Article Text

Abstract
Ejection fraction (EF) is a traditional marker of systolic function. However, it may not detect early, subtle cardiac disease with regional predilection. The aim of this study was to define regional intra-ventricular variation in myocardial strain in a cohort of healthy volunteers using Tissue-tracking cardiac magnetic resonance (CMR).
Methods Healthy volunteers were recruited (n = 94, age range 20–79 years, 54% male). CMR at 1.5T was performed. Tissue-tracking software (CVI42, Circle Cardiovascular Imaging Inc.) estimated myocardial strain from the long-axis and the short-axis steady-state free precession (SSFP) cine images (Figure 1). The entire cohort was analysed by two independent readers. Inter-observer variability was also assessed. Myocardial segments were defined in accordance to the American Heart Association 16-segment model. Regional variations in circumferential and radial strain between basal, mid-cavity and apical segments as well as between left ventricle walls were assessed. Statistical analysis was performed using paired t test (p < 0.05).
Results Inter-observer reproducibility analyses were excellent for mid-cavity and apical radial and circumferential strain values. On the other hand, reproducibility was not as good for basal segments for both deformation directions. Regional variations in strain (Table 1) revealed a statistically significant increase in deformation of the apical segments compared to the basal and mid-cavity ones for both radial and circumferential strain. Analysis of the different LV walls deformations indicated lowest values in the septum in all subjects, as well as across all age and gender subgroups.
Conclusion This is the first study to demonstrate that there is a positive gradient toward the apex in both circumferential and radial strain using CMR-derived myocardial strain analysis. Furthermore, we also showed that the interventricular septum is the segment with lowest deformation values. These findings are important, as a comprehensive understanding of normal intra-ventricular regional variation is needed before this new tool can be implemented in routine clinical practice.
Regional strain values
{kind=link}
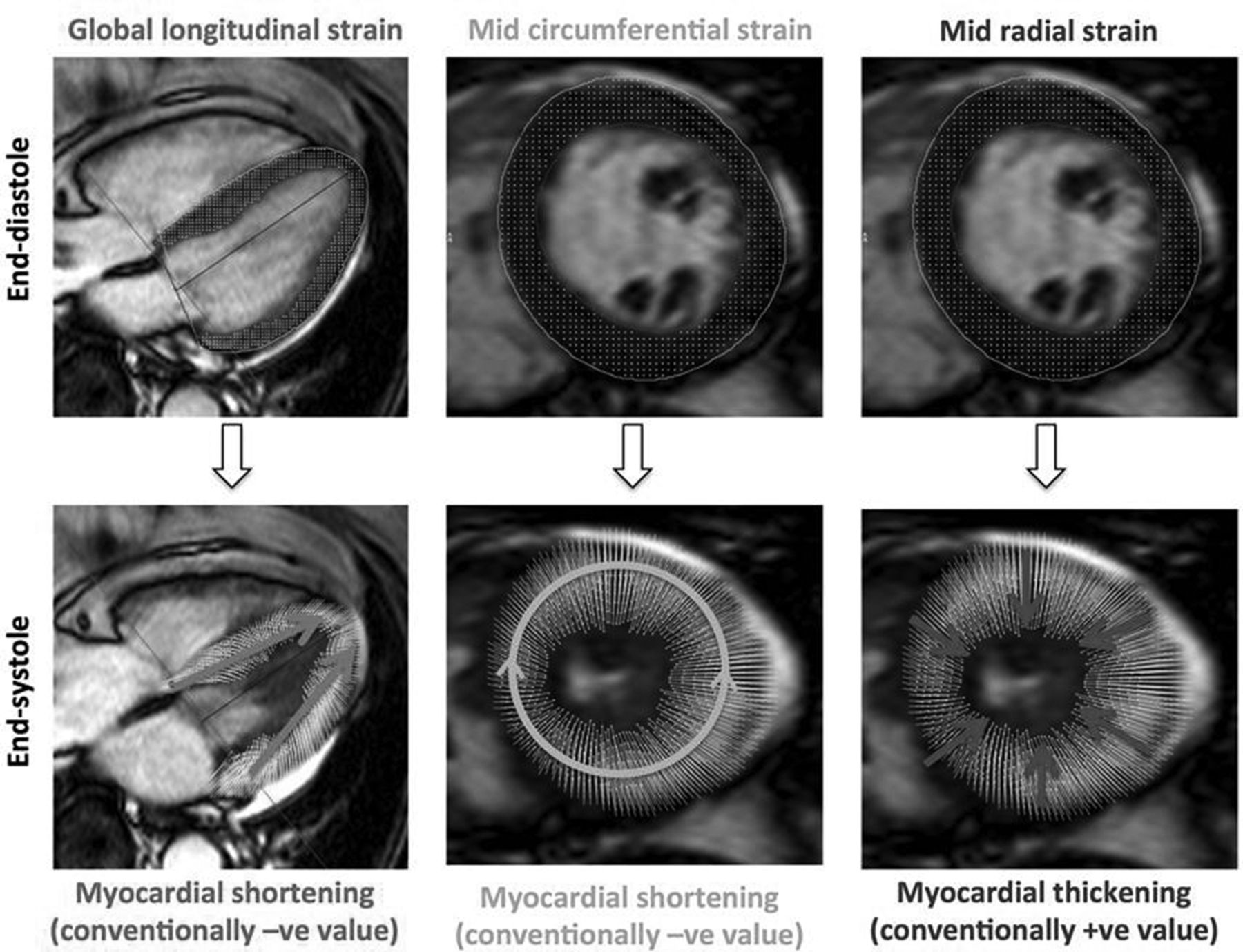
Definition of longitudinal, circumferential and radial myocardial strain, calculated by SSFP long-axis and short-axis cine images