Article Text

Statistics from Altmetric.com
Loneliness and social isolation as risk factors for CVD
A recent meta-analysis has shown that loneliness and social isolation are risk factors for coronary heart disease and stroke.1 These latest findings, specific to cardiovascular outcomes, are consistent with substantial research indicating broad health risks (eg, immune functioning, cardiovascular functioning, cognitive decline) associated with the quantity and quality of social relationships—including several meta-analyses documenting mortality risk.2 ,3 In the most comprehensive of these,3 the overall odds for mortality was 1.50, similar to the risk from light smoking and exceeding the risks conferred by hypertension and obesity. Thus, the epidemiological data suggest that having more and better quality social relationships is linked to decreased health risks and having fewer and poorer quality relationships increased risk.2 ,3
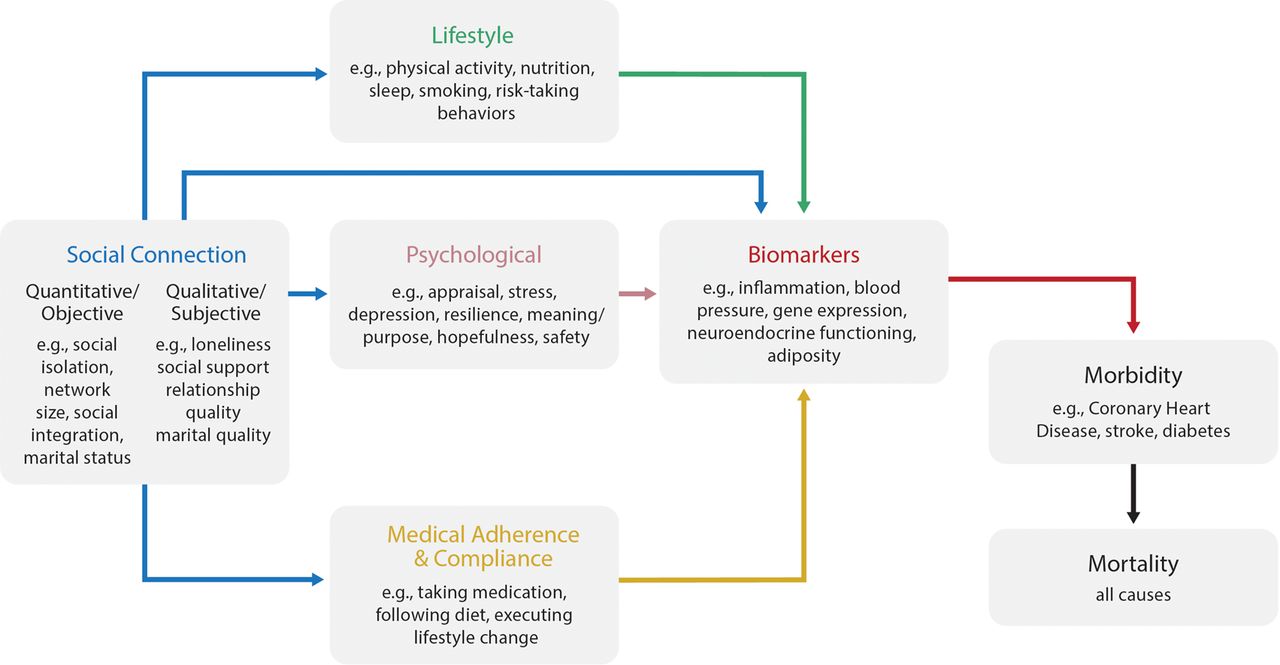
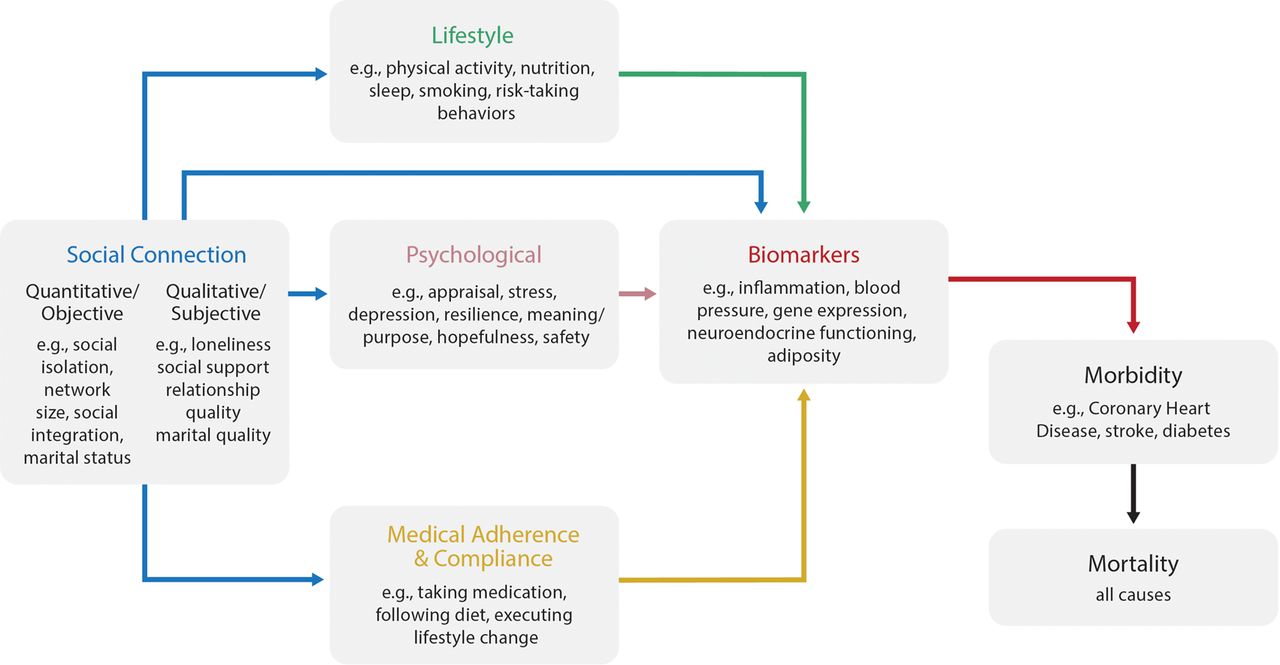
Research has also documented the influence of social connections (including measures specific to loneliness and isolation) on multiple pathways involved in both the development and progression of coronary heart disease and stroke. As depicted in figure 1, these include lifestyle (eg, nutrition, physical activity, sleep),4 treatment adherence and cooperation,5 and direct effects on surrogate biological markers.6 ,7 Recent longitudinal data from four nationally representative US samples revealed a dose–response effect of social integration on several surrogate biomarkers of cardiovascular disease including hypertension, body mass index, waist circumference and inflammation (hs-CRP).6 Moreover, most epidemiological studies control for lifestyle factors (eg, smoking, physical activity), documenting an independent influence of social relationships on mortality. Taken together, these latest findings specific to loneliness and isolation1 bolster the already robust evidence documenting that social connections significantly predict morbidity and mortality, supporting the case for inclusion as a risk factor for cardiovascular disease (CVD).
{kind=link}
Simplified model of possible direct and indirect pathways by which social connections influence disease morbidity and mortality.
Targeting social isolation and loneliness in evidence-based patient care
How should these data inform clinical practice? To begin, the data suggest the need for greater prioritisation and inclusion of social variables (quantity and quality) in medical education, individual risk assessment and public health surveillance, guidelines and policies applied to populations and health service delivery.
Medical education
The cumulative evidence points to the benefit of including social factors in medical training and continuing education for healthcare professionals. Physicians supervising students and residents’ can assess patients’ social risk factors and then discuss with patients the importance of nurturing and maintaining positive social connections as part of a healthy lifestyle. Evidence-based training could include social factors in medical case examples and textbooks to provide realistic patient descriptions with life circumstances relevant to disease development, progression and response to treatment. For instance, a case description of a 55-year-old male with hypertension and atrial fibrillation who is responding poorly to treatment could include relevant circumstances of intense marital conflict that have elevated levels of distress and increased adiposity due to increased consumption of low quality foods away from home. Given the multiple social factors associated with health conditions and patients’ responses to treatment, medical training that requires consideration of patients’ social circumstances could improve patients’ outcomes.
Medical training can also make explicit the processes for making effective referrals to mental health and social support services. In the hypothetical case of the patient mentioned above, referral for marital counselling and stress management therapy would be indicated. Medical training can encourage physicians to proactively identify relevant social and psychological conditions, rather than ignore those conditions simply because they would be treated by another specialist. In the same way cardiologists refer and follow-up with patients who have comorbid renal disease, they should refer and follow-up with patients experiencing social isolation or distress. Social factors must now be given attention in coursework detailing the major findings of health psychology and neuroscience, rather than relegating such information to a side note (eg, a mini-lecture during students’ exposure to psychiatry).
Risk assessment
Patient information should be used to inform treatment. Hospitals and clinics should include assessments of social integration and/or loneliness in electronic medical records. This important step can identify individuals at risk—which may also have multiple implications for health service delivery. Further, at a broader level, population-wide surveillance will aid public health efforts.
Such efforts will require multifactorial risk assessment. While short and simple assessments are desirable, single-item assessments would be insufficient and problematic. According to meta-analytic data,3 multivariate measures of social relationships yield data much more predictive of death (OR=1.91) than simplistic measures (OR=1.19). Further, although loneliness and social isolation entail equivalent levels of risk, they are not interchangeable. Social isolation denotes few social connections or interactions, whereas loneliness involves the subjective perception of isolation—the discrepancy between one's desired and actual level of social connection. Although social isolation and loneliness may co-occur, individuals can be isolated without feeling lonely or feel lonely despite having others present. Thus assessments should include objective/quantitative aspects of relationships (eg, network size, marital status), as well as more subjective/qualitative aspects (eg, loneliness, social support, perceived relationship quality). Each significantly predicts risk for mortality,3 and may potential tap into different mechanistic pathways; thus, multifactorial assessments may best capture overall risk. A key challenge will be how to develop a point-of-care assessment that is multifaceted, has predictive validity, and easily incorporated into day-to-day clinical practice.
Population-based recommendations and policies
The WHO now lists ‘Social Support Networks’ as a determinant of health (http://www.who.int/hia/evidence/doh/en/). Major health organisations specific to cardiovascular disease (eg, American Heart Association, British Heart Foundation) should also include social connections in their lists of major risk factors, similar to comparable lifestyle factors that currently receive sustained attention. Government and professional health organisations will need to establish recommendations for social relationship quantity and quality for the broader population and specific risk groups. These recommendations should be based on empirical evidence, subject to periodic revision and annual public health surveillance.
Among other European nations, the UK has already undertaken several public health initiatives intended to reduce social isolation and decrease risk for premature mortality. Current efforts are focused primarily on older adults or individuals reporting high levels of loneliness; however, recommendations and cautions can be broadly applied. A broad approach is supported by evidence indicating (a) remarkable consistency of effect across different countries and across multiple individual characteristics (eg, gender, health status), with data suggesting greater relative risk prior to retirement age;2 (b) a gradient effect of social connection rather than a threshold effect3 ,6 and (c) social relationships affect cardiovascular health by altering biomarkers and shaping health behaviours across the lifespan—including adolescence, young adulthood, middle age and old age.6 Thus, efforts to promote public health via social connection need not be limited to specific groups but can be applied across the risk trajectory.
Health service delivery: prevention
Attention to social connection needs to be incorporated into existing preventative efforts. Chronic illnesses, including cardiovascular diseases, develop slowly over decades. Because social relations influence multiple mechanistic pathways in both the development and progression of disease, they warrant attention in primary, secondary and tertiary prevention efforts. Given efforts aimed at primary prevention result in lower economic costs to the individual, family, employers and the broader healthcare system—we urge healthcare and health policy professionals to prioritise social connections in prevention efforts.
Further scientific inquiry
Despite robust literature of epidemiological evidence, several important questions remain.
Causal mechanisms
Social isolation and loneliness are clearly risk factors for cardiovascular disease (CVD).8 However, the term risk factor can imply prediction and causality, and causality is not easily established. Similar to other risk factors for CVD (eg, hypertension, obesity, smoking, cholesterol levels) the influence of social relationships is complex and multifactorial (no single putative mechanism).8 Furthermore, we must take a multilevel approach considering microlevel (eg, genetic markers of susceptibility, gene–environment interactions) to macrolevel (eg, cultural norms, neighbourhood characteristics) processes to better understand additional pathways by which social relationships influence physical health, as well as the pathways by which we may intervene to reduce risk and improve health.
Interventions
Perhaps the biggest challenge and opportunity for the future is to design effective interventions to increase social connections. Previous interventions involving social support have had mixed results. Additional research is needed to determine what works best for whom, in what conditions. Notably, the major effects established via epidemiological data are based on existing social relationships (eg, family, friends), yet many clinical interventions use hired personnel to deliver support to patients. This discrepancy may be problematic because support from the patients’ family and broader social networks may differ from that provided by hired personnel in several important ways (eg, trust built over decades, regular social contact, importance of the relationship, degree of social control, sense of obligation in the relationship). Thus, efforts to strengthen existing family relationships may prove more effective than interventions by hired personnel.
On a related note, policies that for essential reasons restrict access to patients’ medical records and information may have indirectly contributed to a practice climate not conducive to family involvement, even when the patient authorises family involvement. Hospitals and clinics should make efforts to enhance family involvement when authorised by the patient.
Social technology
Social technology has rapidly become a dominant form of communication and social interaction. While existing and developing technology has the potential to combat loneliness and isolation (facilitating social connection), it may also contribute to problems exacerbating risk. With such rapid changes in the way people are interacting socially, empirical research is needed to address several important questions. Does interacting socially via technology reduce or replace face-to-face social interaction and/or alter social skills? Due to the rapid and instant access afforded, does technology accelerate relationship processes (both positive and negative) leading to accentuation of sociality or lack thereof? Do social relationships/interactions via technology have a similar influence health and well-being?
Conclusions
Decades of research have documented an unequivocal influence of social connections on longevity,2 ,3 with a recent meta-analysis confirming the association between social isolation and CVD.1 Given projected increases in levels of social isolation and loneliness in Europe and North America, medical science needs to squarely address the ramifications for physical health. Similar to how cardiologists and other healthcare professionals have taken strong public stances regarding other factors exacerbating CVD (eg, smoking, diets high in saturated fats), further attention to social connections is needed in research and public health surveillance, prevention and intervention efforts. Those efforts will necessarily integrate methods and findings from related disciplines and expand the complexity of research questions and analyses.
Supplementary materials
Press release
Files in this Data Supplement:
Footnotes
Twitter Follow Julianne Holt-Lunstad at @jholtlunstad
Contributors JHL and TBS participated in the drafting of this editorial and take full responsibility for its content.
Competing interests None declared.
Provenance and peer review Commissioned; internally peer reviewed.