more cases of RHD than physical examination alone, the cost of standard echocardiography is prohibitive for community screening in the resource-limited areas where RHD is endemic. POC echo is a promising approach given the lower cost of the instruments, the ability to train non-experts quickly, and the short time (averaging less than 7 minutes) for the screening exam. Although specificity is not ideal, one strategy might be to perform a more detailed echocardiogram only in those with abnormal findings on the POC echo. The randomized study using POC echo for assessment of volume status in heart failure patients also is encouraging, although studies demonstrating the effects on readmission rates and clinical outcomes are lacking. Studies on the potential benefit of POC echo for improving clinical outcomes are needed. Barbosa and Nunes conclude: “Improvement in handheld equipment, making it even easier to be used by non-cardiologists at the point of care, at lower cost, should also be a desired task to be achieved in the near future to allow for a more universal use of this tool in the point of care.”
The potential pleiotropic effect of dabigatran on lipoprotein levels was prospectively evaluated in the 2513 patients in the Randomized Evaluation of Long-Term Anticoagulation Therapy (RE-LY) study. (see page 57) As shown in figure 2, there was a significant (−7%) reduction in apolipoprotein B levels in patients randomized to dabigatran compared to warfarin.

Least-square mean values for the difference in apolipoprotein B (ApoB) concentrations from baseline to 3 months by treatment group. Data presented as least-square mean (95% CI). Covariates in the analysis were treatment group, age, history of cardiovascular disease, diabetes, hypertension, waist to hip ratio, sex, ethnicity, smoking history, previous oral anticoagulant use and baseline ApoB concentration. *=p Value <0.05 when compared with warfarin group.
As eloquently explained by Dr Hugo ten Cate, the presumed mechanism of the decrease in apoliporotein B levels with dabigatran therapy is competition for carboxylesterases, which are needed both for lipoprotein metabolism and for conversion of dabigatran etexilate to its active form (see page 5). In theory, direct thrombin inhibition by dabigatran may also be beneficial because thrombin affects both inflammatory and proliferative pathways that promote atherogenesis (figure 3) although these effects have not yet been studied. As he suggests: “The long-term use of new classes of anticoagulants that may interfere with the many biological effects of thrombin and other serine proteases in complex processes like atherothrombosis deserves attention from the medical community currently embracing new direct oral anticoagulants as practical, effective and safe anticoagulants.”

Thrombin is involved in many pathways in atherogenesis (including inflammation and proliferation); blocking thrombin's catalytic activity with dabigatran will also diminish the potential of thrombin to bind and activate protease activated receptor-1 (PAR-1), resulting in attenuated effects of thrombin on atherogenesis (indicated by the blocked arrow). The potentially pleiotropic actions of thrombin in vivo may be supported by the observed effect of dabigatran lowering apoB levels in blood, presumably by competitive use of carboxylesterases for activation of the prodrug dabigatran etexilate to the active dabigatran (indicated in the left upper part of the figure, by arrows).
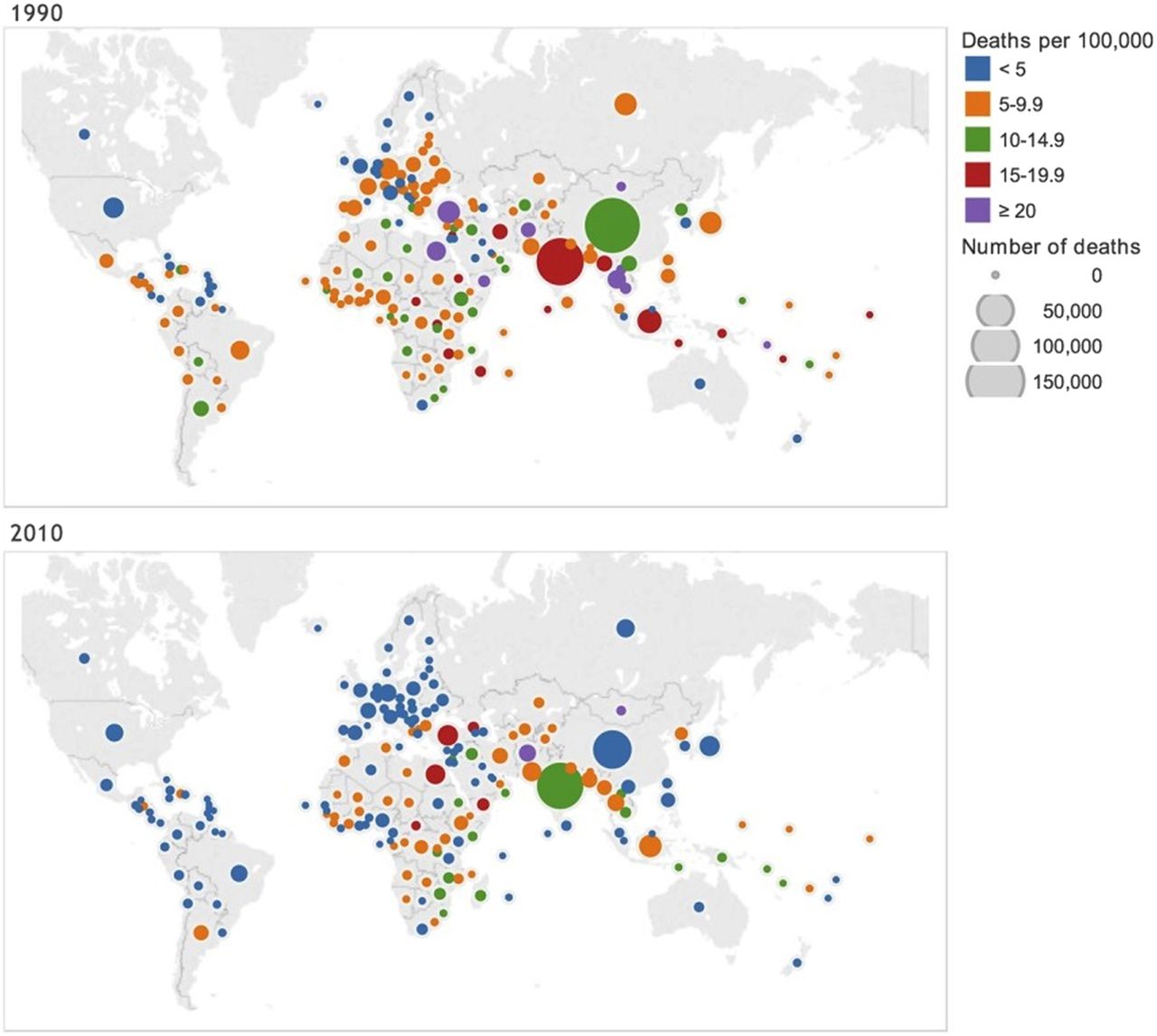
The Education in Heart article in this issue (see page 75) brings us up to date on the epidemiology of valvular heart disease. Rheumatic heart disease prevalence is declining but remains the major cause of heart valve disease worldwide (figure 4). In high-income countries, calcific aortic stenosis is a major contributor to deaths due to heart valve disease. Endocarditis occurs in only between 1 and 11 per 10 0000 people per year but continues to be a highly fatal disease with 30 day mortality rates in excess of 20%. In addition, there is an increased incidence of infections in older patients with cardiac implanted electronic devices; about 1/3 of these cases have valvular involvement.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Change in age-standardised mortality rate due to rheumatic heart disease from 1990 to 2010. Data were obtained from the Global Burden of Disease study. The colour of the circles indicates the mortality rate category, while the area of the circle indicates number of deaths. Mortality rate can be seen to have decreased in most countries, accompanied by a reduction in numbers dying. The country with the highest numbers of deaths from rheumatic heart disease was China in 1990 and was India in 2010. An interactive data visualisation is available at: http://oxvalve.nhs.uk/research/rhdmap
The image challenge case in this issue shows an echocardiographic image with an interesting differential diagnosis. (see page 39) Clinical cardiologists and those in training should get this right!
Linked Articles
- Heart failure and cardiomyopathies
- Cardiac risk factors and prevention
- Education in Heart
- Valvular heart disease
- Editorial
- Editorial