Article Text

Abstract
Persistent pulmonary hypertension of the newborn (PPHN) is the most common neonatal form and mostly reversible after a few days with improvement of the underlying pulmonary condition. When pulmonary hypertension (PH) persists despite adequate treatment, the severity of parenchymal lung disease should be assessed by chest CT. Pulmonary vein stenosis may need to be ruled out by cardiac catheterisation and lung biopsy, and genetic workup is necessary when alveolar capillary dysplasia is suspected. In PPHN, optimisation of the cardiopulmonary situation including surfactant therapy should aim for preductal SpO2 between 91% and 95% and severe cases without post-tricuspid-unrestrictive shunt may receive prostaglandin E1 to maintain ductal patency in right heart failure. Inhaled nitric oxide is indicated in mechanically ventilated infants to reduce the need for extracorporal membrane oxygenation (ECMO), and sildenafil can be considered when this therapy is not available. ECMO may be indicated according to the ELSO guidelines. In older preterm infant, where PH is mainly associated with bronchopulmonary dysplasia (BPD) or in term infants with developmental lung anomalies such as congenital diaphragmatic hernia or cardiac anomalies, left ventricular diastolic dysfunction/left atrial hypertension or pulmonary vein stenosis, can add to the complexity of the disease. Here, oral or intravenous sildenafil should be considered for PH treatment in BPD, the latter for critically ill patients. Furthermore, prostanoids, mineralcorticoid receptor antagonists, and diuretics can be beneficial. Infants with proven or suspected PH should receive close follow-up, including preductal/postductal SpO2 measurements, echocardiography and laboratory work-up including NT-proBNP, guided by clinical improvement or lack thereof.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Video abstract
Introduction
Pulmonary hypertension (PH), especially in the neonate, is a syndrome with multiple possible aetiologies, leading to challenges in its management. In the newborn, persistent pulmonary hypertension of the newborn (PPHN; PH group 1”) is mostly associated with pulmonary or systemic conditions leading to acute respiratory failure. In the preterm infant, PH mainly occurs with chronic lung disease (CLD) where impaired vascular growth and function results from prenatal and postnatal injuries. Likewise, other developmental lung anomalies such as congenital diaphragmatic hernia (CDH) can be associated with PH. Both, the heterogeneity of the disease mechanisms and the lack of evidence from clinical trials limit the availability of standardised treatment regimen. Long-term outcome in infants with PH is largely unknown. Here, we discuss different pathophysiological aspects of PH in the preterm and term neonate with acute or chronic lung disease, and presents expert consensus recommendations on diagnostic and therapeutic approaches.
Classification
As a modification of the Dana Point classification,1 the Nice World Symposium classification of PH2 now emphasises different conditions of the lungs arising in the neonatal period associated with the development of PH. First, PPHN due to its particular anatomic and physiological nature forms a separate subcategory in group 1 ‘pulmonary arterial hypertension’. Second, group 3 ‘pulmonary hypertension due to lung diseases and/or hypoxia’ now comprises a subcategory ‘developmental lung diseases’. In this category, different disease entities are summarised resulting from abnormalities of the alveolar and vascular compartment or the connective tissue as a consequence of early pre or postnatal injury mechanisms impacting on lung developmental processes (table 1).
Recommendations for supportive measures and pharmacotherapy in PPHN and PH associated with BPD/nCLD
Methods
The recommendations of this expert consensus statement are given in table 1. The recommendations relate to the grading system currently suggested by the European Society of Cardiology (ESC) and the American Heart Association (AHA), and were based on data derived from paediatric studies only (class, level of evidence). The grading and voting process within the writing group is outlined in the executive summary of this online supplement.24 Computerised searches of the PubMed/MEDLINE bibliographic database from January 1990 to July 2015 were conducted. The developer searched using the terms ‘pediatric pulmonary hypertension’, ‘pulmonary hypertension’, ‘neonate’, ‘neonatal chronic lung disease’, ‘bronchopulmonary dysplasia’, ‘congenital diaphragmatic hernia’, ‘nitric oxide’, ‘sildenafil’.
Background on PH in the NEONATE and infant
We focused on expert consensus statements referring to the most common and most relevant clinical scenarios associated with PH in the neonate and infant: PPHN (here defined as PH with failed postnatal decrease in pulmonary vascular resistance (PVR)), PH associated with CDH/lung hypoplasia, and PH in bronchopulmonary dysplasia (BPD)/neonatal CLD (nCLD).
The consequence of the first breaths after birth aiming at establishing functional residual capacity of the lungs is an acute drop of PVR that allows a subsequent 8-fold to 10-fold increase in pulmonary blood flow, essential for postnatal gas-exchange through the lungs. If this physiological adaptation fails, PPHN can develop.
PPHN as a disease of failed postnatal transition with persistently high PVR and pulmonary arterial pressure (PAP) has been estimated to occur in 2 per 1000 of live born infants.25 Others have defined PPHN as a disease occurring during the first 30 days of life usually presenting at or within a few days after birth.26 Regardless of the definition, the diagnostic evaluation of any neonate presenting with symptomatic PH outside the first week of life is critical as the aetiology is likely to exceed the classical PPHN diagnosis. Chronic progressive PH in the first year of life is now known to be a distinct condition that is even less well understood than PPHN, and may occur or worsen with or without a preceding PPHN episode. This disease can resemble idiopathic PAH of infancy, which tends to have a poor prognosis.27
PH frequently complicates the course of neonates with respiratory failure. Known risk factors for the development of PPHN are (elective) caesarean delivery, meconium aspiration syndrome, severe respiratory distress due to primary surfactant deficiency in the preterm infant and sepsis.28 It can occur without any perinatal risk factor, but is known to complicate the course of congenital heart diseases. The role of maternal drug intake such as serotonin reuptake inhibitors in promoting PPHN remains a matter of debate. Prenatal constriction of the arterial duct (ductus arteriosus)—sometimes due to exposure to non-steroidal anti-inflammatory drugs in the third trimester—may also cause neonatal PH resembling PPHN but with a restrictive or closed arterial duct.29
PPHN can be a life-threatening complication but is in most cases reversible within the first few days of life, usually alongside the improvement of the pulmonary disease it accompanies. When PPHN does not resolve within 2 weeks of adequate management and chest CT indicates significant parenchymal lung disease, alveolar capillary dysplasia (ACD) should be evoked by lung biopsy (or at autopsy). In ACD, histological findings include reduction in alveolar capillaries, thickening of alveolar septal tissue, and lack of sufficient endothelial-epithelial contact. A few familial cases suggest a possible genetic cause. In addition, deletions and point mutations within the FOX transcription factor gene cluster at 16p24.1 were identified.30 Currently, ACD is incurable, with a maximum reported survival of 3 months,31 ,32 although ACD occurred up to the age of 6 months in our own patient population (unpublished).
In congenital diaphragmatic hernia (CDH), PH is present in most cases, although its pathophysiology is not univocal. Indeed, lung hypoplasia and the reduction of pulmonary arterial cross-sectional area, abnormal vasoreactivity to hypoxic episodes and left heart diastolic dysfunction result in changes of the pulmonary vascular pressure and blood flow.33 ,34 The difference between various contributors to PH development in CDH often complicates the decision on the best preoperative and surgical management in the most severe forms of CDH. Likewise, postoperative PH in CDH requires careful evaluation of all known variables impacting on PVR as well as pulmonary and systemic blood flow in these infants.
Table 2 gives an overview over the most important lung developmental anomalies that are known to are known to be associated with PH.
Developmental lung diseases associated with pulmonary hypertension
PH associated with BPD/nCLD mainly develops in the preterm infant. BPD is defined according to Jobe and Bancalari as oxygen requirement at day 28 of postnatal life or oxygen or ventilator support at 36 weeks postmenstrual age.35 Risk factors such as very low birth weight with and without the presence of intrauterine growth restriction, placental anomalies, intra-amniotic infections, and postnatal risk factors such as oxygen toxicity, mechanical ventilation and congenital and nosocomial infections among others contribute to the development of BPD/nCLD. These conditions develop their impact in a critical developmental window, where the functionally and structurally immature organ is vulnerable towards the induction of dramatic and sustained changes determining postnatal respiratory outcome. The pathobiology and clinical course of BPD/nCLD has changed in the postsurfactant era: The disease is now characterised by (1) impaired alveolarisation with fewer, larger and simplified alveoli, alongside with (2) disturbed vasculogenesis resulting in fewer (small, intra-acinar) pulmonary arteries. Bronchial smooth muscle thickening, interstitial oedema, fibrosis and inflammation known from the presurfactant era can also be found in the new form of the disease. Associated with defective vascular function and structure the reduction in vascular surface area can result in pulmonary hypertensive vascular disease that impacts short and long-term survival and is characterised by pulmonary arteriolar muscularisation, vessel loss, and right ventricular (RV) hypertrophy, among other findings.
In concert with the different pre and postnatal risk factors indicated above, the presence of alveolar hyperoxia (and hypoxia resulting from frequent desaturations) as well as mechanical stretch lead to the structural remodelling of the pulmonary vasculature. Beyond the neonatal period, increased pulmonary vascular tone and heightened vasoreactivity may contribute to sustained PH and potentially increase the risk for late PH associated with (n)CLD.
Although PH predominantly develops in the very low birth weight and very preterm infant, some infants develop late onset PH after a couple of weeks.22 ,36 ,37 Furthermore, the moderate but growth-retarded preterm infant has been shown to develop PH in a considerable number of cases.36 A crucial and unresolved question in neonates and infants with BPD is the optimal time for PH screening by echocardiography. At the same time, the best diagnostic tool to detect PH in patients with BPD is still a matter of debate, as the non-invasive evaluation by echocardiography has been shown to lack sensitivity compared with the invasive procedure of cardiac catheterisation in these patients. Finally, the prediction of late PH by the presence of early disease in the preterm infant is still questionable. Certainly, patients with BPD with late PH need careful evaluation and a minimisation of hypoxic episodes.38 Furthermore, the persistence of PH in these and other patients should lead to the consideration of cardiac catheterisation and specific imaging techniques, that is, CT and/or cardiac MRI to rule out pulmonary vein stenosis. It has to be considered that pulmonary capillary haemangiomatosis (PH group 1') may be diagnosed at a wide age range, and may clinically be indistinguishable from pulmonary veno-occlusive disease (PH group 1') or PAH (PH group 1).
Prognosis and outcome of PH in BPD/nCLD
Approximately one in four infants with moderate-to-severe BPD is known to develop PH,39 triggered by the complex interplay of inflammatory processes, stretch and oxygen toxicity side-by-side with recurrent alveolar hypoxia leading to endothelial dysfunction. The development of PH in BPD is not only an epiphenomenon or minor secondary event, but appears to greatly increase mortality with an estimated death rate of 47% 2 years after PH diagnosis.40 Furthermore, with an increasing percentage of extremely immature infants surviving in the postsurfactant era, BPD is one of the most common primary diagnoses in neonatal follow-up care and frequently seen in paediatric PH clinics today. BPD as a major etiologic factor for PH development has been recognised and, in fact, was assigned its own category in the recently published classification of paediatric pulmonary hypertensive vascular disease (category 4: BPD; PVRI Panama classification, 2011).26
Diagnosis and monitoring of PH associated with acute or chronic lung disease in the preterm and term neonate and infant
Diagnosis and monitoring of existing or developing PH is critical in PPHN as well as in PH associated with developmental/parenchymal lung diseases. High resolution chest CT with angiography is a key non-invasive diagnostic tool for assessing the underlying lung disease beyond chest X-ray41 and needs to be considered in cases where other diagnostic tools do not suffice. Regarding the diagnosis of PH by echocardiography and catheterisation we refer to other publications in this special issue.42 ,43
In general, transthoracic echocardiography should be performed initially and once or twice per month in all infants with clinical suspicion of PH. The latter is fulfilled with increased oxygen requirement or hypoxaemia, gradual increase in ventilator settings or oxygen requirement and clinical signs of RV dysfunction. In infants treated for acute PH or undergoing weaning from PH, echocardiography should be pursued twice a week in combination with serum BNP/NT-proBNP. In infants with BPD after discharge, regular or continous measurements of oxygen saturation should accompany oxygen weaning in infants with BPD, at the upper and lower extremities. Echocardiography should be performed (a) every 3 months in infants with BPD in need of additional oxygen supply or those at strong risk for PH; (b) every 3–6 months in children at risk, that is, infants with growth retardation, very low birth weight, MV/CPAP >28th day of life, BPD, failure to thrive despite adequate caloric intake. Cardiac MRI can be considered, if available and if strong clinical suspicion for PH with ventricular dysfunction is present. Serum BNP or NT-proBNP are frequently used as monitoring and outcome biomarkers for children with diagnosed PH, but increased concentrations due to high systemic blood pressure, persistent ductus arteriosus (PDA), renal failure, or left ventricular dysfunction can be a confounder. All infants with persistent PH despite optimal management of lung disease, before starting chronic pulmonary vasodilator therapy, should probably undergo cardiac catherisation,3 ,22 ,23 ,40 unless clinical circumstances skew the risk-benefit ratio.
Therapy of PH associated with acute or chronic lung disease in the preterm and term neonate and infant
General treatment measures for PPHN in the term and preterm neonate
Usually, the course of PPHN is favourable. First, exposure to environmental factors that worsen PPHN including handling, tracheal suction, heel pricks and others have to be minimised or avoided, if possible. Furthermore, polycythaemia increasing blood viscosity and increased PVR should be corrected (figure 1).
Mechanical ventilation strategies need to aim for adequate lung recruitment and alveolar ventilation by avoiding overinflation of the lungs as well as high mean airway pressures to prevent both, pulmonary barotrauma and volutrauma. The goal is to maintain preductal SaO2 over 85%, and PaCO2 in the range of 40–55 mm Hg. Optimisation of the acid-base balance (pH range 7.45–7.55) to control PVR may require repetitive doses of sodium bicarbonate, although this therapy needs to be considered with caution due to its known side effects and limitations. Furthermore, appropriate fluid management, cardiovascular resuscitation and use of pulmonary vasodilators should be considered (5). Supporting cardiovascular function remains a major goal in PPHN management. Early initiation of inotropic and vasoactive agents to increase cardiac output, maintain adequate blood pressure and enhance oxygen delivery to the tissue is preferred.
The application of the locally vasodilative inhaled nitric oxide (iNO) is the mainstay of PPHN therapy in most cases. Intravenous vasodilators such as epoprostenol and treprostinil may be considered and should be given through a central venous line of the upper body, but can worsen the clinical condition by creating V/Q mismatch and intrapulmonary shunt resulting in profound desaturations. In all cases, a rigorous clinical and echocardiographic assessment is required for diagnosis and monitoring of biventricular systolic and diastolic function.
Pharmacological and extracorporal membrane oxygenation treatment for PPHN
Infants with significant right-to-left shunting require pulmonary vasodilator therapy. iNO is presently recommended for infants with PPHN12 as it improves outcome in the hypoxemic term and near term infant by reducing the incidence of the combined endpoint death or need for extracorporal membrane oxygenation (ECMO). Oxygenation improves in approximately 50% of infants receiving iNO.12 Usual concentrations of iNO range from 5 to 20 ppm to treat PPHN, with the typical starting dose being 20 ppm. As a preventive measure for the development of acute or chronic PH in the preterm infant with respiratory failure, the use of iNO cannot be recommended outside randomised controlled trials.9 ,10 In patients with CDH, iNO may be considered for bridging to ECMO (oxygenation index>20 or saturation differences >10%; oxygenation index (OI): FiO2%×MAP/pO2) although no beneficial effects could be shown for this patient cohort.44
ECMO may be required to ensure effective oxygenation and decarboxylation while limiting barotrauma and volutrauma of the lung and to improve right heart failure. ECMO is indicated when hypoxaemia persists in spite of optimal medical management according to the following criteria:
Preductal SpO2 <85% despite peak inspiratory pressure >28 cmH2O (or mean airway pressure >15 cmH2O with high frequency oscillation),
PPHN and circulatory failure resistant to adequate management,
Gestational age >34 weeks,
Birth weight >2 kg.
Additional ECMO criteria have been proposed with consistent OI ≥40, systemic hypotension resistant to fluid and inotropic therapy, urine output <0.05 mL/kg/h for 12–24 h and metabolic acidosis (lactate ≥5 mmol/L, pH <7.15). See also the ELSO guidelines for ECMO.45
There is limited experience for the application of systemic medication used in PAH in patients with PPHN. Phosphodiesterase-5 (PDE-5) inhibitors such as sildenafil may be potentially useful as an increase in PDE-5 activity contributes to the pathophysiology of PPHN. Evidence exists that sildenafil is well tolerated in the newborn with PPHN.14 It is applied via feeding tube in a starting dose of 0.5–1 mg/kg/dose every 6 h.46–48 ,64 Meta-analysis of three trials including 77 newborns with PPHN indicated that sildenafil may improve oxygenation and reduce mortality.14 These results suggest that sildenafil has significant potential for PPHN treatment, especially in settings where iNO is not available. Nonetheless, systemic pulmonary vasodilator treatment has to be considered with caution as worsening of the ventilation-perfusion mismatch hypoxia and systemic hypotension may occur, especially in the preterm infant.3 ,49 In CDH, intravenous sildenafil can be considered in case of suprasystemic PAP and right-to-left shunting.
Prostacyclin and analogues have been used in PPHN but evidence is limited as only a few case reports or short series are available. The use of epoprostenol in term and preterm infants requires a central line and careful management of systemic effects.50
Finally, there is increasing evidence that endothelins contribute to PH in the neonate. Although, recent case reports and earlier studies suggest that bosentan may improve PPHN, there is still insufficient evidence to generally recommend the use of bosentan to manage PPHN.51 ,52 The yet unpublished FUTURE4 trial on bosentan in PPHN showed negative results, may be due to poor intestinal resorption of oral bosentan in neonates.
In the case of imminent RV failure, the (re-) opening of the ductus arteriosus by the use of prostaglandin E1 (PGE1) or even stenting of the persistent ductus arteriosus (PDA) may be considered to decompress the RV, leading to a decrease in SaO2 measured in the lower extremities53 Figure 1 provides a schematic overview over treatment and monitoring measures in the infant with PPHN.

Algorthm with the current recommendations for the diagnosis, monitoring and treatment of persistent pulmonary hypertension of the newborn (PPHN). ^PH needs to be considered when tricuspid regurgitation (TR) jet >2.5m/sec (Echo) and preductal/postductal oxygen saturation differences >10%. ^^https://www.elso.org/Portals/0/IGD/Archive/FileManager/8588d1a580cusersshyerdocumentselsoguidelinesfo rneonatalrespiratoryfailure13.pdf. ECMO, extracorporal membrane oxygenation; iNO, inhaled nitric oxide; PGE1, prostaglandin E1; PPHN, pulmonary hypertension of the newborn; RV, right ventricle; TR, tricuspid regurgitation.
Treatment of chronic PH in BPD/nCLD
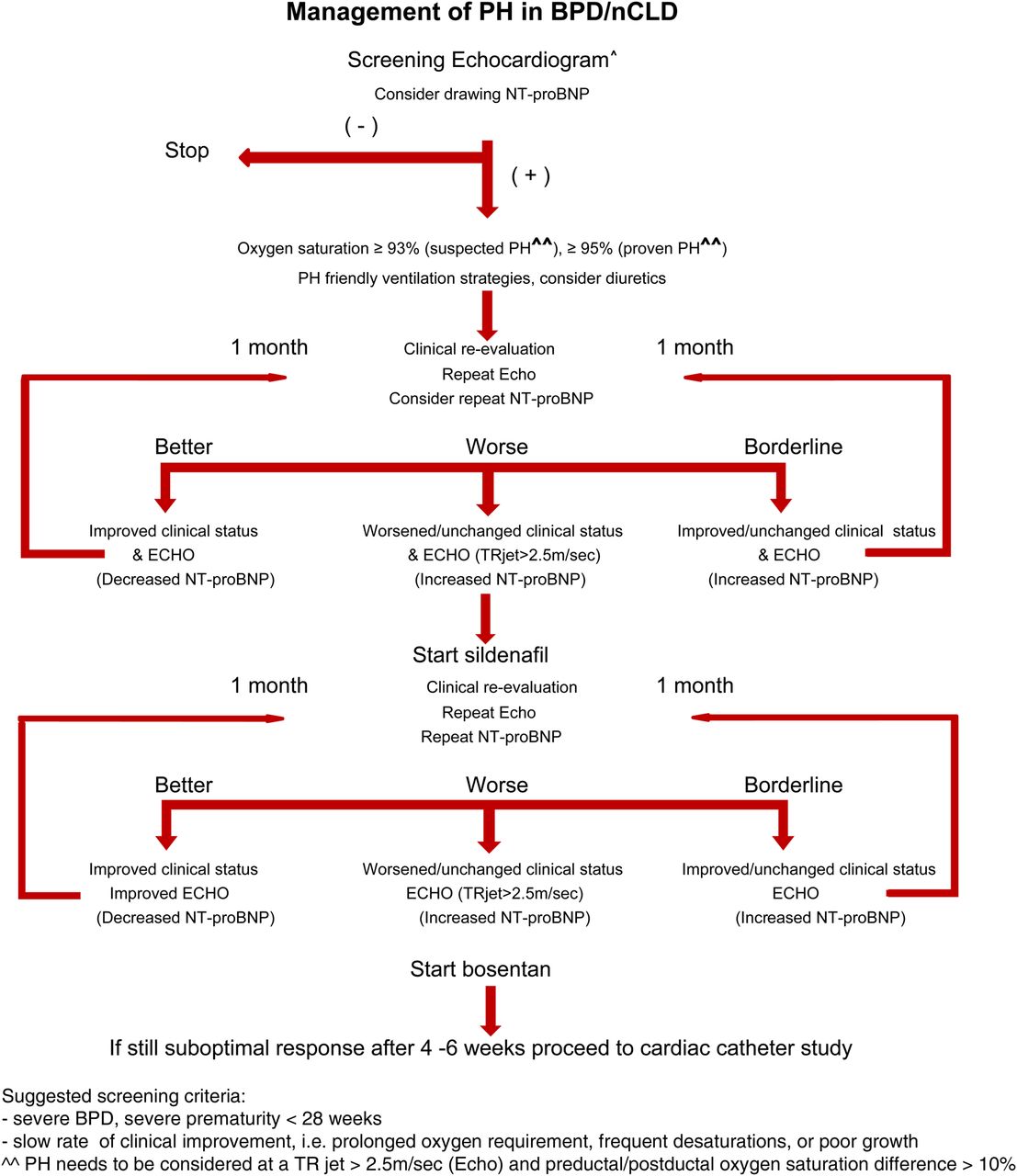
Supplemental oxygen therapy is the common treatment option for PH associated with BPD/nCLD where target systemic arterial oxygen saturation is >93% for all premature infants and >95% for infants with proven PH (figure 2). Serial echocardiograms and cardiac catheterisation is recommended to determine PAP and PVR.4 Atrial or ventricular shunts are not well tolerated in children with nCLD and may be related to the smaller vascular surface area in relation to body size and cardiac output, where a mild increase in pulmonary blood flow may indicate a significant shunt.4
Diuretics
In infants with severe BPD, treatment with diuretics, that is, hydrochlorothiazide and spironolactone can be considered, especially when volume overload is evident.20 ,54 Spironolactone may have additional benefits in neonates and young infants due to mineralocorticoid blockade in RV hypertrophy and PH and can improve lung mechanics in BPD.55
Pulmonary vasodilators/PAH specific medication
Long-term therapy may be considered after careful evaluation and exclusion of associated anomalies such as a left-to-right shunt, left ventricular diastolic dysfunction and pulmonary vein stenosis. However, published data do not provide sufficient evidence to allow for general recommendations. Therefore, careful considerations for the use of targeted therapeutic approaches together with consequent and timely re-evaluations are advised. It has to be noted that all PAH- targeted drugs have to be declared ‘off-label use’ in the neonate and infant with PH associated with BPD/nCLD.
Of the three current potential target pathways for PH treatment in BPD/nCLD, the widest experience is reported for the modulation of the NO signalling pathway with the PDE-5-inhibitor sildenafil. With oral sildenafil, significant improvement of PAP could be demonstrated in children under the age of 2 years with nCLD and PH.56 Intravenous sildenafil may be advantageous in sick infants when enteral bioavailability is unclear. Furthermore, repetitive (or potentially continuous) application of inhaled iloprost can be used in patients with BPD.57–59 As endothelin is a potent pulmonary vasoconstrictor and increased in BPD and hyperoxia,51 ,60 ,61 bosentan treatment may also be considered in PH associated with BPD/nCLD, although only case reports are available for these infants.60 ,62 ,63 ,64
Very potent intravenous vasodilators, such as epoprostenol or treprostinil, can be considered but need to be given through a central venous line (upper body line preferred). Their use may be limited due to the adverse effects with systemic hypotension, potential V/Q mismatch and intrapulmonary right-to-left shunting with consecutive hypoxaemia Figures 1 and 2 provide schematic overviews over treatment and monitoring measures in the infant with PPHN or PH in BPP/NCCD. Over the current recommendations for the treatment of pulmonary hypertension (PH) in chronic lung disease of the preterm and term infant.
{kind=link}
{kind=link}
Algorithm with the current recommendations for the management of pulmonary hypertention in the newborn with bronchopulmonary dysplasia (BPD)/neonatal chronic lung disease (nCLD).
Conclusions
PPHN is a condition in term neonates that may or may not have prenatal origins, and often complicates acute respiratory failure in the first 1–2 weeks after birth. As the course of the disease can be extremely severe, rigorous treatment regimen is mandatory to improve disease outcome. Since iNO and ECMO are effective in the majority of the cases and only limited evidence for the efficacy of oral or intravenous medications for PPHN treatment is available, the importance of any additional, so-called ‘PH specific’ medication in the armamentarium for PH treatment needs to be defined for this patient cohort. In the preterm infant, PH is rare in the first 4 weeks of postnatal life, but may develop along with nCLD, that is, BPD, where vascular dysfunction and alveolar hypoxia perpetuate disease development. Management of PH in developmental lung diseases is mainly focused on the optimisation of systemic oxygenation. Evidence is still lacking for the use of medications available for pulmonary arterial hypertension treatment in the neonatal or former preterm cohort. Thus, a thorough evaluation of PH and its underlying mechanisms is mandatory before targeted PH therapy on a case-by-case basis. Long-term outcome related to PPHN and PH associated with developmental lung diseases remains mostly unknown, pointing to the need for prospective and controlled studies in population-based cohorts.
References
Footnotes
This article is a product of the writing group of the European Paediatric Pulmonary Vascular Disease (PVD) Network (Writing Group Chair: G Hansmann, Writing Group Co-Chair: C. Apitz). DGPK, German Society of Paediatric Cardiology; ISHLT, International Society of Heart and Lung Transplantation.
Funding AH receives grant support from the Helmholtz Gemeinschaft, the Helmholtz Zentrum Muenchen, Germany and the German Center for Lung Research (DZL). CA currently receives grant funding from Stiftung Kinderherz (2511-10-13-001) and Behring-Röntgen-Stiftung (59-0018). DB received grants from the Agence Nationale de la Recherche and from the Fédération Française de Cardiologie. GH currently receives grant support from the German Research Foundation (DFG; HA 4348/2-1), Fördergemeinschaft deutsche Kinderherzzentren (W-H-001-2014), and Stiftung Kinderherz (2511-6-13-011).
This Heart supplement was produced with support from an unrestricted educational grant from Actelion Pharmaceuticals Germany GmbH, Bayer Pharma AG, and Pfizer Inc. None of these organisations had any influence on the composition of the writing group or the content of the articles published in this supplement. Open Access publication of this article was sponsored by Actelion Pharmaceuticals Germany GmbH.
Competing interests DB received fees for consulting, advisory boards and steering committee memberships from Actelion Pharmaceuticals, EliLilly, Pfizer and Bayer.
Provenance and peer review Commissioned; externally peer reviewed.