Article Text

Abstract
Objective While vascular dysfunction is well defined in patients with heart failure (HF) with reduced ejection fraction (HFrEF), disease-related alterations in the peripheral vasculature of patients with HF with preserved ejection fraction (HFpEF) are not well characterised. Thus, we sought to test the hypothesis that patients with HFpEF would demonstrate reduced vascular function, at the conduit artery and microvascular levels, compared with controls.
Methods We examined conduit artery function via brachial artery flow-mediated dilation (FMD) and microvascular function via reactive hyperaemia (RH) following 5 min of ischaemia in 24 patients with Class II–IV HFpEF and 24 healthy controls matched for age, sex and brachial artery diameter.
Results FMD was reduced in patients with HFpEF compared with controls (HFpEF: 3.1±0.7%; Controls: 5.1±0.5%, p=0.03). However, shear rate at time of peak brachial artery dilation was lower in patients with HFpEF compared with controls (HFpEF: 42 070±4018/s; Controls: 69 018±9509/s, p=0.01), and when brachial artery FMD was normalised for the shear stimulus, cumulative area-under-the-curve (AUC) at peak dilation, the between-group differences were eliminated (HFpEF: 0.11±0.03%/AUC; Controls: 0.09±0.01%/AUC, p=0.58). RH, assessed as AUC, was lower in patients with HFpEF (HFpEF: 454±35 mL; Controls: 660±63 mL, p<0.01).
Conclusions Collectively, these data suggest that maladaptations at the microvascular level contribute to the pathophysiology of HFpEF, while conduit artery vascular function is not diminished beyond that which occurs with healthy aging.
Statistics from Altmetric.com
Introduction
In many disease states, global reductions in vascular function impact the health of the vascular tree, including conduit vessels and the microcirculation. This is particularly evident in heart failure (HF), a clinical syndrome that presents with numerous symptoms, including impaired cardiac contractile function and systemic vascular dysfunction, which collectively result in the prominent characteristic of severely reduced exercise tolerance and subsequently a reduced quality of life. While HF has classically been characterised by a reduction in ejection fraction, it is now recognised that approximately a half of patients with HF present with normal or ‘preserved’ ejection fraction (HFpEF).1 ,2 Importantly, the prognosis for HFpEF is similar to that of patients with HF with reduced ejection fraction (HFrEF),1 ,3 yet the vascular pathophysiology of this clinical syndrome remains poorly understood.
Vascular dysfunction has been well documented in patients with HFrEF.4–7 In contrast, very few studies have sought to evaluate vascular function in patients with HFpEF, and in the studies that have been undertaken, the results are equivocal. Using a MRI approach, Hundley et al8 reported that flow-mediated dilation (FMD) of the superficial femoral artery was similar between patients with HFpEF and age-matched controls. Subsequent to this, in one of the only studies to assess vascular function using conventional FMD testing, Haykowsky et al9 reported a similar brachial artery FMD in patients with HFpEF compared with healthy, older controls. In contrast, a recent investigation by Farrero et al10 demonstrated reduced brachial artery FMD in patients with HFpEF compared with hypertensive controls without HF. Unfortunately, none of these studies appear to have evaluated the shear stimulus that provokes brachial artery FMD, which is viewed as an important consideration to appropriately interpret the vasodilatory response.11 Thus, whether patients with HFpEF exhibit vascular dysfunction, as assessed by standardised, up-to-date FMD testing guidelines,12 remains uncertain in this patient population.
Though FMD testing has been established as a valuable research tool for non-invasive assessment of vascular function in the conduit vessels, the test provides limited information about vascular function at the level of the microcirculation. Determination of reactive hyperaemia (RH) subsequent to a period of cuff occlusion fills this void, providing an index of microvascular function that is complimentary to conduit vascular function assessed via FMD. There is emerging evidence that RH, assessed via peripheral arterial tonometry (PAT), is reduced in patients with HFpEF,13 ,14 and that this disease-related reduction in RH-PAT is independently correlated with incidence of future cardiovascular events15 and predictive of poor prognosis.14 However, to date, there has not been a study that assessed conduit artery and microvascular function in patients with HFpEF to comprehensively assess peripheral vascular dysfunction in this ever-growing patient population.
Therefore, we sought to determine conduit artery and microvascular function in patients with HFpEF compared with healthy controls using FMD and RH, respectively. We tested the hypothesis that patients with HFpEF would demonstrate reduced vascular function, at the conduit artery and microvascular levels, compared with controls.
Methods
Subjects
Twenty-four patients with Class II–IV HFpEF and 24 healthy control subjects matched for age, sex and brachial diameter volunteered for this study. Patients were recruited from the University of Utah HFpEF Clinic. Within this clinic, patients were screened and included in a manner consistent with the inclusion criteria from the Treatment of Preserved Cardiac Function Heart Failure with an Aldosterone Antagonist (TOPCAT) trial, which included the following criteria: (1) HF defined by the presence of one or more symptoms at the time of screening (paroxysmal nocturnal dyspnea (PND), orthopnoea, dyspnoea on exertion) and one sign (oedema, elevation in jugular venous distention (JVD)) in the previous 12 months; (2) left ventricle ejection fraction ≥45%, (3) controlled systolic blood pressure and (4) either one or more hospitalisations in the previous 12 months for which HF was a major component of hospitalisation, or B-type natriuretic peptide in the previous 60 days ≥100 pg/mL. Diastolic dysfunction on echocardiogram was diagnosed using a lateral wall E/e′ of >10 with a lateral wall e′ of <10. Exclusion criteria for the HFpEF group included significant valvular heart disease, acute atrial fibrillation and body mass index (BMI) >45. All subjects were current non-smokers. The healthy controls were normotensive, free from overt cardiovascular disease, and were not taking any prescription medications. Subjects reported to the laboratory fasted (overnight; >10 h) and had not exercised or consumed caffeine in the 24 h preceding the study. Data collection occurred in a thermoneutral laboratory with subjects resting in the supine position.
Resting haemodynamic and cardiovascular assessments
Prior to the FMD and RH tests, supine resting systolic and diastolic arterial blood pressures were determined by an automated blood pressure monitor (Tango+, Suntech, Morrisville, North Carolina, USA) and mean arterial pressure was calculated as diastolic arterial pressure plus a third arterial pulse pressure. Heart rate was monitored from a standard three-lead ECG interfaced with a data acquisition device (Biopac, Goleta, California, USA).
Measurements of brachial artery FMD and RH
All FMD procedures were performed according to current guidelines.12 Following 20 min of supine rest, baseline measurements of brachial artery diameter and blood velocity were taken for 1 min. Immediately following baseline measurements a blood pressure cuff, placed on the right arm proximal to the elbow and distal to the Doppler probe measurement site, was inflated to a suprasystolic pressure (>250 mm Hg) for 5 min. The cuff was then rapidly deflated and brachial artery diameter and blood velocity measures were obtained continuously for 2 min. RH was quantified as the cumulative brachial artery blood flow (ie, area-under-the-curve, AUC) for the 2 min period post cuff release.
Blood velocity and vessel diameter were assessed with a Logiq 7 ultrasound Doppler system (GE Medical Systems, Milwaukee, Wisconsin, USA) operating in duplex mode. The Logiq 7 was equipped with a linear array transducer operating at an imaging frequency of 14 MHz. Blood velocity was collected with the same transducer at a Doppler frequency of 5 MHz in high-pulsed repetition frequency mode (2–25 kHz). Sample volume was optimised in relation to vessel diameter and centred within the vessel. An angle of insonation of ≤60°16 was achieved for all measurements of blood velocity.
Analyses
Commercially available software (Logiq 7) was used to calculate angle-corrected, time-averaged and intensity-weighted mean blood velocity (Vmean). Brachial artery vasodilation was determined offline from end-diastolic, ECG R-wave triggered images collected from the Logiq 7 using automated edge-detection software (Medical Imaging Applications, Coraville, Iowa, USA). Brachial blood flow was calculated based on the formula: brachial blood flow (mL/min)=(Vmean×π (vessel diameter/2)2×60). FMD was quantified using the greatest increase in brachial artery diameter during the 2 min period following cuff release. Shear rate was calculated as: shear rate (/s)=8 Vmean/arterial diameter. Cumulative AUC values for blood flow and shear rate were integrated via the trapezoid rule and calculated as: (∑(yi(x(i+1)−xi)+(1/2)(y(i+1)−yi)(x(i+1)−xi))).
Blood analysis
A fasting glucose and lipid panel was performed on blood drawn from an antecubital vein in all subjects using standard methods.
Data analysis and statistical approach
Statistical analysis was performed with commercially available software (SigmaStat V.3.10, Systat Software, Point Richmond, California, USA). A Student's unpaired t test was used to determine mean differences for subject characteristics, resting mean arterial pressure and heart rate, as well as FMD and RH AUC. A two-way analysis of variance (group×time) was used to determine differences between groups for RH following cuff release. When a significant main effect was observed, a Holm-Sidak post hoc analysis was performed. Statistical significance was accepted at α≤0.05. Group data are presented as mean±SEM, and exact p values are given unless otherwise noted.
Results
Characteristics of patients with HFpEF and age-matched controls
Anthropometric data and general characteristics for patients and controls are shown in table 1. Disease related characteristics and pharmacological information for the patients with HFpEF are shown in table 2.
Subject characteristics
HFpEF characteristics and medications
Brachial artery FMD
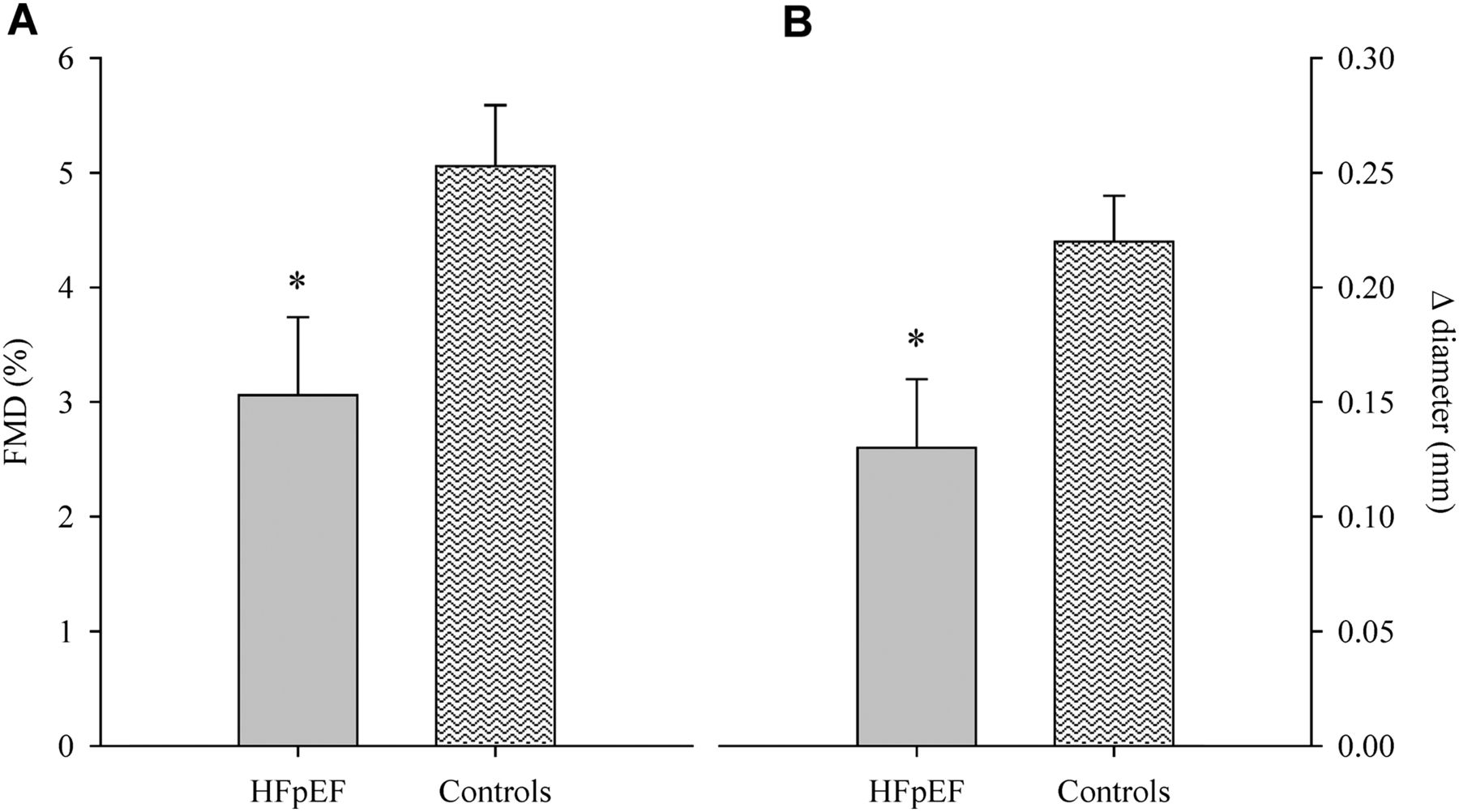
Patients and healthy controls were well matched for baseline brachial artery diameter (p=0.44; table 3). Peak brachial artery diameter following cuff release was not different between groups (p=0.71); however, time to peak was longer in HFpEF compared with controls (p=0.03; table 3). Patients with HFpEF demonstrated a reduction in brachial artery FMD, assessed by the peak percentage (HFpEF: 3.06±0.68% (range−5.9–10.7%, median=3.03%); Controls: 5.06±0.53% (range 0.16–10.49%, median=4.30%), p=0.03; figure 1A) and absolute (HFpEF: 0.13±0.03 mm (range −0.23–0.35 mm, median=0.16 mm); Controls: 0.23±0.12 mm (range 0.01–0.48 mm, median=0.20 mm), p=0.02; figure 1B) change in brachial artery diameter. However, cumulative shear rate at peak dilation was markedly lower in patients compared with controls (p=0.01; table 3), and when brachial artery FMD was normalised for shear rate the differences between groups were eliminated for peak percentage (HFpEF: 0.11±0.03 (range −0.14–0.77, median=0.10); Controls: 0.09±0.01 (range 0.01–0.20, median=0.07), p=0.58; figure 2A) and absolute (HFpEF: 0.005±0.002 (range −0.008–0.420, median=0.004; Controls: 0.004±0.001 (range 0.0005–0.011, median=0.003), p=0.58; figure 2B) change in brachial artery diameter.
Brachial artery flow-mediated dilation

Brachial artery flow-mediated dilation (FMD), expressed as per cent (A) and absolute (B) change from baseline in patients with heart failure with preserved ejection fraction (HFpEF) and healthy individuals (Controls). Data are presented as mean±SE. *Significantly different from controls, p≤0.03.

Brachial artery flow-mediated dilation (FMD) normalised for shear rate area under the curve (SR AUC), expressed as per cent (panel A) and absolute (panel B) change from baseline in patients with heart failure with preserved ejection fraction (HFpEF) and healthy individuals (Controls). Data are presented as mean±SE.
Reactive hyperaemia
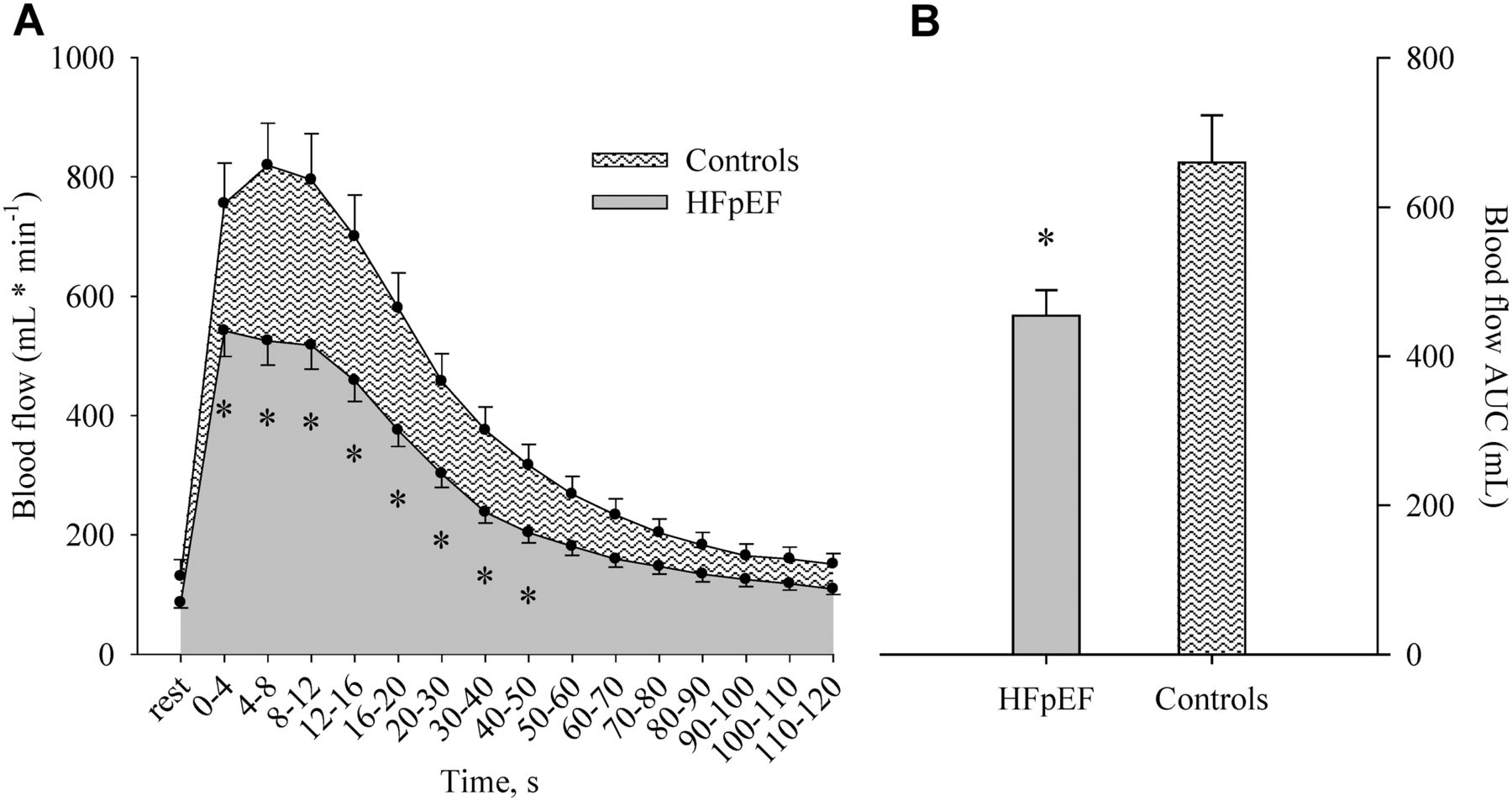
Although baseline brachial artery blood flow was not different between patients with HFpEF and healthy controls (HFpEF: 86±9 mL/min; Controls: 130±28 mL/min, p=0.15; figure 3A), RH was blunted in patients with HFpEF during the initial 50 s following cuff release (p≤0.03; figure 3A). Likewise, RH assessed as AUC was markedly (≈30%) lower in patients with HFpEF relative to controls (HFpEF: 454±35 ml/min (range 169–798 mL/min, median=446 mL/min); Controls: 659±63 mL/min (range 210–798 mL/min, median=631 mL/min), figure 3B).
{kind=link}
{kind=link}
{kind=link}
Postocclusion reactive hyperaemia,expressed as absolute blood flow (panel A) and as blood flow area under the curve (AUC; panel B) in patients with heart failure with preserved ejection fraction (HFpEF) and healthy individuals (Controls). Data are presented as mean±SE. *Significantly different from Controls, p≤0.02.
Discussion
The present investigation sought to comprehensively evaluate peripheral vascular function, at the conduit and microvascular levels, in patients with HFpEF compared with healthy controls. With respect to conduit vessel vascular function, we identified a reduction in brachial artery FMD in patients with HFpEF compared with controls. However, in the HFpEF group, this apparent impairment in FMD was accompanied by a marked (≈40%) reduction in postocclusion shear rate, a haemodynamic variable that is widely viewed as the stimulus for the FMD response. When FMD was normalised for the shear stimulus, the between-group differences were no longer evident, suggesting an absence of overt vascular dysfunction at the conduit level in patients with HFpEF. In contrast, RH, an index of microvascular function, was significantly (≈30%) reduced in patients with HFpEF compared with controls, suggestive of abnormal function in the microcirculation in these patients. In combination, these findings provide new evidence in support of the concept that vascular dysfunction in the conduit vessels is not a requisite feature in the pathophysiology of HFpEF, implicating instead a reduction in peripheral microvascular function that may contribute significantly to clinical status and disease progression in this patient group.
Role of the peripheral vasculature in the pathophysiology of HFpEF
Despite the fact that half of all patients with HF fall into the category of HFpEF, current understanding of the pathophysiology of this pervasive disease remains limited.17 The guidelines for clinical diagnosis of HFpEF continue to evolve, with a focus on echocardiographic evidence of abnormal left ventricular relaxation, filling and diastolic stiffness.18 However, the classic clinical presentation of HFpEF continues to be defined by dyspnoea upon exertion and severe exercise intolerance,19 symptoms that are likely attributable to deficits in cardiac mechanics and peripheral vascular function.20 With respect to the latter, a recent study examining ‘global cardiovascular reserve’ in patients with HFpEF identified a significant correlation between microvascular function (RH) and peak exercise capacity (peak oxygen consumption) and subjective symptoms of fatigue and dyspnoea (Borg scores) during exercise,13 highlighting the relationship between peripheral vasculature function and exercise intolerance in this cohort. Further evidence supporting the concept that disease-related changes in the peripheral circulation may contribute significantly to symptom status in HFpEF comes from Dhakal et al,21 who recently reported significant reductions in peripheral O2 extraction during incremental cycling exercise in patients with HFpEF compared with HFrEF and control groups that the authors attributed to abnormalities in skeletal muscle or peripheral microvascular function. It is from this framework that the present study was undertaken, with the goal of comprehensively evaluating peripheral vascular function in patients with HFpEF in an effort to better define the vascular pathophysiology in this growing patient group.
Conduit vessel vascular function in HFpEF
Although vascular dysfunction, assessed by FMD, has been well documented in patients with HFrEF,4–7 and is an independent risk factor for an increased risk of clinical events and poor prognosis in this cohort,4 much less is known about vascular function in the HFpEF population. In the current study, we observed a reduction in brachial artery FMD in patients with HFpEF compared with controls (figure 1), which initially seemed to indicate impaired conduit vascular function in this patient group. However, assessing the FMD response in this manner does not take into account shear rate, which represents the laminar shear force across the vascular endothelial cells that initiates the FMD response.22 The significance of considering this aspect of the stimulus-response relationship should not be underestimated. Indeed, it has been reported that much of the between-subject variability in FMD testing can be significantly reduced by correcting for the shear stimulus,11 and current guidelines for FMD testing recommend inclusion of this variable to provide a complete characterisation of the FMD response.12 Thus, in view of the substantial reduction in shear rate AUC in patients with HFpEF at the time of peak vasodilation (table 3), we deemed it appropriate to normalise FMD for wall shear rate. Using this approach, the decrement in FMD observed in the patient group with HFpEF was no longer evident (figure 2), suggesting that the ostensible reduction in %FMD (figure 1) was, at least in part, the consequence of a reduced shear stimulus.
The current finding that FMD is not attenuated in patients with HFpEF adds to a very small group of studies that have examined conduit vessel vascular function in this cohort. Using a MRI approach, Hundley et al8 evaluated changes in superficial femoral artery circumference after a 5 min suprasystolic cuff occlusion, and reported that FMD was similar between HFpEF and age-matched controls. Using the more traditional FMD methodology to explore vascular function, Haykowsky et al9 identified similar brachial artery %FMD in patients with HFpEF compared with age-matched, healthy controls, which is in contrast to more recent work from Ferrero et al10 that identified impaired FMD in patients with HFpEF compared with hypertensive controls. With strict adherence to current guidelines regarding FMD testing and careful matching of patients with HFpEF with healthy controls, the present study may be viewed as confirming and extending this previous work, providing new evidence in support of the concept that vascular dysfunction in conduit vessels is not a requisite feature in the pathophysiology of HFpEF.
Microvascular function in HFpEF
Determination of RH subsequent to a period of cuff occlusion provides an index of microvascular function that is complimentary to conduit vascular function assessed via FMD. This haemodynamic assessment has been used in a number of patient groups, and has been identified as an independent predictor of prognosis in patients with HFrEF23 and HFpEF,14 suggesting that RH responses may provide important information for risk stratification and determination of disease progression. In the present study, we determined RH by quantifying the blood flow AUC following a 5 min cuff occlusion of the lower arm, and identified a profound (≈30%) reduction in RH in patients with HFpEF relative to healthy controls (figure 3). This attenuation in the RH response provides clear evidence for the presence of microvascular dysfunction in this patient group that is well beyond the decrement that exists as a consequence of the aging process, which is in agreement with recent work that has used PAT in patients with HFpEF to evaluate RH. Indeed, a recent study by Borlaug et al13 reported a clear reduction in RH index in patients with HFpEF and hypertension compared with healthy age-matched controls, which the authors interpreted as evidence of endothelial dysfunction in these patient groups. Using the more conventional forearm RH technique, findings from the present study build on this previous report, adding additional evidence indicating a clear reduction in microvascular function in patients with HFpEF compared with older, healthy controls.
The observed decrement in peripheral microvascular function in HFpEF may be of particular relevance in the context of the coronary circulation, as there is recent evidence implicating coronary microvascular inflammation as a key player in the aetiology of HFpEF. Paulus and Tschope24 identified a new paradigm for the aetiology of myocardial remodelling and dysfunction in HFpEF that relates inflammation, perhaps as a consequence of comorbidities such as diabetes, to the subsequent production of reactive oxygen species and reduction in nitric oxide (NO) bioavailability in the coronary microcirculation. According to this proposed model, a shift in myocardial redox balance creates an environment that promotes cardiomyocyte hypertrophy and increased collagen deposition, with the functional consequence of diastolic left ventricular dysfunction. In the same manner that flow-mediated vasodilation in the brachial artery has been demonstrated to correlate with coronary artery vasomotor responses,25 it is tempting to speculate that the observed impairment in peripheral microvascular function may provide a surrogate measure for disease-related changes in the coronary microcirculation, and as such, serve as a diagnostic biomarker in this patient group. Additional studies are needed to explore this intriguing possibility.
The distinct vascular pathology of HFpEF
The present findings identifying dysfunction at different sites along the arterial tree helps to further characterise vascular dysfunction in this cohort, and presents another aspect of the HFpEF pathophysiology that differs significantly from HFrEF. Our group has recently demonstrated that patients with HFrEF have reduced FMD, but not post occlusion RH, compared with healthy age-matched controls.7 These data suggest that, in contrast to our current findings in HFpEF, conduit artery impairments alone contribute to the vascular dysfunction in HFrEF. This discrepancy between disease-related changes in the conduit and microvascular segments of the peripheral circulation may partially explain why many of the therapeutic approaches that have proven so successful in patients with HFrEF are somewhat less efficacious in the patient group with HFpEF. Indeed, previous studies in HFrEF have identified the ability of drugs targeting the renin-angiotensin-aldosterone system and HMG-coenzyme A reductase inhibition to improve conduit vascular function.26 ,27 In contrast, the majority of clinical trials targeting these pathways in HFpEF have proven unsuccessful,28–30 though it should be noted that vascular function was not a primary end point in these studies. Thus, while the disparate response to pharmacological treatment is likely due to a host of factors that differ between HFrEF and HFpEF, the distinct manner in which vascular dysfunction manifests in these two cohorts may be worthy of consideration as clinical care of HFpEF continues to evolve.
Experimental considerations
In the present study, we enrolled patients with HFpEF on optimised pharmacotherapy, and no medications were withheld on experimental days. Thus, we cannot exclude the possibility that existing drug therapy may have affected our measurements of vascular function. We also enrolled patients without regards to existing comorbidities such as hypertension, diabetes and coronary artery disease. While this approach may introduce some heterogeneity in terms of baseline parameters, it provided an opportunity to study the pathophysiology of HFpEF in a manner that fairly represents the diverse nature of this patient population. It is acknowledged that the sample size of the present study was relatively small, though a sufficient number of subjects were enrolled to achieve adequate statistical power in the major variables. Finally, we recognise the known variability that is associated with FMD testing, an issue that was somewhat mitigated by the use of standardised testing procedures that conformed to current published guidelines.12
Conclusions
This investigation documents attenuated vascular function in the microcirculation despite an apparent preservation of conduit artery function in patients with HFpEF compared with well-matched, healthy controls. These novel findings highlight a specific site of peripheral vascular dysfunction in this patient group that further characterises this disease.
Key messages
What is already known on this subject?
Vascular function in the peripheral circulation, assessed by flow-mediated dilation (FMD), has been well documented in patients with heart failure (HF) with reduced ejection fraction (HFrEF). However, there is currently no consensus regarding the presence of vascular dysfunction in patients with HF with preserved ejection fraction (HFpEF).
What might this study add?
By investigating vascular function in patients with HFpEF at the conduit and microvascular levels, we have identified a distinct pattern of vascular dysfunction that is specific to the microvasculature. Brachial artery FMD normalised for shear rate was similar between patients with HFpEF and controls, suggesting an absence of overt vascular dysfunction at the conduit level in this cohort. In contrast, reactive hyperaemia, an index of microvascular function, was significantly (≈30%) reduced in patients with HFpEF compared with controls, indicative of abnormal function in the peripheral microcirculation.
How might this impact on clinical practice?
The observed discrepancy between disease-related changes in the conduit and microvascular segments of the peripheral circulation may partially explain why many of the therapeutic approaches that have proven so successful in patients with HFrEF are somewhat less efficacious in the patient group with HFpEF. The results from this study may thus serve to guide the ongoing development of diagnostic algorithms and biomarkers related to vascular function in this patient group.
References
Footnotes
Contributors All authors contributed to study design, implementation and manuscript preparation.
Funding Funded in part by NIH PO1 HL091830, VA RR&D I01RX000182, VA RR&D I21 RX001433, VA RR&D I21 RX001418 and NIH R01 HL118313.
Competing interests None declared.
Patient consent Obtained.
Ethics approval University of Utah and Salt Lake City Veterans Affairs Medical Center Institutional Review Boards.
Provenance and peer review Not commissioned; externally peer reviewed.