Article Text

Abstract
Transthoracic echocardiography (TTE) is a useful method for non-invasive screening of patients at risk of pulmonary hypertension (PH). Since TTE often serves as the initial study before invasive cardiac catheterisation, misinterpretation of TTE variables may lead to missed or delayed diagnosis with devastating consequences for the patients, or unnecessary invasive diagnostics that have inheriting risks. Due to the heterogeneous anatomy in congenital heart disease, particularly the assessment of myocardial function in children with PH is challenging. Here, we present recommendations on the use of TTE in the screening, diagnosis and follow-up of patients with PH, and discuss the limitations of this non-invasive imaging technique. This expert consensus statement focuses on key TTE variables used to determine the pressure in the pulmonary artery, myocardial contractility and systolic and diastolic function of the RV and LV. A particular focus is on the TTE assessment of RV function and geometry. According to the published data on the application of TTE in PH in childhood, we suggest a structured approach for non-invasive assessment of pulmonary artery pressure and myocardial function that may help to identify patients with early ventricular deterioration and their response to advanced pharmacotherapy. In addition to clinical and biochemical markers, serial examination of patients with PH using a standardised TTE approach, determining conventional and several more novel echocardiographic variables may allow early diagnosis and treatment, better recognition of disease progression and guide tailored therapy.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Video abstract
Introduction
Pulmonary hypertension (PH) in children is commonly characterised by the presence of precapillary PH due to increased pulmonary vascular resistance (PVR) and impaired blood flow just proximal to the pulmonary capillaries.1 Chronically elevated PVR leads to RV pressure overload and ultimately to RV failure. In children, pulmonary arterial hypertension (PAH) (ie, group 1 PAH of the Nice classification 20132) is usually a severe, refractory, progressive and lifelong disease.
Transthoracic echocardiography (TTE) is the most important, most accessible non-invasive diagnostic procedure not only for the initial confirmation of suspected PH but also for screening children at increased risk for PH development and possible systolic RV dysfunction. TTE is also important for the clinical follow-up after change of treatment or clinical condition. Due to variable body size and different causal pathophysiology, TTE variables used for the assessment of paediatric PH can have different reference ranges and variable impact on the accuracy of diagnosis in children versus adults with PH.3
Here, we review the principles and applications of TTE in patients with PH, thereby focusing on children with pulmonary hypertensive vascular disease, and provide practical recommendations for its use. We emphasise non-invasive variables that may provide insight into the pathophysiology and course of PH along with invasive haemodynamic assessment. Combining commonly used and novel TTE variables and modalities to assess RV function and geometry in paediatric PH may help the clinician avoid some of the pitfalls of the TTE examination, especially the overreliance on the Doppler pressure estimation in the initial diagnosis and serial assessment of children with PH. In general, overreliance on any single TTE variable, and especially RV and PA pressure estimation, detracts from the overall diagnostic validity of the TTE examination.
Methods
The recommendations given in table 1 relate to the grading system currently suggested by the European Society of Cardiology (ESC) and the American Heart Association (AHA), and was based on paediatric data only (class, level of evidence). The grading and voting process within the writing group is outlined in the executive summary of this online supplement.
Recommendations on transthoracic echocardiography (TTE) in paediatric pulmonary hypertension
Echocardiographic features of RV in paediatric PH
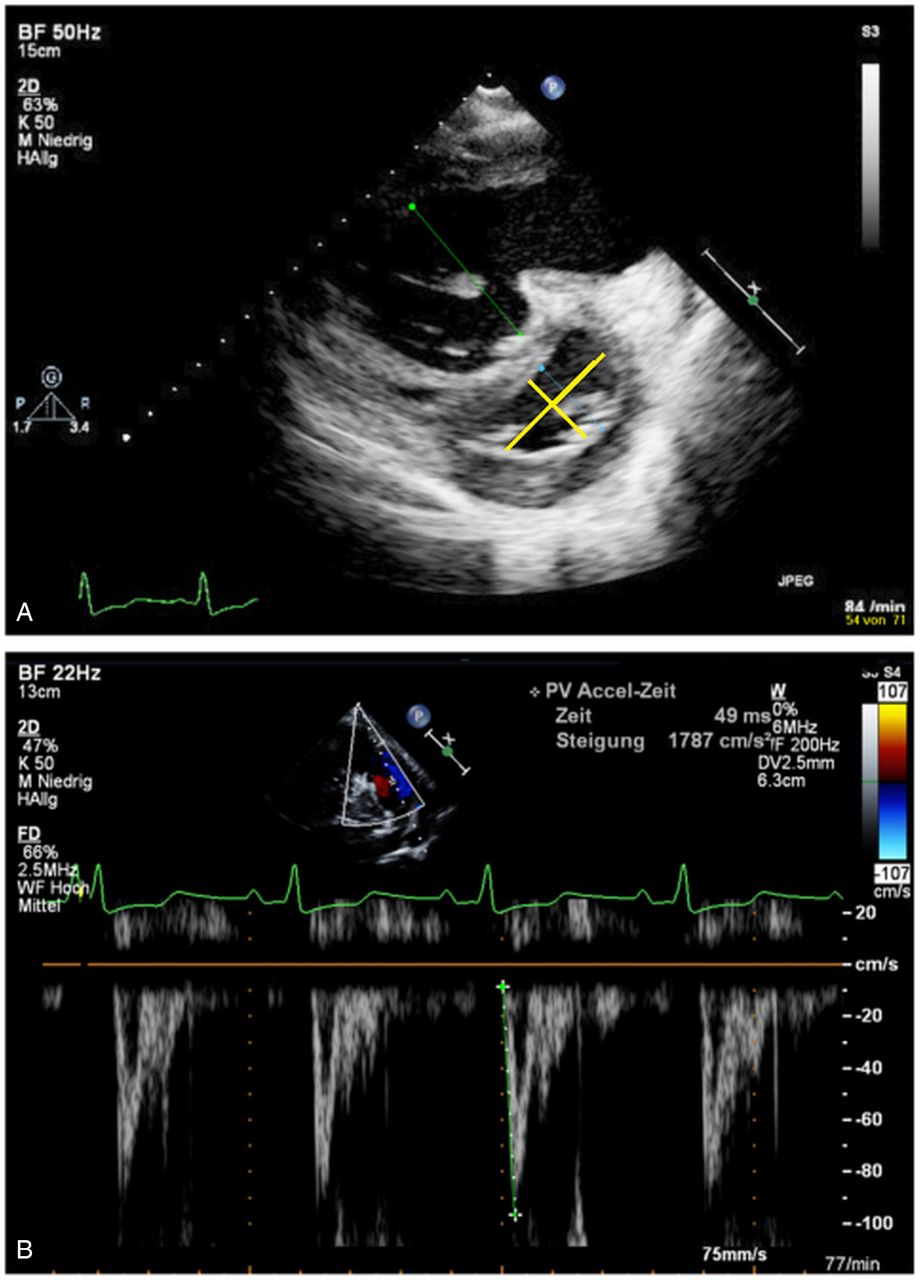
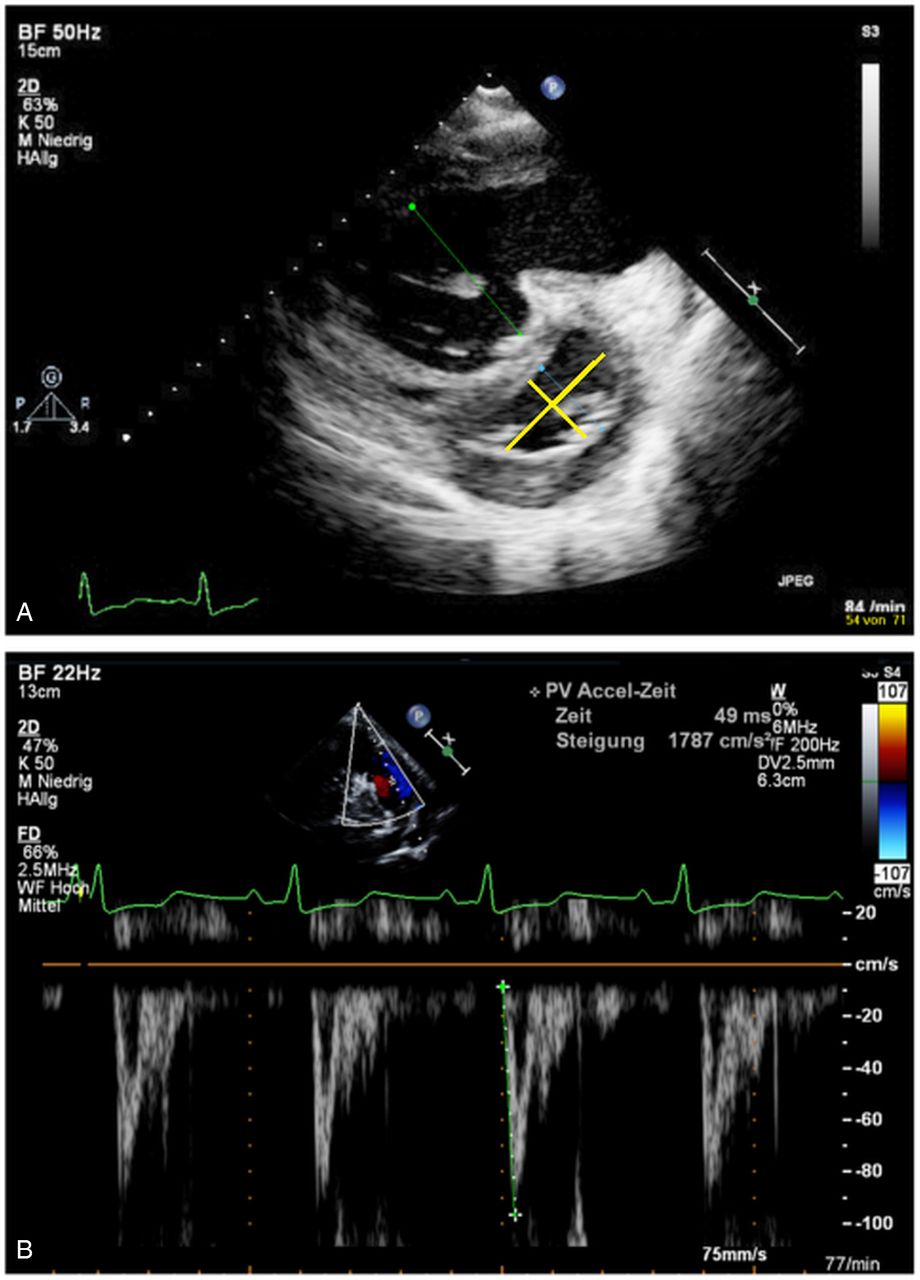
An echocardiographic study of a child with a suspected/confirmed PH should include the assessment of the following variables: estimation of the systolic pulmonary artery pressure (PAP), by estimating RV systolic pressure (RVSP) through the measurement of the velocity of the tricuspid regurgitation (TR) jet by continuous wave (CW)-Doppler (figure 1A), the estimation of mean PAP and end-diastolic PAP through CW-Doppler velocity measurement of the pulmonary regurgitation (PR) jet in the parasternal short-axis view (figure 1B), RV longitudinal systolic function determination (figure 2A), RV strain and strain rate measurements (most commonly longitudinal strain from apical four-chamber view), RV volume determination by 3D echocardiography, measurement of the RV systolic to diastolic duration ratio (TR in apical four-chamber view; figure 2B), determine tissue Doppler velocities (figure 2C), measurement of the RV/LV diameter ratio and eccentricity index (figure 3A), and determination of the PA acceleration time (PAAT) (figure 3B).

Estimation of RV and PA pressure using continuous wave (CW)-Doppler echocardiography. (A) Estimation of RV systolic pressure through the measurement of the velocity of the tricuspid regurgitation (TR) jet using CW-Doppler in the apical four-chamber view. The white broken line indicates CW-Doppler cursor placement at TR. The peak TR velocity is above 4 m/s, thus estimating an increased pressure gradient between RV and right atrium (RA). This added to an estimated RA pressure (v wave) will estimate the systolic RV pressure that is approximately the systolic pulmonary artery pressure (PAP) (in the absence of pulmonary stenosis). (B) Estimation of mean PAP through CW-Doppler of the pulmonary regurgitation (PR) jet in the parasternal short-axis view. The white broken line indicates CW-Doppler cursor placement at PR. The mean PAP can be seen as the PR gradient with a markedly increased value of 48 mm Hg compared with normal values (<25 mm Hg). The end-diastolic regurgitation velocity (yellow line) is 2.5 m/s. When added to an estimated mean RA pressure of 10 mm Hg, this suggests a diastolic PA pressure (dPAP) of 35 mm Hg.

Measurements in the apical four-chamber view. (A) The white broken line indicates M-Mode cursor placement at the tricuspid lateral annulus. Representative M-mode image of the tricuspid annular plane systolic excursion (TAPSE) in a 17-year-old patient with pulmonary hypertension (PH) secondary to congenital heart disease with a decreased TAPSE. The white broken line shows the decreased TAPSE value and flat course of the excursion. Note the dilatation of the right cavities. (B) Doppler-derived tricuspid regurgitation time (TR) interval ratio of systolic (S) duration to diastolic (D) duration (S/D). The ratio of S/D duration was calculated by dividing the duration of the TR spectral Doppler flow pattern by the time interval of the cardiac cycle that did not include TR. Systolic and diastolic duration using TR duration was measured by continuous wave (CW)-Doppler from the apical four-chamber view to calculate the S/D ratio. The red lines show the systolic duration, and the yellow lines show the diastolic duration. (C) RV tissue Doppler imaging (TDI) along the basal long axis of the RV free wall with the cursor through the lateral tricuspid annulus. Example of a pulsed-wave TDI traced parameters tricuspid annular peak systolic velocity (S′), peak early diastolic velocity (E′) and peak late (atrial) diastolic velocity (A′) in a 10-year-old patient with PH. Note the reduced values on all sites and the dilated right cavities. S′, tricuspid annular peak systolic velocity; E′, peak early diastolic velocity; A′, peak diastolic velocity during atrial contraction.
{kind=link}
{kind=link}
{kind=link}
Measurements in the parasternal short-axis view. (A) Parasternal short-axis view of RV and LV. D-shaped LV and enlarged RV (due to flattening of the interventricular septum). The end-systolic septal bowing is typical for pulmonary hypertension (PH). Remodelling of left and right cavities in a 14-year-old patient with severe idiopathic PH (iPH). The RV/LV ratio was derived from RV diameter and LV diameter at end systole. The green line marks the severe dilatation of RV with LV compression shown by the blue line. The longer yellow line represents the anterior–posterior dimension and the shorter yellow line the septal–lateral dimension to determine the eccentricity index. (B) Parasternal short-axis view. Representative pulmonary artery flow velocity profile in the mean pulmonary artery in a 9-year-old patient with iPH. Note the rapid acceleration to peak flow velocity in early systole marked by the green line, with a rapid deceleration to a nadir in mid systole, followed by a secondary increase in flow velocity in late systole. Pulmonary artery acceleration time of 49 ms is reduced compared with normal subjects.
The abnormal pressure elevation in the RV leads to flattening of the interventricular septum with LV appearing D-shaped with reduced volumes but preserved global systolic function.3 Of course, standard evaluation of the left heart, including LV systolic function (LVEF, FS), longitudinal systolic LV function (mitral annular plane systolic excursion (MAPSE)), and inflow and outflow Doppler of all valves, should complete a comprehensive TTE study for PH to unravel concomitant LV dysfunction and/or adverse RV–LV interactions.
The validity of transthoracic RV echocardiography is still limited in paediatric clinical practice by the lack of standardisation. Current recommendations on echocardiographic evaluation of the paediatric right heart may help to overcome this problem.4 A list of the main diagnostic investigations, and main advantages and disadvantages of these echocardiographic variables, is provided in tables 2 and 3.
Echocardiographic investigations in suspected or confirmed paediatric PH
Advantages and disadvantages of (surrogate) echocardiographic measurements in PH
The presence of a pericardial effusion (PE) found by TTE is prognostic and indicates poorer survival in patients with PH.5 In adult patients with no PE at the diagnosis ‘PH’, the appearance of a new moderate or larger PE has been shown to be associated with increased mortality; however, mortality was not increased when only a small PE developed.6 Currently, no data on the significance of PE on mortality in paediatric PH are available. Nevertheless, exact evaluation for PE should be considered in the evaluation of paediatric PH.
Right atrium (RA) enlargement plus interatrial septal bowing from right to left indicates poor RV compliance or increased mean RA pressure (RAP), or both in adults.7 An RA area >20 cm2 measured from the apical four-chamber view has been shown to be abnormal, and an RA area >27 cm2 was associated with a higher rate of transplantation or death in adults with idiopathic PAH (IPAH).7 The RA size has been demonstrated to be positively related to greater RV dimensions.8 Currently, no data on RA enlargement in paediatric PH are available. However, determination of RA size may be considered in the evaluation of paediatric PH.
TTE findings of PH alone (eg, elevated TR jet velocity, decreased tricuspid annular plane systolic excursion (TAPSE)) are not sufficient to establish the diagnosis PH and to initiate so-called specific pharmacotherapy—unless the patient is too sick/unstable to undergo cardiac catheterisation,9 but deserves the immediate initiation of (usually parenteral prostanoid) therapy (WHO functional class III/IV).
Estimation of PAP
The estimation of systolic PAP (PASP) is based on the peak velocity of the jet of TR. The simplified Bernoulli equation and CW-Doppler is used to assess velocity within TR jet [RVSP= PASP=4×(TRV)2+RA v wave=approximately 4×(TR)2+mean RAP] describes the relationship of TR and RVSP as a surrogate of PASP in the absence of an RV outflow tract (OT) obstruction (figure 1A). The mean (m)PAP can be calculated from the PA systolic pressure (≈ RVSP) as the mean PAP=0.61×PASP+2 mm Hg. The latter formula could allow the use of Doppler measurements to raise the suspicion for PH, applying the accepted definition of paediatric PH as a mean PAP >25 mm Hg and a PVR index >3.0 Wood units m2 for biventricular circulations.10 Usually TR velocity (TRV) values >3.4 m/s, corresponding to a PASP >50 mm Hg at rest, make PAH highly likely in adults. Velocity measurements are dependent on the angle of interrogation (goal: Doppler sample in line with the blood flow). A limitation of the CW-Doppler velocity measurements includes cases with severe TR when the PASP usually is underestimated. Inappropriate estimation of RAP and the use of inadequate Doppler signals were identified as frequent pitfalls in TTE that led to incorrect PAP estimations.11
If PR can be interrogated with CW-Doppler, mPAP and end-diastolic PA pressure can be estimated from the maximum (early diastolic) and minimum (end-diastolic) PR velocity (PRV) using the simplified Bernoulli equation [mPAP=4×(max. diastolic PRV)2+RA v wave=4×(PRV)2+mean RAP]; [diastolic PAP=4× (max. diastolic PRV)2+RA v wave=4×(min. end-diastolic PRV)2+mean RAP].12 Mean PAP and end-diastolic pressure can also be routinely used in the diagnosis and follow-up of paediatric PH, especially when TRV is unreliable. In 2D echocardiography, the pulmonary valve can best be imaged in the parasternal short-axis view at the level of the aortic valve (figure 1B). TRV and PRV should be taken from multiple views searching for the best envelope and maximal velocity.
RV longitudinal systolic function (TAPSE)
TAPSE, a variable of longitudinal systolic RV function, reflects the longitudinal excursion of the tricuspid annulus towards the apex and is measured with M-mode in the apical four-chamber view13 (Figure 2A). TAPSE appears to be a developmentally dependent variable as values increase from preterm infants to healthy adolescents with growth and ageing.14 Reference values for TAPSE are available for adults and in children.15 ,16 Abnormal TAPSE is related to abnormal RV function in adults. For every 1 mm decrease in TAPSE, the unadjusted risk of death increased by 17% in adult patients with PH.17 With increasing age of paediatric and young adult patients with PH, that is, the longer the RV is exposed to severe pressure overload and environmental factors associated with PH, TAPSE values fade and become significantly decreased compared with age-matched controls.18 Despite the difficulty in determining the exact onset of PH in the individual patient, a decreased TAPSE value (z-score <−2) may point towards an early decline of global RV systolic function. Of note, TAPSE does not take into account segmental RV function and contractility, or the important radial systolic function that significantly contributes to RV ejection in the setting of severe RV hypertrophy.
Since RV dysfunction and advanced PH with systemic or supra-systemic RV pressure frequently affects diastolic and systolic LV function, tissue Doppler imaging (TDI) not only for the RV but for the left lateral wall and interventricular septum, as well as MAPSE for longitudinal systolic LV function, also should be documented at PH diagnosis and in selected patient encounters at PH follow-up.
Deformation imaging (2D strain and strain rate)
Strain measurements are known to be useful to quantify global and regional RV function in adult patients with PH.19 The more severe the PH, the lower the end-systolic longitudinal strain in the RV free wall, demonstrating a dependence of systolic RV longitudinal strain measurement on RV afterload.20 RV global longitudinal peak systolic strain and strain rate were significantly reduced in adults with PH compared with controls.21 Significant correlations between RV strain and strain rate and the mean PAP were found in adult patients with PH.22 An individual improvement of >5% in RV strain at follow-up was correlated with better pulmonary haemodynamics, improved clinical status and less evidence of RV failure.23 It was recently observed that low RV longitudinal peak systolic strain (>−19%) was associated with lower TAPSE and worse New York Heart Association functional class.24 Quantitative assessment of RV free-wall longitudinal strain is feasible and a powerful predictor of clinical outcome of patients with known or suspected PH.25 Disadvantages of deformation imaging include the relative low temporal solution that hinders tracking in the presence of high heart rates, and the time-intensive postprocessing of the image data.
3D echocardiography
3D echocardiography is very dependent on adequate acoustic windows with 3D measurements and only feasible in about 50% of all patients studied26 due to inadequate image quality. In patients with PH, a good correlation was found in the measurements of RVEF and right ventricular end-diastolic volume (RVEDV) determined by either 3D echocardiography or MRI. Thus, it is suggested that RV remodelling can be comprehensively assessed by 3D echocardiography as long as image quality is adequate.27 By 3D TTE, adult patients with PAH had more dilated, hypertrophied and poorly functioning RVs compared with other forms of PH.28 The use of 3D echocardiography has been validated for the measurement of RV volumes, and EF in adults, which correlated well with variables determined by cardiovascular MRI also in a paediatric population.29
Systolic-to-diastolic duration ratio
In patients with PH, RV contraction is prolonged, although RV ejection time is shortened, so that systolic (S) duration to diastolic (D) S/D duration was proposed as an indicator of PH severity.30 Children with significant PH have a marked decrease in diastolic duration and increase of the S/D duration ratio when their heart rates increase compared with control subjects (figure 2B). An increased S/D duration ratio >1.4 inversely correlates with survival in paediatric PH.31 A limitation of S/D duration ratio is the need for a clearly defined onset and end of TR on spectral Doppler tracings to assess ventricular function. Although RV contraction is prolonged but RV ejection is shortened in severe PH, diastolic duration (or more precisely relaxation and filling) is even shorter than systolic ejection.32 The S/D duration ratio is not dependent on heart size, which is of importance in growing children.
Tissue Doppler velocities
TDI, which measures myocardial velocities, allows quantitative assessment of RV systolic function. Tissue velocities vary with age, therefore normal values for adults cannot be applied to children. In adults, TDI measurements have been shown to have a sensitivity of only 33% and a specificity of 100% to identify patients with precapillary PH, and a negative predictive value of 85% to rule out precapillary PH.33 In paediatric PH associated with congenital heart disease (PH-CHD), the tricuspid annular peak systolic velocity (S′) measured on the lateral tricuspid annulus is significantly impaired, with constant decrease of the S′ value the longer the PH lasts34 (Figure 2C). RV TDI variables were found to correlate well with invasive pulmonary haemodynamics in patients with paediatric PH-CHD and were suggested to be useful variables in the follow-up of children with IPAH.35 TDI investigations of patients with paediatric PH revealed lower S′ and early diastolic (E) velocities at the tricuspid, septal and LV lateral wall compared with controls.36 In patients with paediatric PH, abnormalities in systolic and diastolic ventricular function were also identified and shown to be more prominent with older age.37 Of note, TDI be applied to any chamber morphology because the variables are not based on any assumption of chamber geometry. The limitations of TDI are mainly related to the variability of the measured velocities with different loading conditions, heart size and the dependency on the angle of interrogation.
RV-to-LV diameter ratio
RV is more compliant than LV but LV adapts better to pressure overload. In PH, pressure in RV increases, causing the interventricular septum to flatten in systole. In cases of supra-systemic RV pressure, the septum may even bulge into the LV cavity at end systole.38 The RV/LV end-systolic diameter ratio, measured in the parasternal short-axis view at the level of the papillary muscles at end systole, is a variable that correlates well with invasive haemodynamic measures39 (Figure 3A). The RV/LV ratio was derived to combine a measure of RV size with septal shift secondary to elevated RV pressure. The RV/LV ratio has been shown to be significantly higher in children with PH compared with controls.39 An RV/LV ratio >1 was associated with increased risk for adverse events in paediatric PH.39 The RV/LV end-systolic diameter ratio can be easily obtained in the clinical setting and used to follow patients with PH over time. Limitation of the RV/LV end-systolic diameter ratio is that left-to-right shunts lesions may alter RV size and that therefore this index is of limited use in such patients with PH. In a pressure-loaded RV, flattening of the septum occurs in end systole, resulting also in an increased end-systolic LV eccentricity index. This LV eccentricity index (figure 3A) is the ratio of the minor axis of LV parallel to the septum divided by the minor axis perpendicular to the septum. An LV eccentricity index >1 has been shown to be prognostic in adult patients with IPAH who also had a decreased RV systolic function.40
Pulmonary flow velocity measurements
The PA forward flow velocity profile, obtained in the RVOT with pulsed wave (PW)- Doppler just proximal to the pulmonary valve, can be used to obtain PAAT (figure 3B). PAAT is the interval in microseconds from the onset of ejection to the peak flow velocity and can be used for the estimation of RV pressure and PASP.41 Even when a TR CW-Doppler envelope is not available or incomplete, PAAT measurements are possible in 99% of patients.41 In adults, a PAAT <100 ms is considered abnormal and an indicator for elevated mPAP and PVR.42 In children, a PAAT >124 ms was suggested as cut-off value to distinguish between patients with PH and healthy controls.43 Proper placement of the Doppler sample in the middle of PA and accurate alignment to the long axis of PA is essential. Limitation of PAAT is its dependency on heart rate and RV function, that is, usually, tachycardia shortens and systolic RV dysfunction lengthens the PAAT.
Follow-up
Following the initial diagnostic evaluation for PH, transthoracic echocardiograms should be performed in 3–6 months' intervals. More frequent echocardiograms should be conducted when the clinical condition or medication changes (class of recommendation (COR): I; level of evidence (LOE): C).
Conclusion
The results of the initial TTE examination often are pivotal in the decision-making process whether children should be referred to an expert PH centre and undergo further diagnostic testing, including cardiac catheterisation and cardiac MRI. We suggest the regular assessment of certain prognostic TTE variables as part of a standardised approach for initial diagnosis and for the follow-up management of children with PH. Overreliance on any single TTE variable should be avoided as it detracts from the overall diagnostic potential of a comprehensive standardised TTE examination for PH. Thus, a TTE protocol for PH should include an estimation of the systolic PAP (TR CW-Doppler), the estimation of mean PAP and end-diastolic PAP (PR CW-Doppler), determination of the PAAT (RVOT PW-Doppler) as surrogate of PAP and PVR, RV longitudinal systolic function measurements using M-mode, RV strain and strain rate measurements, RV volume measurement by 3D echocardiography, determination of the RV systolic to diastolic duration ratio (TR), determination of tissue Doppler velocities, measurement of the RV/LV end-systolic diameter ratio, and LV eccentricity index. Regular and consistent usage of such a TTE protocol may increase the identification of children with PH, leading to earlier comprehensive diagnosis and treatment. However, no clinical decision should be based solely on these TTE measures and confounding factors such as a right bundle brunch block make interpretation of TTE variables difficult. Prospective comparative studies in patients with paediatric PH and randomised controlled trials using the suggested TTE variables are therefore necessary. However, the new imaging methodologies discussed in this article already offer new insights into RV function and geometry in PH. Cardiac sonographers should become familiar with both traditional and newer techniques for more detailed assessments of ventricular performance in children with PH.
References
Footnotes
This article is a product of the writing group of the European Paediatric Pulmonary Vascular Disease (PVD) Network (Writing Group Chair: G. Hansmann, Writing Group Co-Chair C. Apitz). ISHLT, International Society of Heart and Lung Transplantation. DGPK, German Society of Paediatric Cardiology.
Competing interests GH and CA indicate no conflict of interests related to the content of this article. HA-K served as consultant for Actelion and received financial reimbursement for his service.
Relationships with industry (RWI): HAK served as consultant for Actelion and received financial reimbursement for his service. MK, CA and GH no relevant relationship with industry.
Funding CA currently receives grant funding from Stiftung Kinderherz (2511-10-13-001) and Behring-Röntgen-Stiftung (59-0018). GH currently receives grant support from the German Research Foundation (DFG; HA 4348/2-1), Fördergemeinschaft deutsche Kinderherzzentren (W-H-001-2014) and Stiftung Kinderherz (2511-6-13-011).
This Heart supplement was produced with support from an unrestricted educational grant from Actelion Pharmaceuticals Germany GmbH, Bayer Pharma AG, and Pfizer Inc. None of these organisations had any influence on the composition of the writing group or the content of the articles published in this supplement. Open Access publication of this article was sponsored by Actelion Pharmaceuticals Germany GmbH.
Provenance and peer review Commissioned; externally peer reviewed.