Article Text

Abstract
Objective Atrial fibrillation (AF) is a risk factor for stroke and mortality and the prothrombotic state has been linked to inflammation. In this study we evaluated the relationship between inflammatory biomarkers at baseline and future risk of cardiovascular events in the Apixaban for Reduction In Stroke and Other Thromboembolic Events in Atrial Fibrillation (ARISTOTLE) trial.
Methods The ARISTOTLE trial randomised 18 201 patients with AF to apixaban or warfarin. Interleukin 6 (IL-6) and C reactive protein (CRP) were analysed in plasma obtained at randomisation from 14 954 participants, and median follow-up was 1.9 years. Association between quartile groups of IL-6 and CRP and outcomes were analysed by Cox regression adjusted for clinical risk factors and other cardiovascular biomarkers (NT-proBNP, troponin, GDF-15, cystatin C).
Results The IL-6 median level was 2.3 ng/L (IQR 1.5–3.9), median CRP level was 2.2 mg/L (1.0–4.8). IL-6 and CRP were significantly associated with all-cause mortality independent of clinical risk factors and other biomarkers (HR (95% CI) 1.93 (1.57 to 2.37) and 1.49 (1.24 to 1.79), respectively, Q4 vs Q1). IL-6 was associated with myocardial infarction, cardiovascular mortality, and major bleeding beyond clinical risk factors but not in the presence of cardiovascular biomarkers (NT-proBNP, troponin, GDF-15, cystatin C). Neither inflammatory biomarker was associated with stroke/systemic embolism. Risk prediction for stroke, death and major bleeding was not improved by IL-6 or CRP when added to clinical risk factors and the other cardiovascular biomarkers (NT-proBNP, troponin, GDF-15, cystatin C).
Conclusions In patients with AF on anticoagulation, after accounting for clinical risk factors and other biomarkers, biomarkers of inflammation were significantly associated with an increased risk of mortality. However, there were no associations with the risk of stroke or major bleeding.
Trial registration number ClinicalTrials.gov identifier: NCT00412984 post-results.
Statistics from Altmetric.com
Introduction
Atrial fibrillation (AF) constitutes a major risk factor for stroke and death.1 ,2 The potential of biomarkers to improve the prognostication concerning stroke and other cardiovascular events in patients with AF is gaining strength of evidence and clinical promise. In particular the biomarkers of cardiovascular stress and dysfunction such as cardiac troponin (cTn), a marker of myocardial cell damage; N-terminal B-type natriuretic peptide (NT-proBNP), a marker of cardiac dysfunction; and growth-differentiation factor-15 (GDF-15), a marker of inflammation and oxidative stress, have been shown to be strong independent predictors.3–8 Although inflammatory activation has been linked to the occurrence of AF and to a prothrombotic state, the association with subsequent cardiovascular events during treatment with oral anticoagulation has not been fully established.9–14 Prior studies evaluating the relation between inflammation and cardiovascular events in patients with AF have often been exploratory and did not take into account the protective effect of oral anticoagulation. In addition the associations with outcomes have not been fully adjusted for other risk indicators, in particular other cardiovascular biomarkers, which recently have showed to be independent and powerful markers of adverse outcomes in patients with AF.4 In this predefined biomarker study within the Apixaban for Reduction in Stroke and Other Thromboembolic Events in Atrial Fibrillation (ARISTOTLE) trial we assessed the associations between levels of the inflammatory biomarkers interleukin 6 (IL-6) and C reactive protein (CRP) at baseline and clinical outcomes including adjustments for established clinical risk factors and other previously shown to be prognostically significant cardiovascular biomarkers in approximately 15 000 patients with AF treated with either warfarin or apixaban oral anticoagulation.15 ,16 Further, the prognostic information gained by the inflammatory biomarkers in relation to the currently used CHA2DS2VASc (risk model to assess risk of stroke) and HAS-BLED (risk model to asses risk of major bleeding) scores was evaluated, as well as potential interactions with the effects of apixaban as compared with warfarin on all outcomes.
Methods
The ARISTOTLE trial
The details of the ARISTOTLE trial have been published previously.15 ,16 Briefly, ARISTOTLE was a double blind, double-dummy, randomised clinical trial that enrolled 18 201 patients with AF and at least one risk factor for stroke or systemic embolism. Patients were randomised to warfarin (n=9081) or apixaban (n=9120). The primary end point was stroke or systemic embolism. The present biomarker cohort consisted of the first included patients with the inflammatory biomarkers available (IL-6 n=14 954, CRP n=14 884). The ARISTOTLE trial was event driven, participants included in the trial after the extension amendment were not included in the prespecified biomarker study. The median length of follow-up was 1.9 years for the participants with biomarkers available.
End points and clinical risk classification
The end points in this study included stroke or systemic embolism; myocardial infarction; all-cause mortality; cardiovascular death (excluding bleeding and other non-cardiac causes); and major bleeding according to the International Society on Thrombosis and Haemostasis criteria. A blinded clinical events committee using prespecified criteria adjudicated all end points.16 CHADS2 and CHA2DS2VASc scores were calculated for each patient based on the sum of the corresponding risk factors present at randomisation. Patients were classified by CHA2DS2-VASc scores according to 0–1, 2, 3, 4 and ≥5, and major bleeding outcomes were evaluated in relation to the HAS-BLED score classified by 0–1, 2 or ≥3.
Biochemical methods
Venous blood samples were obtained before start of study treatment. Plasma was frozen in aliquots and stored at −70°C until analysed centrally at Uppsala Clinical Research Center, an academic platform for analyses of biomarkers at the Uppsala University Hospital, Uppsala, Sweden. Plasma concentrations of highly sensitive IL-6 were analysed using an ELISA technique, R&D Systems, Minneapolis, USA, and highly sensitive CRP using a particle enhanced immunoturbidimetric assay, Abbott, Abbott Park, Illinois, USA. The methodology of the other cardiovascular biomarkers in the statistical models have been described in detail previously and were analysed as follows: cardiac troponin I with high sensitivity assays using the ARCHITECT i1000SR (Abbott Diagnostics); NT-proBNP with the Cobas Analytics e601; cystatin C with the ARCHITECT ci8200; and GDF-15 with a precommercial assay from ROCHE Diagnostics.5–7 ,17
Statistical analyses
These analyses included the patients who provided blood samples for the biomarker study at randomisation and also had available results of the evaluated biomarkers (IL-6 n=14 954 and CRP n=14 884). Demographics and other baseline characteristics were summarised using frequencies for categorical variables and median and 25th and 75th centiles for continuous variables. For tests of differences among groups, the χ2 test was used for categorical variables and Kruskal-Wallis test was used for continuous variables.
Efficacy analyses included all randomised patients and included all events from randomisation until the efficacy cut-off date (predefined as 30 January 2011). Bleeding analyses were ‘on treatment’ including all randomised patients who received at least one dose of study drug and included all events from receipt of the study drug until 2 days after the last dose of the study drug.
The interaction between treatment and IL-6 or CRP group was analysed using Cox proportional hazards models including treatment group, IL-6/CRP (in quartile groups as well as continuous using restricted cubic splines) and treatment by IL-6/CRP interaction as covariates. The outcomes in relation to IL-6/CRP quartiles were evaluated in multivariable Cox proportional hazards models, sensitivity analyses using continuous variables were also performed. The multivariable analyses included (A) established risk factors (age, sex, body mass index, smoking status, systolic blood pressure, heart rate, AF type (paroxysmal or persistent/permanent), diabetes, history of symptomatic congestive heart failure, previous stroke/systemic embolism/transient ischemic attack (TIA), hypertension, previous myocardial infarction, previous peripheral artery disease/coronary artery bypass surgery (CABG)/percutaneous coronary intervention (PCI), treatment at randomisation with aspirin, ACE inhibitors or angiotensin receptor blockers (ARB), amiodarone, for the major bleeding end point; history of anaemia and history of spontaneous or clinical relevant bleeding were also included), randomised treatment, region, use of warfarin within 7 days before randomisation, use of statin medication within 30 days before randomisation. In a second model (B) other cardiovascular biomarkers were added in continuous natural logarithm form (cardiac troponin I, NT-proBNP, GDF-15 and cystatin C (a marker of renal function)). As a sensitivity analysis a third multivariable Cox proportional hazards model was used that excluded GDF-15 from Model 2 above since GDF-15, similar to IL-6 and CRP, is associated with inflammatory activity. The HRs and 95% CIs, using the group with the lowest IL-6/CRP levels as reference, were reported. We performed likelihood ratio tests to evaluate whether the global model fit improved after the addition of the biomarkers of inflammation. The assumption of proportional hazards for the factors included in the Cox regression analyses was assessed visually using log-cumulative hazard plots. Sensitivity analysis using the Fine-Gray competing risks regression analysis showed consistent results.
The increased discriminative value of IL-6 and CRP was investigated by estimating the C index for survival data18 for models with established risk factors including the components of the CHA2DS2VASc score or HAS-BLED score, without and with biomarker.
Kaplan–Meier estimates of the cumulative risk to the first occurrence of an event were calculated and plotted. All presented event rates were reported per 100 patient-years of follow-up. All statistical tests were two-tailed and performed at the 0.05 significance level. Since all analyses were exploratory, there were no adjustments for multiple comparisons. The Statistics section at Uppsala Clinical Research Center conducted the statistical analyses.
Results
Baseline characteristics and distribution of biomarkers of inflammation
The IL-6 median level was 2.3 (25th centile 1.5, 75th centile 3.9) ng/L, and CRP median level was 2.2 (25th centile 1.0, 75th centile 4.8) ng/L.
Baseline characteristics and medications according to quartiles of IL-6 and CRP, respectively, are shown in table 1. Several variables were associated with increasing levels of biomarkers of inflammation. Increasing IL-6 levels had more pronounced association with older age, persistent or permanent AF, and presence of diabetes, heart failure and renal dysfunction. Increasing CRP levels similarly showed a more pronounced association with presence of diabetes and heart failure, and was in addition inversely related to statin therapy with a somewhat larger proportion on statin therapy in the lowest quartile group.
Demographics and baseline characteristics for groups (A) IL-6 at baseline (B) CRP at baseline
The levels of the cardiovascular biomarkers, cardiac troponin I, NT-proBNP, GDF-15 and cystatin C, increased significantly with rising quartile levels of IL-6 and CRP. Generally, there was a pattern of larger spread of the cardiovascular biomarkers levels between the lowest and highest quartile groups of IL-6, as compared with the respective quartile groups of CRP.
Stroke or systemic embolism
There were a total of 394 stroke or systemic embolism events during follow-up, cumulative hazard rates according to quartile groups of IL-6 and CRP levels are shown in figure 1. The yearly event rates of stroke or systemic embolism ranged from 1.08% in the first quartile group of IL-6 to 1.54% in the highest quartile group. However Cox analyses adjusted for clinical risk factors (Model 1) did not show an independent association (HR 1.26, 95% CI 0.93 to 1.69, p=0.1155) (figure 2A), with similar results for the analyses based on quartile levels of CRP (HR 1.31, 95% CI 0.98 to 1.74, p=0.3347) (figure 2B).

(A and B) Cumulative hazard rates for the primary outcome (stroke or systemic embolism) according to quartile groups at baseline of IL-6 (A) and C reactive protein (CRP) (B).


(A) Associations between quartiles of IL-6 at baseline and cardiovascular events in multivariable analyses. (B) Associations between quartiles of C reactive protein (CRP) at baseline and cardiovascular events in multivariable analyses. *Cox proportional hazards model 1 was adjusted for clinical risk factors and demographic variables**, randomised treatment, prior warfarin status and use of statin medication within 30 days before randomisation. Model 2 included all covariates in Model 1 and cardiovascular and renal biomarkers (NT-proBNP, cardiac troponin I, GDF-15 and cystatin C). **Risk factors and demographic variables: age, sex, body mass index (BMI), smoking status, systolic blood pressure (BP), heart rate, atrial fibrillation (AF), diabetes, heart failure, previous stroke/systemic embolism/TIA, hypertension, previous myocardial infarction (MI), previous peripheral artery disease/CABG/PCI, treatment at randomisation with aspirin, ACE inhibitors or ARB, amiodarone. For bleeding end points, history of anaemia, history of spontaneous or clinically relevant bleeding, haematocrit, drug abuse and abnormal liver function were also included. Sensitivity analyses using continuous variables showed similar results for all outcomes. In a sensitivity analysis for the association between IL-6 (figure 3A) and CRP (figure 3B) and myocardial infarction a reduced set of covariates of clinical risk factors showed similar results (age, sex, BMI, smoking status, systolic BP, diabetes, heart failure, history of MI, use of statin medication within 30 days before randomisation).
Myocardial infarction
There were 149 myocardial infarctions during follow-up. The yearly event rates of myocardial infarction were in range from 0.27% to 0.69%, HR 2.20; 95% CI 1.29 to 3.76, p=0.0138 for the association of IL-6 in adjusted Cox proportional-hazards regression model adjusted for established clinical risk factors (Model 1). The independent association, however, did not remain after extending the multivariable adjustment by adding cardiovascular and renal biomarkers (NT-pro-BNP, cardiac troponin I, GDF-15 and cystatin C) as covariates to the model (figure 2A, Model 2).
For CRP the yearly event rates increased from 0.42% in the lowest quartile group to 0.73% in the highest quartile group, HR 1.78; 95% CI 1.12 to 2.85, p=0.0545. Adding cardiovascular and renal biomarkers as covariates to the model attenuated the results further (p=0.4734) (figure 2B).
All-cause mortality
There were a total of 1064 deaths during follow-up. For IL-6, the yearly event rates increased stepwise from 1.70% in the lowest quartile to 6.84% in the highest quartile, HR 2.84; 95% CI 2.33 to 3.47, p<0.0001 for the effects of IL-6 levels in multivariable analysis adjusted for established clinical risk factors. The result remained significant even in the presence of cardiovascular and renal biomarkers (p<0.0001) (figure 2A).
Similar trends were seen for CRP, the yearly event rates increased from 2.62% in the lowest quartile to 5.55%, HR 2.13; 95% CI 1.78 to 2.55 in the highest quartile group; p<0.0001 for the effects of CRP levels after multivariable adjustment and the association remained significant after adding cardiovascular and renal biomarkers to the model (p=0.0001) (figure 2B).
Cardiovascular mortality
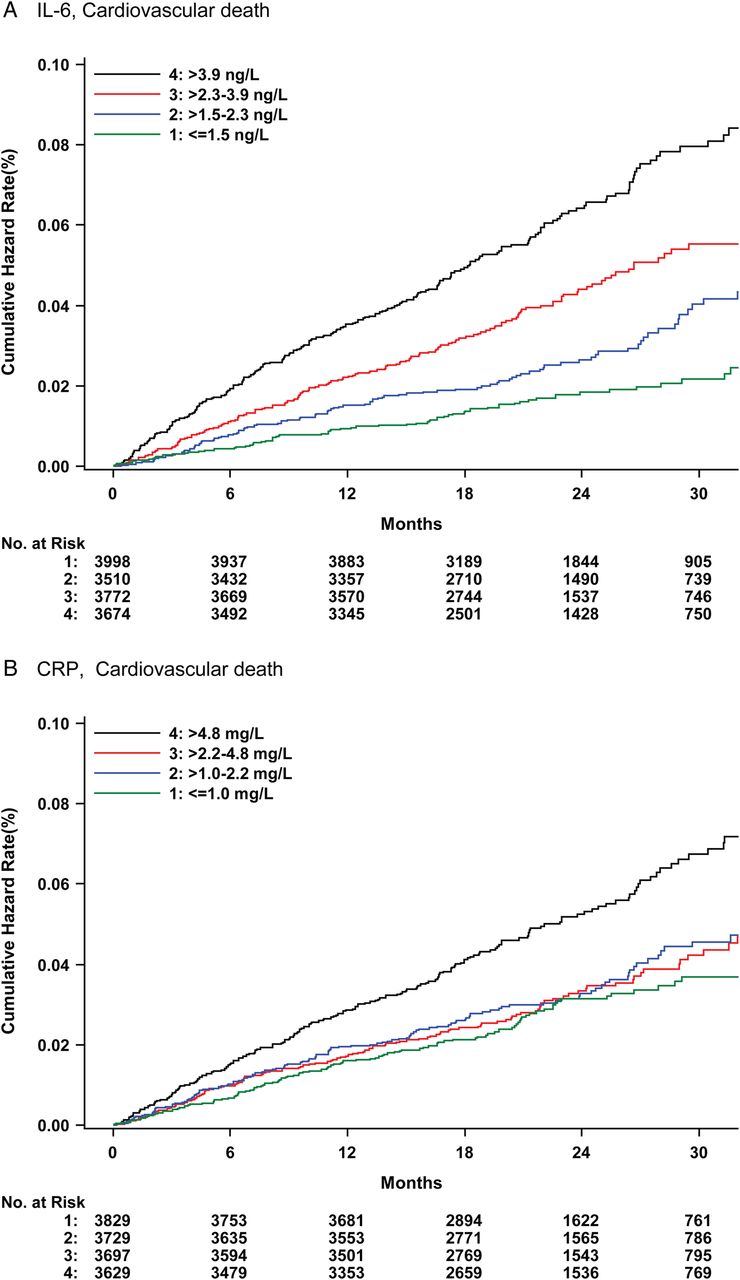
During follow-up 541 patients died from cardiovascular cause, cumulative hazard rates according to quartile groups of IL-6 and CRP levels are shown in figure 3. The yearly event rates of cardiovascular death for the quartiles of IL-6 ranged from 0.91% to 3.21%, HR 2.42; 95% CI 1.83 to 3.19, p<0.0001 for the effects of IL-6 levels in multivariable analysis. The association between IL-6 and cardiovascular mortality was attenuated and did not remain significant after the addition of the cardiovascular and renal biomarkers to the model (figure 2A).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
(A and B) Cumulative hazard rates for cardiovascular mortality according to quartile groups at baseline of IL-6 (A) and C reactive protein (CRP) (B).
For CRP, the yearly event rates ranged from 1.49% to 2.61%, HR 1.71; 95% CI 1.34 to 2.18, p=0.0001 in the multivariable analysis adjusted for established clinical risk factors. The result became non-significant after the addition of cardiovascular and renal biomarkers to the model (figure 3B).
Major bleeding
During follow-up a total of 667 events of major bleeding occurred. The yearly event rates of major bleeding for the quartiles of IL-6 ranged from 1.88% in the lowest to 3.68% in the highest quartile, HR 1.58; 95% CI 1.26 to 1.98, p=0.0006 for the effects of IL-6 levels in multivariable analysis. The association became statistically non-significant in the presence of cardiovascular and renal biomarkers (figure 2A).
For CRP there was no significant association between CRP levels and major bleeds in the multivariable analysis.
Sensitivity analyses excluding GDF-15
GDF-15 also has associations with the inflammatory response, as a sensitivity analysis a third Cox regression model excluding GDF-15 was constructed and used. The sensitivity analyses included established risk factors and the biomarkers cardiac troponin I, NT-proBNP and cystatin C. The results remained similar concerning the associations between the inflammatory biomarkers and all the above outcomes except for IL-6 and its relation with major bleeding and cardiovascular death, respectively. The association between IL-6 and major bleeding was of borderline significance in the absence of GDF-15, HR 1.33; 95% CI 1.05 to 1.68, p=0.087, and non-significant in the full model including GDF-15 (p=0.3224). The relation between IL-6 and cardiovascular mortality showed a similar trend (p value from 0.02 to 0.07 when including GDF-15). The results also remained similar in analyses using continuous levels of the inflammatory biomarkers (see online supplementary figure I).
Outcome in relation to study treatment and biomarker subgroups
There were no relevant interactions between study treatments with apixaban or warfarin in relation to any of the inflammatory biomarker levels for the outcomes either by using quartile groups or continuous levels (see online supplementary figure II and table).
Biomarkers of inflammation for prediction of cardiovascular events in AF and comparison with the CHA2DS2-VASc and HAS-BLED scores
Both biomarkers of inflammation improved the C index for the prediction of all-cause mortality in the models containing the established clinical risk factors (IL-6 from 0.72 to 0.74, and CRP from 0.72 to 0.73, respectively, both p<0.0001). No significant improvements were, however, seen when adding either inflammatory biomarker to the models additionally containing cardiovascular and renal biomarkers (from 0.77 to 0.77 for both).
In comparison with the clinically used stroke risk model, the CHA2DS2VASc score, no improvements were seen by addition of either biomarker of inflammation for prediction of stroke or systemic embolism (table 2). IL-6 and CRP improved the CHA2DS2VASc score for the prediction of all-cause mortality, however concerning cardiovascular death only IL-6 improved the C index slightly in the models containing the other biomarkers (table 2). In relation to the HAS-BLED score concerning major bleeding events, only IL-6 improved the prediction, although not significantly in the model also containing the cardiovascular and renal biomarkers (table 2).
The additive discriminative value of biomarkers of inflammation to the CHA2DS2-VASc and HAS-BLED risk scores
Discussion
The major findings from this prespecified study of a large cohort of patients with AF on oral anticoagulation treatment were that the inflammatory biomarkers IL-6 and CRP were significantly associated with all-cause mortality even after adjustment for clinical factors and the cardiovascular biomarkers NT-proBNP, cardiac troponin I, GDF-15 and cystatin C. IL-6 also showed associations with myocardial infarction, major bleeding and cardiovascular mortality, when adjusting for established risk factors. These associations, however, did not remain significant in the presence of the other cardiovascular biomarkers. Neither inflammatory biomarker was associated with stroke or systemic embolism in patients with AF treated with oral anticoagulation. Concerning risk prediction in this setting, the inflammatory biomarkers did not confer improvements to the prognostication of mortality in the presence of clinical risk factors and other biomarkers. Neither the clinically used CHA2DS2-VASc nor the HAS-BLED risk score were improved by the addition of these specific inflammatory biomarkers for the prediction of stroke or major bleeding, in patients with AF on oral anticoagulation.
Although the evidence is persuasive that inflammatory processes play a pivotal role in the development and progression of atherosclerosis and cardiovascular disease, inflammatory biomarkers have to date, somewhat surprisingly, only demonstrated a moderate incremental value concerning risk prediction.19 ,20 In AF, inflammatory activity has been associated with the pathogenesis of the arrhythmia and the subsequent structural remodelling as a consequence.9 ,21 Similar to the findings in the present study, levels of inflammatory activity have previously been described to increase in tandem with an accumulation of stroke risk factors in patients with AF. However, the independent association of biomarkers of inflammatory activity with stroke risk has so far been inconsistent.10 ,11 ,13 Prior studies consisting of either small cohorts or retrospective data has primarily described associations with mortality or different thromboembolic composite outcomes. Another important notion is that the majority of these studies have been in patients on oral anticoagulation, and there might be differences between patients with and without oral anticoagulation. In recent results from the Randomized Evaluation of Long-Term Anticoagulation Therapy (RE-LY) biomarker substudy, the inflammatory biomarker IL-6 was described to have an independent association with stroke risk when adjusting for clinical risk factors; it was, however, significantly attenuated and became non-significant by addition of cardiac biomarkers (troponin and NT-proBNP) to the model.22 In the present ARISTOTLE biomarker study on patients with AF treated with oral anticoagulation, neither IL-6 nor CRP demonstrated an independent association with stroke risk even in the models solely adjusting for the clinical risk factors. The discrepancy may be due to some dissimilarities between the two cohorts such as an older age in the RE-LY cohort, although probably mainly due to a more extensive adjustment of risk factors and risk indicators permitted by the larger numbers of events and total number of participants in the ARISTOTLE biomarker cohort (IL-6 n=14 954, CRP n=14 884) as compared with the RE-LY biomarker cohort (n=6187). Importantly, in the models further adjusting for the other cardiovascular biomarkers the results were congruent in the ARISTOTLE and RE-LY biomarker cohorts and did indeed not show an independent association with stroke or systemic embolism in patients with AF. Concerning mortality outcomes, the association between biomarkers of inflammation and all-cause mortality has been more consistent in prior publications and is in alignment with the findings in the present study based upon the Cox analyses. However, with regards to the added value of inflammatory biomarkers for risk prediction evaluated by C index, the knowledge is limited and has previously not been performed in fully adjusted models and was not significant in the present study, which therefore adds novel insights. The association between biomarkers of inflammation and risk of major bleeding has been less intensively studied. In patients with acute coronary syndromes, bleeding events have been associated with increasing levels of IL-6 and CRP.23 In patients with AF in the RE-LY trial an independent association between IL-6 levels and major bleeding, however not for CRP, was showed.22 The results from the present study demonstrated IL-6 to be a risk marker of major bleeding independent of clinical risk factors, however, contrary to the finding from RE-LY, not when further adjusting for the other biomarkers. Apart from a more extensive adjustment of risk factors and indicators for bleeding in the model used in the present study, as compared with the model in the RE-LY substudy, there are also key differences in the cardiovascular biomarkers used between the models. In the present study GDF-15, a marker of inflammation and oxidative stress, was included in the biomarker adjusted model which recently has been shown to be a powerful independent risk marker for major bleeding in patients with AF.7 The effect of GDF-15 on the association between IL-6 and major bleeding was also evident in the performed sensitivity analyses, in which GDF-15 clearly diminished the significance of IL-6 when added to the model.
Based on the results from this large, high quality prospective randomised trial data set of almost 15 000 patients treated with oral anticoagulation, the usefulness of IL-6 or CRP for improved prognostication in patients with AF seems limited. The indications of inflammatory activity as a component of the AF disease and its associations to a prothrombotic state and potential relation to worse outcomes has made inflammatory activity an interesting area of investigation and prospective treatment target.24–27 However, unspecific indicators of inflammatory activity such as CRP or IL-6 do not seem to be useful to include as routine biomarkers to improve risk stratification in patients with AF as neither of these two biomarkers improved the prediction of stroke nor major bleedings when added to the clinically used scores. Although the addition of IL-6 to the HAS-BLED score significantly improved the prediction of major bleeding, the improvement became non-significant when added to a model consisting of the HAS-BLED score together with more widely available cardiovascular and renal biomarkers. The inflammatory biomarkers, in particular IL-6, may however potentially be useful in the prognostication of mortality in patients with AF. Although the exact mechanism is not clear, the results suggests that systemic inflammatory activity in patients with AF play a role in fatal outcomes and most likely reflect an overall burden of disease, similar to findings from other patient populations.28
Apixaban has previously demonstrated superior efficacy and safety in comparison with warfarin concerning risk of stroke or systemic embolism, all-cause mortality and major bleeding, respectively.15 No relevant interactions were however seen between study treatment with apixaban or warfarin in relation to IL-6 or CRP levels for any of the outcomes.
Strengths and limitations
This study has some strengths and limitations that merit mentioning. The data are from a clinical trial cohort of patients with AF and at least one risk factor for stroke and the results may therefore not be completely generalisable to the general AF population. Further, the associations between the biomarkers of inflammation and outcome events, in particular stroke, may be influenced by all participants receiving oral anticoagulation. The study is, however, based on results from the largest cohort till date of patients with AF and biomarkers which were closely monitored, with all outcomes rigorously adjudicated, in a prospective randomised trial with a prespecified comprehensive analysis encompassing several other important cardiovascular biomarkers in the evaluation which together adds robustness to the presented analyses.
Conclusions
In patients with AF on anticoagulation, baseline levels of IL-6 and CRP were independently associated with an increased risk of mortality; however, no significant association was observed for the risk of stroke. IL-6 was also found to be related to the risk of major bleeding and myocardial infarction, although not independent of other cardiovascular biomarkers such as cardiac troponin, NT-proBNP and GDF-15. In patients on oral anticoagulation neither inflammatory biomarker improved risk prediction significantly on top of established clinical risk factors and other cardiovascular biomarkers. There was no interaction between the risk stratification by inflammatory level and the superior efficacy and safety of apixaban as compared with warfarin.
Key messages
What is already known on this subject?
Inflammatory activity is associated with the pathogenesis of atrial fibrillation (AF) and the inflammatory levels increase in tandem with an accumulation of stroke risk factors. The independent association of inflammatory biomarkers with stroke and other cardiovascular events has, however, so far been inconsistent in the AF population.
What might this study add?
This biomarker study within the Apixaban for Reduction In Stroke and Other Thromboembolic Events in Atrial Fibrillation (ARISTOTLE) trial adds unique information of the prognostic value of inflammatory biomarkers in patients with AF on oral anticoagulation. This was achieved by prespecified comprehensive analyses in the largest cohort till date of almost 15 000 patients from a prospective randomised trial and by including several other important cardiovascular biomarkers in the evaluation.
How might this impact on clinical practice?
In patients with AF on anticoagulation, biomarkers of inflammation were associated with an increased risk of mortality beyond clinical risk factors and other biomarkers. However, there were no independent associations with the risk of stroke or major bleeding. The prognostic value of inflammatory biomarkers in patients with AF on oral anticoagulation therefore seems limited.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online supplement
Footnotes
Contributors Members of the Executive (JHA, BG, CBG, MH, JH, EMH and LW), Steering (JH), Clinical Events (JHA, EMH and RDL) and Biomarker Substudy (BG, CBG, MH, JH, EMH, AS and LW) committees designed the ARISTOTLE trial and the Biomarker Substudy programme and supervised the conduct as previously published. All coauthors were involved in the planning and data interpretation of the analyses for this substudy. The statistical analyses in this substudy were performed at Uppsala Clinical Research Center, Uppsala University, Sweden (UA) using R V.3. All authors had full access to the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. The first draft of the manuscript was written by the corresponding author (ZH), which thereafter was revised by all coauthors until agreement to submit was reached.
Funding The trial was funded by Bristol-Myers Squibb, Princeton, New Jersey, USA and Pfizer, New York, USA and coordinated by the Duke Clinical Research Institute, Durham, North Carolina, USA and Uppsala Clinical Research Center, Uppsala, Sweden. Roche Diagnostics, Rotkreuz, Switzerland, provided the precommercial assay of GDF-15 free of charge.
Competing interests ZH: Institutional research grant and lecture fees from Boehringer Ingelheim; institutional research grant from Bristol-Myers Squibb/Pfizer. JA: Institutional research grant from Boehringer-Ingelheim, Bristol-Myers Squibb/Pfizer. UA: Institutional research grant from Bristol-Myers Squibb/Pfizer. JHA: Institutional research grant, consulting fees and honoraria from Bristol-Myers Squibb; consulting fees and honoraria from Portola Pharmaceuticals, Sohmalution; institutional research grants from Boehringer Ingelheim, CSL Behring, National Institutes of Health, Regado Biosciences, Sanofi, Tenax Therapeutics, Vivus Pharmaceuticals. BG: Consultant/advisory board fees from Medtronic, Baxter Healthcare Corporation, Cardiovascular Research Foundation, St Jude Medical, Ortho-McNeil-Janssen Scientific Affairs, Teva Pharmaceuticals, Boston Scientific, Pfizer Limited. CBG: grants and personal fees from GlaxoSmithKline, Boehringer Ingelheim, Bristol-Myers Squibb, Pfizer, Sanofi-Aventis, Takeda, The Medicines Company, Janssen, Bayer; grants from Medtronics Foundation, Merck & Co, Armetheon; personal fees from Hoffmann-La Roche, Lilly, AstraZeneca, Daiichi Sankyo, Ross Medical Corporation, Salix Pharmaceuticals, Gilead. MH: Employee of and has stock ownership in Bristol-Myers Squibb. JH: Nothing to disclose. EMH: Advisory board member and symposium lecture fees from Bayer, Boehringer Ingelheim, Bristol-Myers Squibb; advisory board member for Daiichi Sankyo, Janssen, Medtronic, Pfizer. RDL: Institutional grant support and consulting fees from Bristol-Myers Squibb; institutional grant support from GlaxoSmithKline; consulting fees from Bayer, Boehringer Ingleheim, Pfizer. AS: Institutional research grants from Bristol-Myers Squibb/Pfizer, AstraZeneca, Boehringer-Ingelheim, GlaxoSmithKline. LW: institutional research grants, consultancy fees, travel support and lecture fees from AstraZeneca, Bristol-Myers Squibb/Pfizer, GlaxoSmithKline; institutional research grants, consultancy fees, and lecture fees from Boehringer Ingelheim; institutional research grants from Merck & Co, Roche; consultancy fees from Abbott; honoraria from GlaxoSmithKline; holds two patents involving GDF-15.
Patient consent Obtained.
Ethics approval The Ethics Committees at all sites.
Provenance and peer review Not commissioned; externally peer reviewed.