Article Text

Statistics from Altmetric.com
Cardiac rehabilitation (CR) is an efficacious and cost-effective intervention in adults with cardiovascular disease in developed countries. The essential elements of CR fall into 4 domains: risk factor management via lifestyle changes such as exercise, diet, and smoking cessation; secondary preventative therapies including lipid-lowering and blood pressure medications; education to improve self-management by patients; and assistance in returning to work. However, CR remains underutilized, even in high-income countries, and there are significant barriers to providing traditional health-care system based CR in low resource settings.
In this issue of Heart, a consensus statement on approaches to CR in low-resource settings is presented by an expert panel using a structured development process based on a systematic literature review (see page 1449). The panel was selected by the International Council on Cardiovascular Prevention and Rehabilitation (ICCPF) and included authors from several countries—Canada, China, India, Iran, Singapore, South Africa, the UK and USA. A detailed table presents 10 specific CR recommendations that can be implemented in any setting, with a modified GRADE level of evidence or indication that this is a consensus based recommendation. There is a detailed discussion of approaches to affordable exercise training.
As Ordunez comments in an editorial (see page 1425): “Clearly, neither CR nor other similar interventions will completely stop the CVD epidemic, but they can contribute to mitigating its consequences and thus saving many lives”. However, “Even when we concur about the reach and comprehensiveness of CR as proposed in its foundational principles, we know that implementation in its original formulation is difficult, and many times unnecessarily complex and unaffordable. To insist on the same approach, despite the evidence that it does not work, may seriously compromise what is truly possible. With a dash of realism and practicality, we can concentrate on what can be sufficiently good—not perfect—and that would allow us to advance further. In this practical and realistic realm, we find interventions that, besides being evidence-based, prioritise primary care, are affordable, are safe, are simple in their delivery and achieve high impact on health outcomes. Let's make CR—and simplified secondary prevention—the art of the possible”.
In patients presenting with an acute coronary syndrome (ACS), risk estimates are important in clinical decision making, with current guidelines recommending earlier aggressive intervention for patients with a moderate to high risk of death. The Global Registry of Acute Coronary Events (GRACE) scores for prediction of 6-month mortality in patients with an ACS is widely used in clinical practice. Patients with chronic obstructive pulmonary disease (COPD) have an increased risk of ACS and have higher mortality rates than non-COPD patients yet are less likely to receive aggressive early intervention. In order to address the apparent under-treatment of ACS in COPD patients, Rothnie and colleagues (see page 1442) evaluated the accuracy of the GRACE score in COPD patients based on data from over 480 thousand patients admitted to UK hospitals with an ACS diagnosis over a 10 year period. They found that the GRACE score underestimated the risk of death in COPD patients (RR 1.29, 95% CI 1.28 to 1.33) but that the predictive value of the GRACE score could be improved either by adding COPD to the model or by multiplying the GRACE score by 1.3 (figure 1).

Proportion of deaths occurring in patients with COPD in each decile of predicted risk for the normal GRACE model, the GRACE model multiplied by 1.3 for patients with COPD, and the MINAP-derived model including COPD. COPD, chronic obstructive pulmonary disease; GRACE, Global Registry of Acute Coronary Events; MINAP, Myocardial Ischaemia National Audit Project.
In the accompanying editorial (see page 1423) Timóteo notes that the diagnostic criteria for COPD are variable, with clinical trials reporting a prevalence of COPD in ACS patients ranging from 5.3 to 18.2 %. She suggests: “Maybe a strategy of early and simple risk stratification would be more appropriate with subsequent stratification considering all additional prognostic comorbidities identified so far, such as diabetes, renal function and COPD. In ST-elevation myocardial infarction, immediate reperfusion therapy is essential and risk stratification is less important. In non-ST elevation ACS, invasive treatment has a wide range of options, between immediate and 72 hours delay. Immediate invasive treatment can be selected by very simple clinical assessment and it does not require risk scoring. For other strategies, we have more time to consider the prognostic impact of other comorbidities. It is thus necessary to understand in real-life clinical practice, what is the real-impact of risk scoring, both in terms of use and in terms of management implications”.
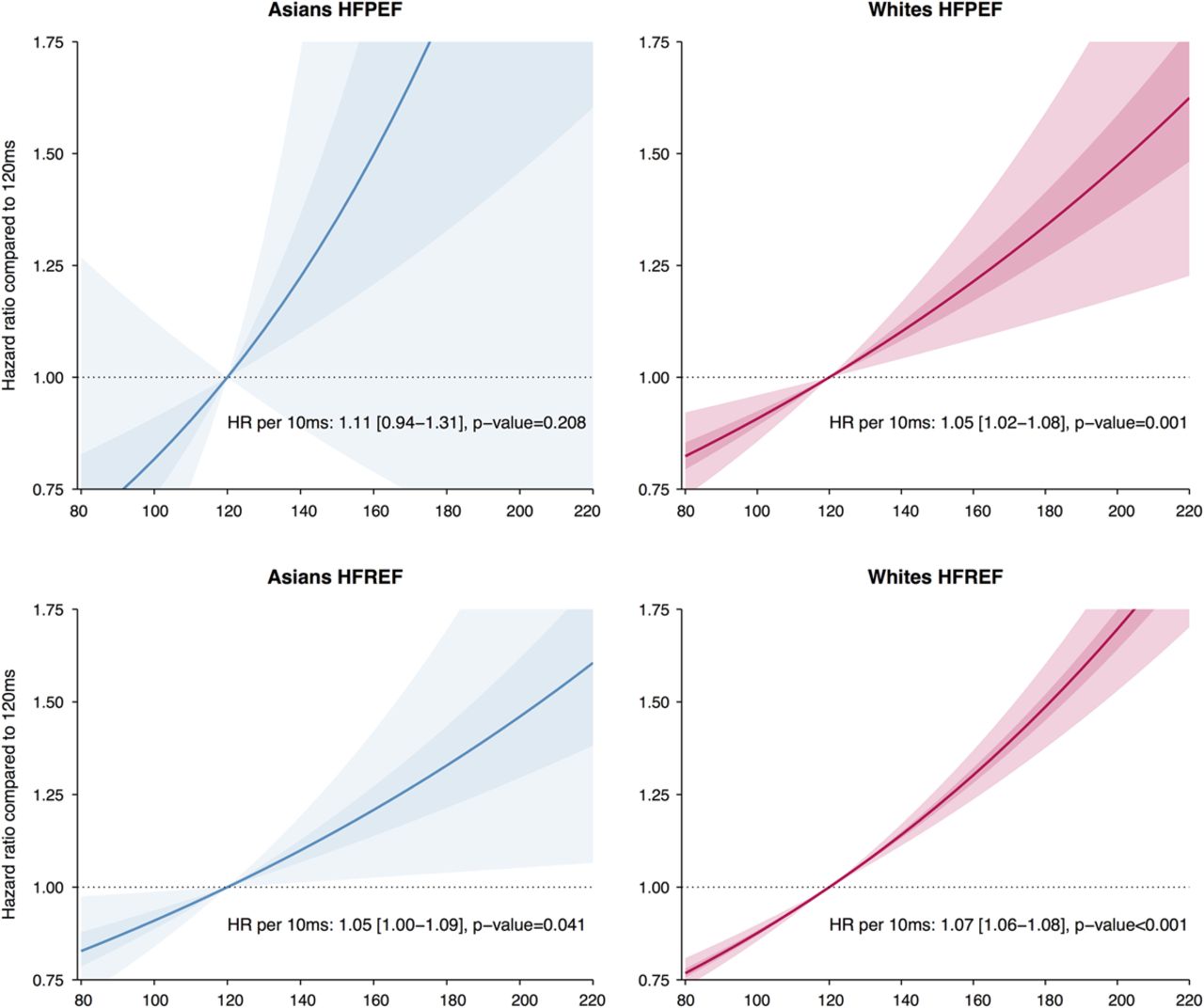
Recommendations for device therapy in heart failure (HF) patients include QRS duration as a key criterion. However, the specific QRS duration values in these guidelines were derived from predominantly white populations. In order to determine if ethnic differences in QRS duration are important, Gijsberts and colleagues (see page 1464) compared the associations between QRS duration, left ventricular ejection fraction (EF) and adverse clinical outcomes (HF hospitalization and death) in 839 Singaporean Asians and 11,221 Swedish white patients. As expected, a lower EF was associated with a longer QRS duration but the slope of this association was steeper in the Asian cohort compared to the white cohort. Although QRS duration was longer in Asians with HF with reduced EF, there was no effect of ethnicity on the association between QRS duration and clinical outcomes. Absolute 2 year event rates for HF hospitalization or death were 40% for a QRS ≤120 ms versus 52% for a QRS >120 ms; the hazard ratio for each 10 ms increase of QRS duration was 1.04 (1.03 to 1.06), p<0.001) (figure 2).
{kind=link}
{kind=link}
Cox regression survival estimates (hazard ratios) are displayed for Asian (in blue, left panel) and white (in red, right panel) patients with heart failure (HF), using 120 ms as the reference value. The top two plots show the relation of QRS duration (QRSd) with outcome for patients with HF with preserved ejection fraction (HFPEF), the bottom two for patients with HF with reduced ejection fraction (HFREF). The outcome is HF hospitalisation or all-cause death. The plotted estimates are derived from univariable analysis. The shaded areas represent the 50% CI (darkest area) and the 95% CI (lighter area). No significant interaction between QRSd and ethnicity was found for outcome (no significant differences between the slopes of the lines for Asians and whites).
In an editorial, Burden (see page 1427) comments: “The article on ethnic differences in the association of QRS duration with ejection fraction (EF) and outcome in heart failure (HF) is a paradigm for epidemiological investigations of ethnic differences in disease”. “For too long observations have been made on Caucasians and for too long these observations have been assumed to be normal, even though access to equal care had been a popular subject for at least the past 20 years”. The Editors of Heart hope to see many more research papers addressing potential ethnic differences in clinical presentation and management of cardiovascular disease in the future.
The current Education in Heart article (see page 1494) discusses percutaneous mechanical circulatory support in management of patients with advanced heart failure (table 1)
Summarising strategy, physiological effects and disadvantages of IABP, Impella, TandemHeart and VA-ECMO
The Image Challenge case (see page 1485)—a 12 year old boy with chest pain and dyspnea—nicely illustrates the differential diagnosis of cardiomyopathy presenting in childhood. Be sure to take a look at the Cardiology in Focus section in this issue (see page 1509) which highlights four young investigators who presented their research at the British Cardiovascular Society Annual Conference in June 2016.
Linked Articles
- Editorial
- Heart failure and cardiomyopathies
- Cardiology in focus
- Cardiac risk factors and prevention
- Editorial
- Image challenge
- Special populations
- Education in Heart
- Editorial