Article Text

Abstract
Childhood pulmonary hypertension (PH) is a heterogenous disease associated with considerable morbidity and mortality. Invasive assessment of haemodynamics is crucial for accurate diagnosis and guidance of medical therapy. However, adequate imaging is increasingly important in children with PH to evaluate the right heart and the pulmonary vasculature. Cardiac MR (CMR) and computed tomography (CT) represent important non-invasive imaging modalities that may enable comprehensive assessment of right ventricular (RV) function and pulmonary haemodynamics. Here, we present graded consensus recommendations for the evaluation of children with PH by CMR and CT. The article provides a structured approach for the use of CMR and CT imaging, emphasises non-invasive variables of RV function, myocardial tissue and afterload parameters that may be useful for initial diagnosis and monitoring. Furthermore, assessment of pulmonary perfusion and characterisation of the lung parenchyma provides structural information about processes that may cause or be due to PH.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Video abstract
Introduction
Pulmonary hypertension (PH) as a result of elevated pulmonary vascular resistance (PVR) ultimately leads to right ventricular (RV) failure and premature death when not responsive to therapy. Despite progress in medical treatment, morbidity and mortality is still high, especially in idiopathic pulmonary arterial hypertension (IPAH). RV failure represents the most common cause of death in childhood PH, and therefore, reliable evaluation of RV function is crucial.1
Echocardiography is the most commonly used non-invasive tool for initial assessment, screening and serial follow-up as it allows rapid assessment of RV function and estimation of pulmonary artery pressure. However, this technique can be limited by poor acoustic windows and the complex geometry of the RV. This sometimes makes reliable assessment of RV function using echocardiography difficult.2
A more comprehensive assessment of the RV and the pulmonary vasculature is possible by cardiac MR (CMR) and CT. These techniques have become important non-invasive imaging modalities in the management of adult PH. CMR offers the ability to assess ventricular function, blood flow, pulmonary perfusion and myocardial tissue characteristics. The main role of CT is to detect alternative causes of PH including lung parenchymal disorders, thromboembolic disease and vascular abnormalities such as pulmonary vein stenosis.
In this consensus statement, we review the principles and application of CMR and CT in patients with paediatric PH. The article provides practical recommendations and emphasises non-invasive variables that may be useful for initial diagnosis and monitoring.
Methods
The recommendations summarised in table 1 relate to the grading system currently suggested by the European Society of Cardiology and the American Heart Association, and was based on paediatric data only (class, level of evidence). The grading and voting process within the writing group is outlined in the executive summary of this special issue. Computerised searches of the PubMed/MEDLINE bibliographic database were conducted between January 1990 and June 2015. Clinical trials, guidelines and reviews limited to paediatric data were searched using the terms ‘pulmonary hypertension’, ‘children’, ‘cardiac magnetic resonance’ and ‘computed tomography’.
Recommendations on the use of cardiac magnetic resonance and computed tomography in children with pulmonary hypertension
CMR protocol
CMR in young children is often performed under either sedation or general anaesthesia. However, patients with paediatric PH are at high risk for cardiac decompensation, and therefore, anaesthesia and sedation come at substantial risk.3 If anaesthesia or sedation is required, it is important to thoroughly weigh the benefits gained from the information acquired against the risks of anaesthesia in a child with PH. If no sedation is required, e.g in an older child, cardiac CMR is recommended in children with suspected or confirmed PH/paediatric pulmonary hypertensive vascular disease (PPHVD) as part of the diagnostic evaluation and during follow-up. As with all CMR examinations, it is recommended that protocols are optimised to answer specific questions related to the disease. Below is a list of the main advantages and disadvantages of CMR variables (table 2), a recommended protocol for paediatric PH (table 3).
Advantages and disadvantages of CMR measurements in pulmonary hypertension
Proposed CMR protocol in children and adolescents with suspected or confirmed PH/PPHVD
Ventricular assessment
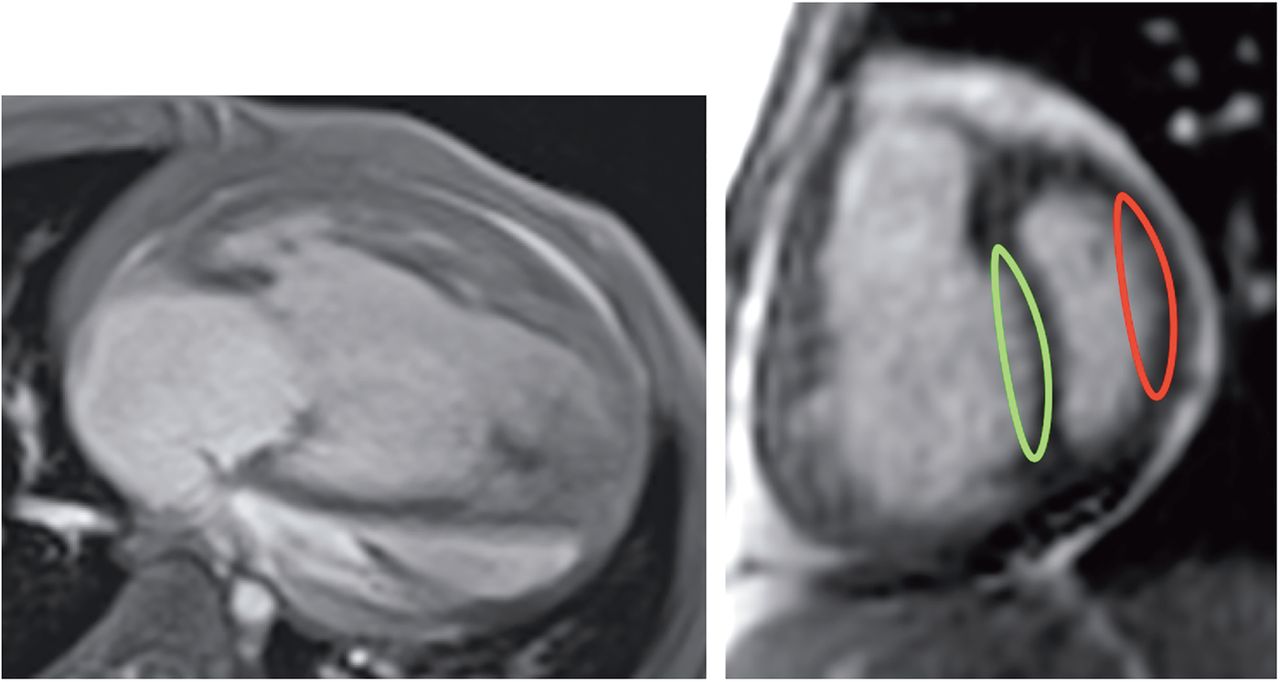
Cine CMR is the gold standard for the assessment of biventricular volumes, muscle mass and global pump function.4 ,5 Cine CMR is also highly reproducible, making it ideally suited for serial follow-up examinations to detect changes in RV dimensions and function.6 ,7 Thus, Cine CMR it is the most important component of a paediatric PH CMR. A stack of contiguous short-axis or transverse slices covering both ventricles is used to measure ventricular volumes (figure 1). There are some data to suggest that transverse slices provide more accurate assessment of RV volumes.8 ,9 However, this has not been definitively demonstrated in paediatric PH. It is recommended that a steady-state free precession (SSFP) sequence is used with approximately 20 true phases per cardiac cycle and a slice thickness of between 5 and 8 mm depending on patient size. This is typically achieved by either short breath-holds or in uncooperative patients free-breathing measurements. Free-breathing cine CMR can be achieved by using signal averaging or real-time techniques. The clinical importance of cine CMR in the paediatric PH population has recently been demonstrated in the study by Moledina et al,7 which included 100 children and adolescents with PH of various aetiologies. This study revealed several CMR parameters to correlate with functional class, 6-minute walk distance and invasive haemodynamic measurements such as pulmonary artery pressure. Furthermore, this study revealed the prognostic value of CMR in the children and young adolescents with PH: of all CMR indices, RV ejection fraction and left ventricle (LV) indexed stroke volume were most associated with an increased risk of death or transplantation with a 1 SD decrease in there measures, resulting in a 2.6-fold and 2.5-fold increased risk of death, respectively. In another study, Blalock et al6 assessed RV volumes and function by cine CMR in a smaller cohort of 26 patients with PH aged 2–16 years and found RV parameters abnormal in contrast to healthy individuals. In a follow-up examination in 15 patients, RV volumes, function and LV stroke volume showed no significant change over 1 year, which was probably related to a relatively stable cohort with normal 6-minute walk distances.
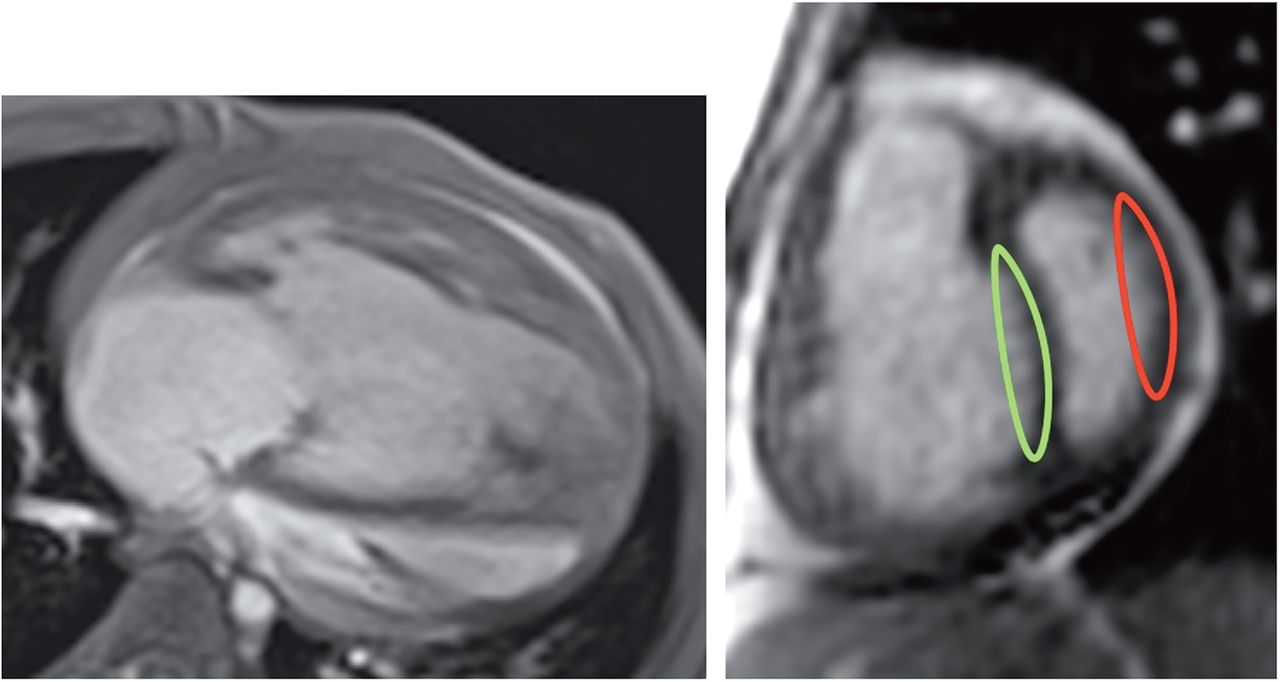
Cine images in the four-chamber view (left) of a patient with systemic PA pressures showing right ventricular (RV) dilatation and hypertrophy and an enlarged right atrium. The short-axis view (right) of a patient with severe idiopathic pulmonary hypertension showing a severely dilated and hypertrophied RV with end-systolic septal bowing to the left. The green and red lines represent the curvature of the interventricular septum and the left ventricle free wall.
Blood flow
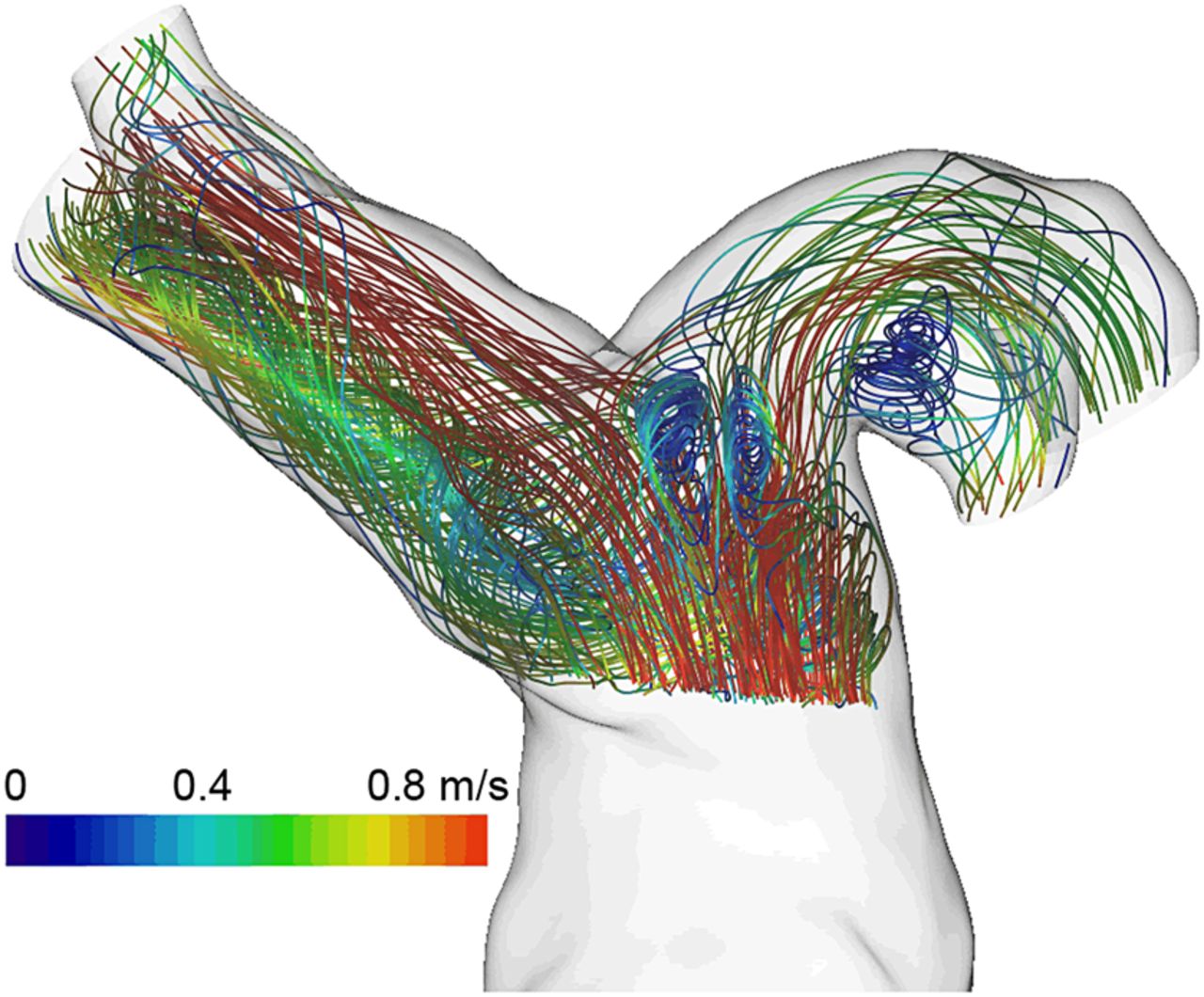
Measurement of blood flow in the ascending aorta, the pulmonary trunk and the right and left pulmonary artery using standard two-dimensional velocity encoded phase contrast MR (PCMR) should always be part of the CMR study (table 4). PCMR allows accurate quantification of cardiac output and shunts, as well as differential lung perfusion and evaluation of valve function.10–12 The CMR study may also include the assessment of blood flow in the systemic or pulmonary veins to allow quantification of blood flow through aortopulmonary or venovenous collaterals. Measurement of blood flow by PCMR is performed in a single plane perpendicular to the vessel of interest. PCMR has low interstudy and interobserver/intraobserver variability and is best performed using free-breathing techniques. Breath-hold or real-time PCMR is possible but tends to have lower spatiotemporal resolution.13 Quantification of blood flow by MR is affected by complex flow patterns as seen in the dilated pulmonary vasculature (figure 2). This is particularly true in the main pulmonary artery, which is why assessment of flow in the branch pulmonary arteries is recommended.14 Assessment of peak velocities is not accurate with PCMR, and reliable quantification of pressure gradients is better with echocardiography.
Summary of CMR and CT studies in children and adolescents with pulmonary hypertension and studies providing CMR reference values in a healthy population

MR image of the pulmonary artery in a patient with pulmonary hypertension. Note abnormal recirculating blood flow patterns at the level of the dilated left and right pulmonary artery.
Anatomical assessment
Anatomical assessment in children with PH may also be important, particularly if there is a suspicion of congenital heart disease. Contrast-enhanced CMR angiography may be useful in children with PH for the assessment of vascular abnormalities. Although uncommon in childhood PH,15 MR angiography may also detect vascular obstruction caused by pulmonary thromboembolism (figure 3) or peripheral pulmonary artery stenoses.16–18 Conventional contrast-enhanced MR angiography is acquired in a breath-hold. Unfortunately, due to the high prevalence of dyspnoea in these patients, the long breath-holds required may be difficult to perform. New techniques such as time-resolved MR angiography may solve problems associated with breath-holding as well as provide quantitative information about perfusion heterogeneity.19 Due to current limitations, MR angiography is not recommended as a sole screening test for chronic thromboembolic PH and most international guideline groups continue to recommend ventilation perfusion scintigraphy followed by pulmonary angiography or CT pulmonary angiography instead. MR angiography is also useful in detection of congenital vascular causes of PH, such as patent ductus arteriosus. However, for assessment of intracardiac causes of PH, such as a ventricular septal defect (VSD), when unable to characterise by echocardiography, three-dimensional SSFP whole heart imaging is recommended.20 Since it is respiratory navigated and ECG triggered, there is no necessity for breath-holding and it is well suited to this patient population.
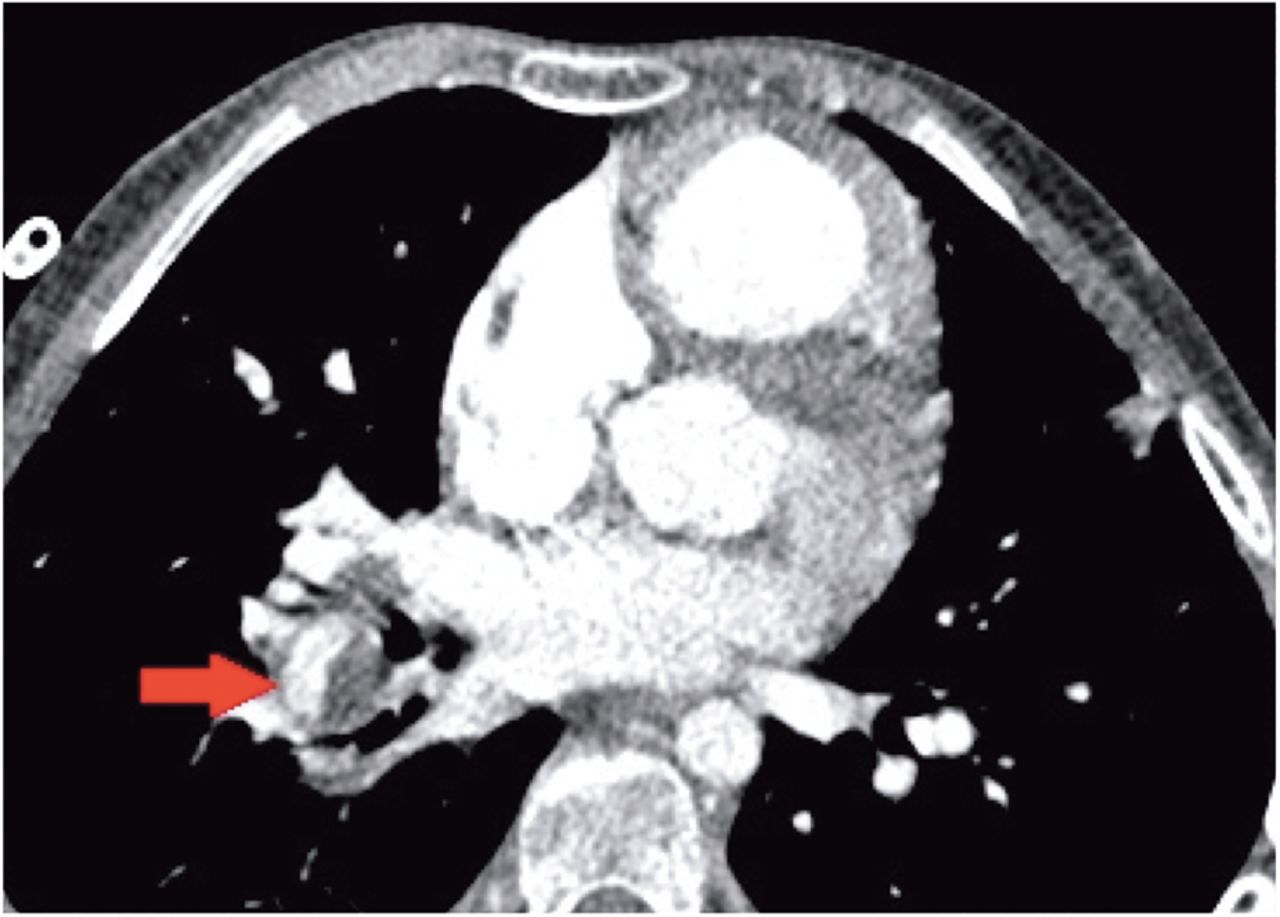
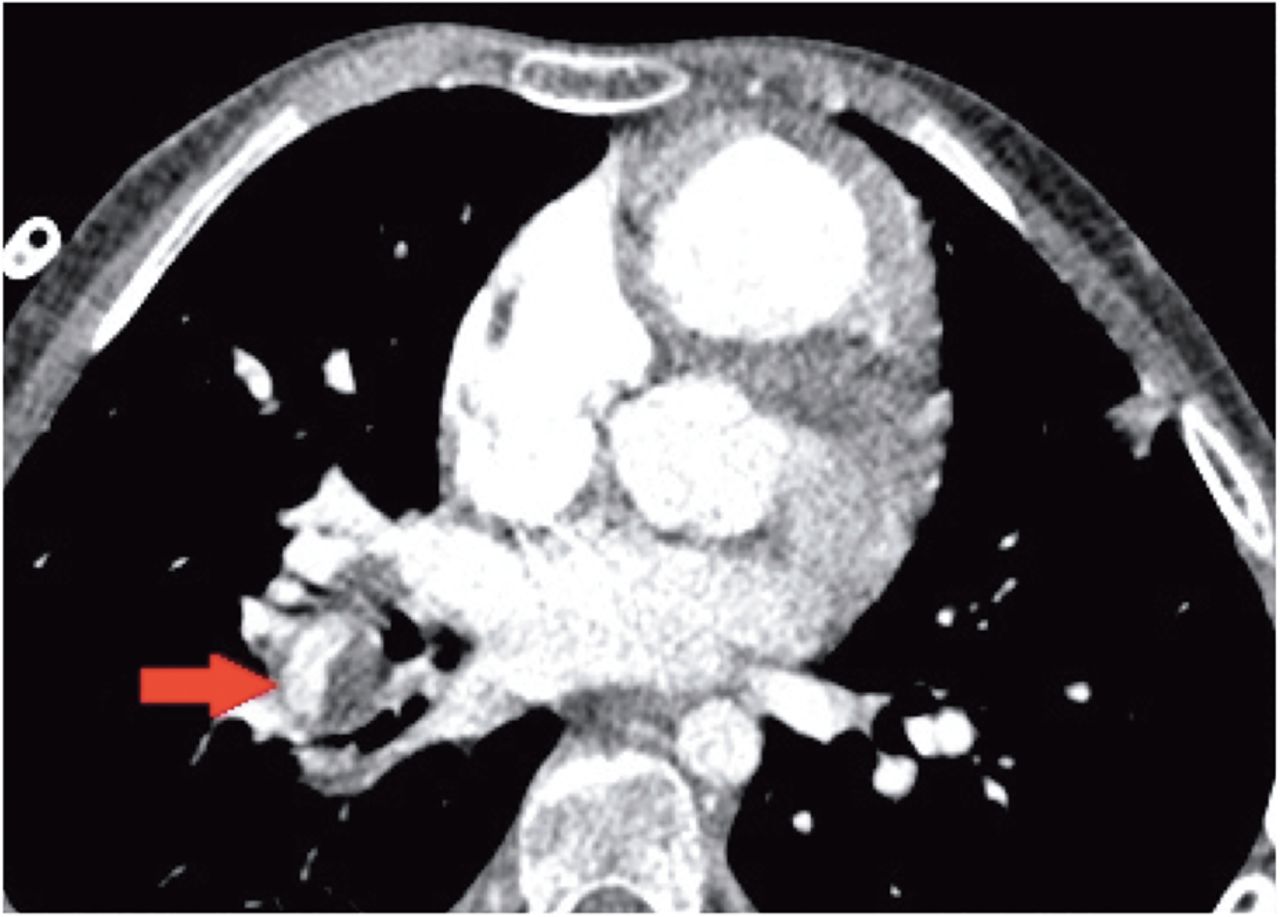
CT image for a patient with chronic thromboembolic pulmonary hypertension. The arrow points to the right lower lobe pulmonary artery, which is partially occluded by thrombus.
Myocardial tissue characterisation
Increased RV afterload is associated with myocyte apoptosis, inflammation and fibrosis.21 Thus, quantification of myocardial fibrosis may be a useful indicator of disease severity. Late gadolinium enhancement (LGE) is typically seen at the RV insertion points (figure 4) and has been found to be related to abnormal pulmonary haemodynamics and RV systolic dysfunction.22–28 Data about the presence of LGE and quantitative data on diffuse RV myocardial fibrosis by mapping techniques and/or extracellular volume quantification are lacking in childhood PH. The prevalence, haemodynamic consequences and prognostic value of delayed enhancement in childhood PH need to be defined in the future.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Late gadolinium enhancement image in the short-axis view in a 7-year-old patient with suprasystemic idiopathic pulmonary arterial hypertension. Note the areas of regional fibrosis typically found at the right ventricular insertion points (arrows).
Areas of further development
Combined measurement of invasive pressure and MR-based volume and flow data by CMR augmented cardiac catheterisation has been described by several groups.29–32 So far, it is uncertain whether simultaneous pressure measurements should be included in a CMR study of a child with suspected PH/PPHVD as experience is currently limited to a small number of specialised centres. CMR-augmented catheterisation may offer some advantages including a precise calculation of PVR due to a more reliable quantification of pulmonary flow volume compared with thermodilution technique or oximetry.31 ,32
Uncertainty exists regarding non-invasive estimation of RV afterload parameters such as RV pressure, PAP and PVR by CMR imaging in children with PH as these techniques are primarily validated in adults.33 ,34 Analysis of interventricular septal curvature by CMR (figure 1) has been found to correlate with mean PAP and indexed pulmonary vascular resistance (PVRi) in adults and in children.35 ,36 Septal curvature metrics also reliably tracked changes in haemodynamics during acute vasodilator testing, making it potentially useful for afterload assessment during follow-up.36 Cine CMR assessment of pulmonary distensibility may be used to detect PH and has been shown to correlate with outcome in small studies.
CT in paediatric PH
The principal role of CT in assessment of PH is to demonstrate features of secondary forms of PH. More specifically, this modality is suited to assessing for parenchymal lung disease, vascular abnormalities and thromboembolic disease. It may also provide information on cardiac, mediastinal abnormalities and may suggest a diagnosis of PH. As such, it features as an early investigation for patients suspected of PH in various guidelines.37 Multislice CT has made it possible to image the thorax at high resolution in under 5 s producing isotropic data at sub-millimetre resolution.
Computed tomography pulmonary angiography (CTPA) protocols vary depending upon the type of scanner, the availability of ECG-gating among other factors. Nevertheless, the aim of any CTPA study is to optimally opacify the right heart chambers and pulmonary arterial tree and limit cardiac and diaphragmatic motion artefact.
CT, when performed for the investigation of other conditions, may raise the suspicion of PH. A recent systematic review and meta-analysis in adult CT suggests the pulmonary artery dilatation and pulmonary artery to ascending aorta diameter ratio to have high specificity for PH. Similar data are not yet available in children.38
CT is the modality of choice for the detection of parenchymal lung disease such as chronic lung disease and developmental abnormalities. Identification and quantification of lung disease may be particularly helpful in paediatric PH, where history of dyspnoea may be non-specific and when younger children may not reliably perform pulmonary function testing. In addition, prevalence of congenital lung abnormalities is likely to be higher in children than in adults. In addition, CT is highly sensitive for the identification of pulmonary veno-occlusive disease (PVOD) due to its characteristic features: thickened interlobular septa, poorly defined nodular opacities and lymphadenopathy.39 POVD is an important differential diagnosis because of its impact it has on management strategy.
Chronic thromboembolic disease (CTED) is an important diagnosis to exclude in patients with PH. Even though the incidence is likely to be low in children with PH, the possibility to surgically cure this condition warrants assessment. Due to its rarity, paediatric-specific data from on are lacking; however, by extrapolation from extensive research in adult CTED, CT pulmonary angiography is the first-line cross-sectional imaging modality for the evaluation of chronic thromboembolic PH in patients with suggestive ventilation-perfusion scan.40 Recent data suggest that modern CT technology in experienced hands may have nearly equal sensitivity and specificity to V/Q scanning. Importantly, CT angiography can distinguish between surgically amenable disease from distal disease.37
CT pulmonary angiography is well suited to assessment of great vessel anatomy and to the detection of extracardiac shunt lesions, for example, persistent arterial duct, aortopulmonary collaterals; however, operators should be aware of the possibility of false negative results. While echocardiography remains the first-line imaging modality for assessing congenital cardiac and vascular abnormalities, CTPA remains an extremely useful adjunct.
Protocols should be developed to minimise exposure to ionising radiation and follow-up CTs should be kept to a minimum. Where possible it is recommended that children undergo low-dose prospectively ECG-gated CT as it provides better image quality.
References
Footnotes
This article is a product of the writing group of the European Paediatric Pulmonary Vascular Disease (PVD) Network (Writing Group Chair: G. Hansmann, Writing Group Co-Chair: C. Apitz). DGPK, German Society of Paediatric Cardiology; ISHLT, International Society of Heart and Lung Transplantation
Funding HL currently receives grant funding from the Pitzer Stiftung (Bad Nauheim, 12-147), the German Society of Paediatric Cardiology (DGPK) and the Fördergemeinschaft Deutsche Kinderherzzentren (W-GI-017/2013). TK currently receives grants from the German Federal Ministry for Education and Science (BMBF SysMed2-012/Az 0101-31P8971), from the European Commission (EUFP7 and EU FP7) and the German Research Foundation (DFG KU1329/10). PB receives grant funding from the Medical Research Council (UK) (MRSBACR), the Fördergemeinschaft Deutsche Kinderherzzentren (W-H-003/2014) and the Kompetenznetz angeborene Herzfehler (FKZ 01GI0210). CA currently receives grant funding from Stiftung Kinderherz (2511-10-13-001) and Behring-Röntgen-Stiftung (59-0018). GH currently receives grant support from the German Research Foundation (DFG; HA 4348/2-1), Fördergemeinschaft deutsche Kinderherzzentren (W-H-001-2014), Stiftung Kinderherz (2511-6-13-011). VM receives grant support from the British Heart Foundation and Great Ormond Street Hospital Charity.
This Heart supplement was produced with support from an unrestricted educational grant from Actelion Pharmaceuticals Germany GmbH, Bayer Pharma AG, and Pfizer Inc. None of these organisations had any influence on the composition of the writing group or the content of the articles published in this supplement. Open Access publication of this article was sponsored by Actelion Pharmaceuticals Germany GmbH.
Competing interests SM has acted as a consultant for Bayer pharmaceuticals.
Provenance and peer review Commissioned; externally peer reviewed.