Article Text

Abstract
Objective International guidelines to rule-in acute myocardial infarction (AMI) in patients presenting with chest pain to the emergency department (ED) recommend an algorithm using high-sensitivity cardiac troponin (hs-cTn) sampling on presentation and 3 h following presentation. We tested the diagnostic accuracy of this algorithm by pooling data from five distinct cohorts from three countries of prospectively recruited patients with independently adjudicated outcomes.
Method We measured high-sensitivity cardiac troponin I (hs-cTnI) and high-sensitivity cardiac troponin T (hs-cTnT) on presentation (0 h) and 3 h post-presentation samples in adult patients attending an ED with possible AMI to validate the European Society of Cardiology (ESC) Working Group on Acute Cardiac Care rule-in algorithm (ESC-rule-in). Specifically, (i) in patients with a 0 h hs-cTn concentration ≤99th percentile and a 3 h hs-cTn >99th percentile, positive patients are those with an absolute change in troponin ≥50% of the 99th percentile, and (ii) in patients with a 0 and 3 h hs-cTn >99th percentile, positive patients are those with a relative change in troponin of ≥20%. We concurrently assessed the efficacy of the 0 and 3 h hs-cTn <99th percentile to rule-out AMI.
Results 1061 patients with hs-cTnI and 985 with hs-cTnT were included. The ESC-rule-in positive predictive value (PPV) was 83.5% (95% CI 74.9% to 90.1%) for hs-cTnI and 72.0% (95% CI 62.1% to 80.5%) for hs-cTnT. Forty-six AMIs (34.9%) were not ruled in using hs-cTnI and 62 (46.2%) using hs-cTnT. The sensitivity of the 99th percentile to rule-out AMI was 93.2% (95% CI 87.5% to 96.8%) for hs-cTnI and 94.8% (95% CI 89.5% to 97.9%) for hs-cTnT.
Conclusions The ESC-rule-in algorithm has good PPV with hs-cTnI and reasonable with hs-cTnT and can rule-in over 50% of AMIs. However, the sensitivity of the 99th percentile to rule-out AMI is too low for clinical use.
Statistics from Altmetric.com
Introduction
High-sensitivity cardiac troponin (hs-cTn) assays have excellent analytical precision at low troponin concentrations and may accelerate the diagnosis of acute myocardial infarction (AMI) by detecting myocardial injury at earlier time points within the emergency department (ED) early after symptom onset. This may enable early treatment and potentially reduce morbidity.1 For this purpose, the European Society of Cardiology (ESC) Working Group on Acute Cardiac Care proposed a rule-in algorithm (ESC-rule-in), which combines a >20% relative change for patients with 0 h troponin above the 99th percentile of a healthy population with an absolute change for those below the 99th percentile.2 In doing so, they acknowledged the limited evidence for such an approach. Keller et al found that a prototype high-sensitivity cardiac troponin I (hs-cTnI) could be used to rule-in AMI when combining a positive 0 h result with a sufficient relative increase in concentration.3 ,4 Serial sampling of high-sensitivity cardiac troponin T (hs-cTnT) at 0 h and between 3 and 6 h5 and at 0 and 2 h6 best ruled-in AMI when an absolute rather than a relative increase in concentration was used. Wildi et al noted that a potential advantage of a rule-in protocol which included changes in cardiac troponin was the possibility of faster rule-out of AMI.7 A rule-in strategy requires high positive predictive value (PPV) because invasive testing is likely for those patients identified as probably having an AMI.
The 2011 ESC guidelines for management of acute coronary syndrome without persistent ST-segment elevation recommended 0 and 3 h sampling to rule-out AMI.8 Once more, this was based on limited data. Similarly, the recent National Institute for Health and Care Excellence (NICE) diagnostics guidance for hs-cTn assays recommended for use with early rule-out protocols, an ‘initial assessment in an emergency department and a second blood sample taken after 3 hours’.9 Time periods as short as 1 h between sampling have been proposed.10 ,11 Because of the potential serious consequences of missed AMI, a rule-out strategy requires very high sensitivity.
We aimed to validate the ESC-rule-in algorithm in patients presenting acutely to EDs with chest discomfort that might be due to an AMI and using a commercially available hs-cTn assays. We further evaluated the use of the 99th percentile as a cut-off to rule-out AMI. We also aimed to use the findings to develop one algorithm to identify both very low-risk and high-risk patients. Finally, we evaluated the performance of hs-cTn at presentation below the level of detection to rule-out AMI.
Methods
We used data collected from four studies (five cohorts) of patients with chest pain presenting to the ED, namely the Brisbane, Australia, and Christchurch, New Zealand, cohorts of the 2-Hour accelerated diagnostic protocol to assess patients with chest pain symptoms using contemporary troponins as the only biomarker (ADAPT) observational study,12 the ADAPT-Accelerated Diagnostic Pathway (ADP), the Emergency Department Assessment of Chest pain score (EDACS) randomised controlled trials (both Christchurch),13 and the reducing the time Interval for identifying new guideline (RING) study in Hamilton, Canada.14 The studies employed very similar inclusion and exclusion criteria; eligible patients were aged ≥18 years, presenting acutely from the community to the ED with chest pain suggestive of AMI for whom, following initial clinical assessment, the attending physician(s) planned to investigate for AMI with serial biomarker tests. In accordance with American Heart Association case definitions, possible cardiac symptoms included: the presence of acute chest, epigastric, neck, jaw or arm pain or discomfort or pressure without apparent non-cardiac source.15 Patients were excluded if any of the following conditions were satisfied: ST-segment elevation myocardial infarction present on any ECG; chest pain episode began >12 h prior to assessment (>6 h for the RING study), proven or suspected non-coronary pathology as the cause of chest pain; need for admission regardless of a negative cTn, due to other medical conditions or need for other investigations; previously enrolled in this study; anticipated problem with follow-up (eg, resident outside the country or terminal illness) and unable or unwilling to provide informed consent. We included only type I AMI.
The planned sampling time points for each study were on presentation and 2 h later (Brisbane ADAPT, Christchurch EDACS); 1, 2 and 24 h later (Christchurch ADAPT); 2 and 4 h later (Christchurch ADAPT-ADP) and 3 h later (RING). From these samples, we extracted all patients with hs-cTnI and hs-cTnT measurements on presentation to the ED (0 h sample) and again at 3 h from presentation (3 h sample). The ESC Working Group acknowledged a paucity of data on timing and recommended additional blood sampling in patients strongly suspected of having an AMI, but no significant hs-cTn increase after 3 h.2 Therefore, we chose to define the 3 h sample as samples taken from 3 h to <4.5 h from presentation. We further excluded all patients with a positive ECG (not known to be old ischaemic changes, namely: ST-segment depression of at least 0.05 mV in two or more contiguous leads, T-wave inversion of at least 0.1 mV or Q-waves >30 ms in width and ≥0.1 mV in depth in at least two contiguous leads) on presentation as these would normally be regarded as high risk.
Reference standard
Classification of AMI for all studies was based upon global taskforce recommendations requiring evidence of myocardial necrosis together with evidence of myocardial ischaemia (ischaemic symptoms, ECG changes or imaging evidence).16 Reference (local laboratory) cardiac troponin assays in use for clinical adjudication of AMI for each cohort were: Access AccuTnI (Beckman Coulter, Chaska, Minnesota, USA) for Brisbane ADAPT, Elecsys troponin T fourth-generation assay (Roche Diagnostics, Basel, Switzerland) for Hamilton RING, ARCHITECT troponin I (Abbot Diagnostics, Chicago, Illinois, USA) for Christchurch ADAPT and ADAPT-ADP and ARCHITECT hs-cTnI (Abbot Diagnostics) for Christchurch EDACS-ADP. Necrosis was diagnosed on the basis of a rising or falling pattern of the reference troponin concentration, with at least one concentration above the 99th percentile and normally a 20% change. For the RING study, as the hs-cTnT fourth-generation 99th percentile concentration was below the limit of detection (LoD), the 10% coefficient of variation (CV) concentration was used,17 ,18 with typically a change of >3 SD of the directly observed imprecision of the assay used for concentrations below 0.10 μg/L and 20% relative change at higher concentrations.19 For the Christchurch cohorts a delta was not rigidly specified, although 20% was commonly used. The second reference troponin was taken at least 6 h after the first in all cohorts. Outcomes and investigations were reported with minimal subjectivity using predefined standardised reporting guidelines.16 ,20 For the Australian and New Zealand cohorts, the presence of AMI was adjudicated independently by local cardiologists using these reporting guidelines and blinded to the results of the hs-cTn except in the case of the EDACS trial, where hs-cTnI was the clinical assay in use. If the reference cardiac troponin was above the reference range, but there was no rise or fall, other causes of a raised cardiac troponin were considered. If no clear alternative cause of the cardiac troponin rise was apparent then, if the clinical presentation was suggestive of acute coronary syndrome, an adjudicated diagnosis of AMI was made. A panel of two cardiologists performed the adjudication independent of each other with a third cardiologist making an independent adjudication in cases of disagreement. For the Canadian cohort, an internal medicine specialist and emergency physician (blinded to the hs-cTn concentrations) independently adjudicated the events in a similar manner as described above.
Index test
We assessed the performance of ESC proposed rapid rule-in AMI strategy (ESC-rule-in; table 1). We determined the absolute delta (δa=|3 h hs-cTn – 0 h hs-cTn|) and relative delta (δr=100×|3 h hs-cTn – 0 h hs-cTn|/0 h hs-cTn) for each patient and each assay. ESC-rule-in categorises as test positive patients by one of two pathways: (i) in patients with a 0 h hs-cTn concentration ≤99th percentile and a 3 h hs-cTnI >99th percentile, positive patients are those with δa >50% of the 99th percentile or (ii) in patients with both 0 and 3 h hs-cTn >99th percentile, positive patients are those with δr >20%. We determined the proportion of high-risk patients identified by the strategy. The cardiac troponins evaluated were the Abbott ARCHITECT hs-cTnI and Roche fifth-generation hs-cTnT assays. The hs-cTnI assay has reported LoD of <2 ng/L, 99th sex-specific percentile for a healthy population of 16 ng/L for women and 34 ng/L for men, and a 99th percentile overall specific threshold of 26 ng/L.21 ,22 The hs-cTnT assay has an LoD of <5 ng/L and 99th percentile of 14 ng/L.23 The hs-cTnT was not measured on the EDACS samples. As measurements were made at different times on available samples, not all patients had both hs-cTn measured. This accounts for the differing total sample number and number of AMI for the assessment of hs-cTnI and hs-cTnT. We concurrently assessed the efficacy of 0 and 3 h hs-cTn <99th percentile and 0 h <LoD to rule-out AMI.
Index tests
Sensitivity analysis
We conducted a sensitivity analysis by assessing each cohort separately. In particular, we compared the performance of the algorithm, where hs-cTnI was used as the reference standard (EDACS randomised controlled trial (RCT) cohort) with the other cohorts, where an earlier generation cardiac troponin was used as the reference standard.
Alternate algorithm development
We determined, independently, which of δa and δr thresholds for an 80% PPV identified the greatest proportion of AMIs (high-risk group). Eighty per cent PPV was chosen after consultation with several cardiologists to determine a likely acceptable rate of false positives. We also determined the hs-cTnI threshold (maximum of the two samples), which gave a >99% sensitivity. We combined these into a single algorithm.
Statistical analysis
All CIs presented are exact binomial 95% CIs. Statistical calculations were performed with R V.3.1.0.24
Results
The five studies recruited 4908 patients, of these 1172 patients had both 0 and 3 h hs-cTnI samples (drawn from all five cohorts) and 1098 patients had both 0 and 3 h hs-cTnT samples (drawn from four cohorts). More than half the patients were male (58%), had hypertension, dyslipidaemia or a family history of ischaemic heart disease (table 2).
Cohort characteristics
High-sensitivity cardiac troponin I
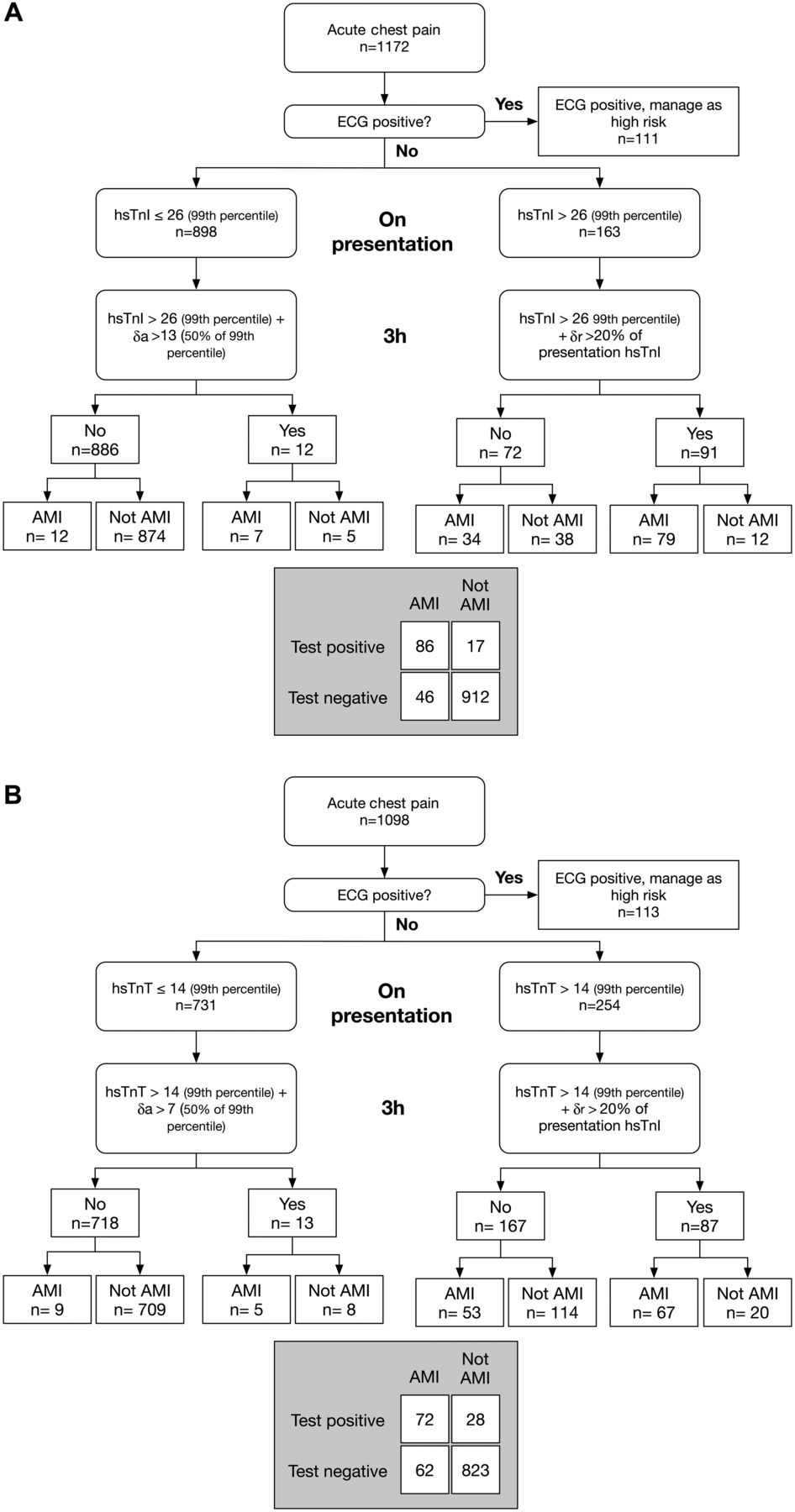
Of the 1172 patients, 111 had a positive ECG leaving 1061 for this analysis. The 3 h sample was taken a median 3 h 37 min (IQR: 3 h 15 min to 4 h 10 min; minimum 3 h 0 min, maximum 4 h 30 min) hours following presentation. One hundred and thirty-two (12.4%) patients were diagnosed with AMI. The majority of patients (84.4%) had 0 h hs-cTnI <99th percentile, therefore, went through the arm of the ESC-rule-in test that used a δa >50% of the 99th percentile (>13 ng/L), where the second troponin was >99th percentile to identify myocardial injury (figure 1A). Seven (8.1%) of the 86 AMI identified by ESC-rule-in went through this arm. In both arms, the ESC-rule-in test identified 103 patients as positive, of whom 17 were false positives (table 3; test (i)). The PPV was 83.5% (95% CI 74.9% to 90.1%). The specificity was 98.2% (95% CI 97.1% to 98.9%). Forty-six (34.9%) AMIs were not ruled in.
Diagnostic metrics for each index test

European Society of Cardiology (ESC)-rule-in. (A) hs-cTnI and (B) hs-cTnT. AMI, acute myocardial infarction; hs-cTnI, high-sensitivity cardiac troponin I; hs-cTnT, high-sensitivity cardiac troponin T.
The sensitivity for 0 and 3 h hs-cTnI at the 99th percentile threshold was 93.2% (95% CI 87.5% to 96.8%) (table 3; test (ii)). Only one of the false negative (FN) had symptom onset <3 h prior to the first sample (it was 2 h 50 min). One FN was diagnosed unstable angina on day 1, but on day 2 the cardiac troponin concentrations were elevated and AMI was diagnosed. Five others were diagnosed through a troponin rise within 6–18 h, the other two had elevated cardiac troponins at time 0 and subsequent angiography verified the diagnosis. At 0 h with the LoD threshold, 5.2% of patients were low risk with a sensitivity of 100% (95% CI 95.8% to 100%) (table 3; test (iii)).
Sensitivity analyses
There were only minor changes in PPV and sensitivity when sex-specific thresholds (hs-cTnI for male=34 ng/L and for female=16 ng/L) were applied rather than the overall threshold (hs-cTnI=26 ng/L). There were three additional false positives for hs-cTnI rule-in reducing the PPV to 81.0% (95% CI 72.1% to 88.0%) and one additional FN for the rule-out for either 0 or 3 h hs-cTnI <99th percentile reducing the sensitivity to 92.4% (95% CI 86.5% to 96.3%).
The ESC-rule-in algorithm performed similarly in each cohort with the exception of RING, where the PPV was very low as a result of few patients with a positive test (table 4). The 99th percentile rule-out showed greater variation in sensitivity, but with large CIs (table 5).
Diagnostic metrics by cohort for ESC-rule-in overall 99th percentile threshold
Diagnostic metrics by cohort for the 99th percentile 0 and 3 h rule-out test
Simplified algorithm development
At a PPV of 80.0%, a δr=200% identified only 4.1% as high risk (figure 2A). At a PPV of 80.0%, a δa=12 ng/L identified 11.8% as high risk of myocardial injury (figure 2B). At a sensitivity of >99%, a hs-cTnI threshold of 5 ng/L identified 49.9% at low risk of AMI. Therefore, we combined δa=12 ng/L and a hs-cTnI threshold of 5 ng/L into one algorithm, which enabled 11.8% of patients to be identified as high risk and eligible for early intervention, 38.3% were intermediate risk and 49.9% as low risk and eligible for consideration for early discharge (figure 3A). The proportion of high-risk patients was marginally greater than the ESC-rule-in test with 8 more false positives and 14 more true positives. Seventy-six per cent of AMI were ruled in. The proportion of low-risk patients was lower than the 99th percentile rule-out algorithm, but with only one rather than nine FNs and a sensitivity of 99.2% (95% CI 95.9% to 100%).

The positive predictive value and proportion of high-risk (greater than the threshold defined by the difference) patients for (A) a relative change in hs-cTnI, (B) an absolute change in hs-cTnI. hs-cTnI, high-sensitivity cardiac troponin I.

{kind=link}
{kind=link}
{kind=link}
Simplified risk assessment strategy based on the maximum of two hs-cTn samples and the delta value of the difference between them. (A) hs-cTnI, (B) hs-cTnT. AMI, acute myocardial infarction; hs-cTnI, high-sensitivity cardiac troponin I; hs-cTnT, high-sensitivity cardiac troponin T; NPV, negative predictive value; PPV, positive predictive value.
High-sensitivity cardiac troponin T
Of the 1098 patients, 113 had a positive ECG leaving 985 for this analysis. The 3 h sample was taken at a median 3 h 37 min (IQR: 3 h 15 min–4 h 9 min; minimum 3 h 0 min, maximum 4 h 30 min) hours following presentation. One hundred and thirty-four (13.6%) patients were diagnosed with AMI. The majority of patients (74.2%) had 0 h hs-cTnT <99th percentile, therefore, went through the arm of the ESC-rule-in test that used a δa >50% of the 99th percentile (>7 ng/L), where the second troponin was >99th percentile to identify myocardial injury (figure 1B). Five (6.9%) of the 72 AMI identified by ESC-rule-in went through this arm. In both arms, the ESC-rule-in test identified 100 patients as positive, of whom 28 were false positives (table 3; test (iv)). The PPV was 72.0% (95% CI 62.1% to 80.5%). The specificity was 96.7% (95% CI 95.3% to 97.8%). Sixty-two (46.2%) AMIs were not ruled in.
The sensitivity for 0 and 3 h hs-cTnT at the 99th percentile threshold was 94.8% (95% CI 89.5% to 97.9%) (table 3; test (v)). Four of the seven FNs were the same as for hs-cTnI. The other three showed a cardiac troponin rise over 6–18 h. At 0 h with the LoD threshold, 30.4% of patients were low risk with a sensitivity of 99.3% (95% CI 95.9% to 100%) (table 3; test (vi)).
Simplified algorithm development
Combining δa=9 ng/L and a hs-cTnT threshold of 5 ng/L into one algorithm enabled 10.1% of patients to be identified as high risk and eligible for early intervention, 59.6% of intermediate risk and 30.7% as low risk and eligible for consideration for early discharge (figure 3B). The proportion of high-risk patients was marginally greater than the ESC-rule-in test with one more false positives and 13 more true positives; 57.0% of AMI were ruled in. The proportion of low-risk patients was lower than the 99th percentile rule-out algorithm but with only one FN and a sensitivity of 99.3% (95% CI 95.9% to 100%). Reducing the threshold to 4 ng/L removed the FNs, but reduced the overall low-risk proportion to 37.8%.
Discussion
The ESC-rule-in test among patients with no new ischaemic changes on ECG from five cohorts from three countries performed well for hs-cTnI with good PPV (84%) enabling the rapid rule-in of 65% of AMIs and less well for hs-cTnT with adequate PPV (72%) enabling rule-in of 54% of AMIs. This is the first validation study of this test. This is particularly important given the acknowledged paucity of evidence to support the algorithm.
Conversely, serial cardiac troponins alone at 0 and 3 h had inadequate sensitivity (hs-cTnI, 93%; hs-cTnT, 95%) for clinical use as a rule-out tool, where the consensus is that 99% sensitivity is required.25 We have previously shown that in a smaller study where samples were prospectively collected on presentation and 4 h later, the sensitivity of this algorithm for hs-cTnI was also low (92.1% (95% CI 82.4% to 97.4%)).26 The NICE guidelines suggested that the 99th percentile could be used to rule-out AMI in people aged ≥70 years or without pre-existing coronary artery disease (CAD) or classified as having a high pretest probability of AMI. Of the 12 FN patients by this definition with either hs-cTn, five were ≥70 years old and three of the others had no pre-existing CAD. Therefore, at least eight would have been FNs in a smaller subgroup. The other four, all had a history of AMI and with previous percutaneous coronary angioplasty (PTCA) or coronary artery bybass graft (CABG) and so may be considered to mean a high pretest probability of AMI. Our findings, therefore, contradict the NICE recommendation, which was also based on a paucity of evidence.
Clearly, to rule-out AMI on the basis of serial cardiac troponin alone requires a more sophisticated approach than merely to apply the 99th percentiles as thresholds. The cardiac troponin T -hs (high sensitivity) assay for RAPID rule-out of acute myocardial infarction (TRAPID) algorithm for use with hs-cTnT was developed without consideration of the 99th percentiles and applies a threshold lower than the 99th percentile together with a very small delta over 1 h to rule-out AMI.10 ,11 This approach allows one algorithm to be used to identify low-risk and high-risk patients. The rest of the patients fall into an intermediate zone requiring further observation before clinical decision can be made. We employed a similar philosophy to the TRAPID algorithm to develop a simple algorithm to place patients into low-risk, high-risk or intermediate-risk categories after two hs-cTn measurements. The proportions in each category critically depend on the rule-out and rule-in thresholds chosen. We based the rule-out threshold on that which achieved a 99% sensitivity because 99% is the sensitivity acceptable to most emergency physicians.25 Over 30% of patients could be ruled out in this way with hs-cTnT and nearly 50% with the hs-cTnI algorithm, comparable with the highest values of accelerated chest pain pathways based on scoring systems.27 While the negative predictive value was excellent, the lower 95% CI for the sensitivity for this threshold was only 96%. If the population sensitivity was at this value, it would lead to an unacceptable FN rate. This highlights the importance of external validation.
The choice to determine the delta rule-in threshold as that which produced 80% PPV was arbitrary and based on discussions with cardiologists as to what they considered an acceptable false positive rate for patients referred to them from ED. A balance between minimising false positives (which may result in over investigation and excess demand on cardiology services) and the desire for a simpler process than that proposed by the ESC-rule-in algorithm is required. An alternative would be to use, say, 90% PPV which, for example, in this cohort for hs-cTnI would mean a rule-in threshold δa=20 ng/L. This would result in a reduction of 16 false positives at a cost of nine fewer AMI being assigned to the high-risk group, decreasing the proportion of AMI identified to 65% and the proportion of the cohort designated as high risk to 9.7%.
The study has some limitations. First, there is a risk of incorporation bias because one study (EDACS) used an hs-cTn assay as the reference test. Furthermore, some patients with an evident >20% change in hs-cTn were not classified as AMI with contemporary troponins who may otherwise been so diagnosed (see online supplementary figure). It is possible that the use of a discrepant reference standard troponin may result in an underestimation of the diagnostic accuracy. In particular, because contemporary assays have a high CV below the 99th percentile, it is less likely a sufficient delta for a patient to be diagnosed with AMI be observed for those patients with an initial troponin concentration less than the 99th percentile than if a high-sensitivity troponin was used as the reference standard. In choosing to use PPV to determine the optimal delta for a rule-in model, we acknowledge that PPV is prevalence dependent. This was a pragmatic choice because the attending cardiologists were most interested in minimising false positives, yet for it to be a practical strategy for early identification of AMI, a reasonable proportion of AMI must be identified. We note, though, that the specificity was high for this strategy. Furthermore, the choice of 80% PPV is somewhat arbitrary and depends on local cardiology practices. Nevertheless, for these reasons the simplified algorithm should be considered hypothesis generating only and represents a methodology of determining an acceptable delta. It awaits validation in a prospective study employing hs-cTnI as the reference test. Also, the studies were not designed specifically to examine these algorithms and the samples chosen were simply those where there was a paired sample with the second sample being 3–4.5 h postpresentation. Only the RING study prespecified 0 and 3 h time points. The samples chosen from the other studies just happened to fall into the range because the practicalities of taking samples were prespecified time points (0 and 2 h or 0 and 4 h in some cases), or clinician choice, meant some samples were delayed or early and so fell into the requisite time difference zone. This, therefore, meant many other patients in those studies were excluded from this analysis. Finally, the exclusion and inclusion criteria for each of these studies means that compared with a typical clinical situation, there may be fewer low-risk patients. It is worth noting that AMI prevalence was greater in the Christchurch cohort than the other cohorts and greater than many other international studies. This is because of a well-developed and funded primary healthcare, which is effective at screening out many patients that might otherwise present to the ED in other health systems. In lower prevalence cohorts, we may expect a greater proportion of low risk and similar sensitivity.
Supplementary figure
Conclusion
The ESC-rule-in algorithm has good specificity and can rule-in approximately 60% of AMIs. However, the sensitivity of serial sampling (0 and 3 h) of hs-cTn using the 99th percentile to rule-out AMI is too low for clinical use with either hs-cTn assay. An alternative algorithm of an absolute delta hs-cTnI of >12 ng/L to rule-in and maximum hs-cTnI <5 ng/L or absolute delta hs-cTnT of ≥9 ng/L to rule-in and maximum hs-cTnT <5 ng/L to rule-out has good PPV and sensitivity and can rapidly classify as high or low risk, a large proportion of the patients presenting with chest pain.
Key messages
What is already known on this subject?
The European Society of Cardiology (ESC) had proposed an algorithm to rapidly rule-in acute myocardial infarction (AMI) using both the concentration of the troponin and its absolute and relative changes over 3 h when a high-sensitivity troponin assay is used. The National Institute for Health and Care Excellence recommended troponin concentrations below the 99th percentile of a healthy population be used to rule-out AMI in some subgroups.
What might this study add?
This is the first study to test these algorithms with high-sensitivity troponins I and T. The ESC Working Group on Acute Cardiac Care rule-in algorithm had good specificity and reasonable positive predictive value to rule-in AMI. Successive troponin concentrations <99th percentile had very poor sensitivity to rule-out AMI. Almost all the false negatives were in the subgroups suggested as eligible to use one troponin <99th percentile to rule-out AMI. The study also proposed an alternative, simplified, strategy to use serial troponins to rule-out or rule-in nearly half the patients with high sensitivity and positive predictive value.
How might this impact on clinical practice?
Clinicians should have confidence that the ESC algorithm can be used to rule-in a substantial proportion of patients, although the positive predictive value acceptable may vary from hospital to hospital. However, even two successive troponin concentrations below the 99th percentile should not be used to rule-out AMI.
Acknowledgments
JWP is supported by a Senior Research Fellowship from the Canterbury Medical Research Foundation, Emergency Care Foundation and Canterbury District Health Board. The Queensland Emergency Research Foundation supports LC with a Research Fellowship. The studies were funded by the Heart Foundation of New Zealand (Grant 1457) and Health Research Committee of New Zealand. MPT, LC, WP, PG and DF have accepted travel, accommodation, consulting fees or honoraria from Abbott Laboratories. PAK received funding by Canadian Institutes of Health Research for the RING study with reagents provided via a grant by Abbott Laboratories. PAK has received grants/honorariums/consultant/advisor fees from Abbott Laboratories, Abbott Point of Care, Beckman Coulter, Ortho Clinical Diagnostics, Roche Diagnostics and Siemens Healthcare Diagnostics with respect to cardiac troponin testing. AW receives research funding from the Canadian Institutes of Health Research with reagents provided via a grant by Abbott Laboratories and Roche Diagnostics.
References
Footnotes
Twitter Follow William Parsonage at @LastCardiology, Louise Cullen at @louiseacullen, and John Pickering at @kiwiskiNZ
Contributors Study design: JWP, JHG, LC, MPT. Data collection: all authors participated in data collection. Data analysis: JWP. Outcome adjudication: LC, DF, WP, AW, PAK, MPT. Manuscript draft: JWP, all authors contributed and approved.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement The data used in this study comprised data collected for previous studies (published). De-identified data are available to be shared for joint research projects through contacting the corresponding author.
Linked Articles
- Editorial
- Editorial
- Coronary artery disease
- Heartbeat